 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 33(3); 2020 > Article
- Review Article Current Concepts in the Articular Cartilage Repair
- Eui Dong Yeo, Whi Je Cho, Young Koo Lee
-
Journal of Musculoskeletal Trauma 2020;33(3):164-170.
DOI: https://doi.org/10.12671/jkfs.2020.33.3.164
Published online: July 31, 2020
1Department of Orthopedic Surgery, VHS Medical Center, Seoul, Korea
2Department of Orthopedic Surgery, Soonchunhyang University Hospital Bucheon, Bucheon, Korea
2Department of Orthopedic Surgery, Soonchunhyang University Hospital Bucheon, Bucheon, Korea
- 1,072 Views
- 3 Download
- 0 Crossref
- 0 Scopus
Abstract
Articular cartilage defects are common in orthopedic practice. Most clinical and research efforts focus on restoring the damaged cartilage in connection with osteoarthritis or trauma. This article explains the current clinical approaches for repairing cartilage, as well as the research approaches and those under translation into clinical practice. Tissue engineering techniques are being employed with aims of repopulating a cartilage defect with hyaline cartilage containing living chondrocytes with hopes of improving the clinical outcomes. Cartilage tissue engineering involves the cell source, biomaterial and membranes, and growth stimulators. Tissue engineering is being applied to clinical medicine by autologous chondrocyte implantation or similar techniques. While basic science has refined orthopedic treatment of chondral lesions, available evidence does not conclude the superiority of tissue engineering methods over other techniques in improving the clinical symptoms or restoring the native joint mechanics.
J Korean Fract Soc. 2020 Jul;33(3):164-170. Korean.
Published online Jul 24, 2020.
https://doi.org/10.12671/jkfs.2020.33.3.164
Published online Jul 24, 2020.
https://doi.org/10.12671/jkfs.2020.33.3.164
Copyright © 2020 The Korean Fracture Society. All rights reserved.
Review
Current Concepts in the Articular Cartilage Repair

Abstract
Articular cartilage defects are common in orthopedic practice. Most clinical and research efforts focus on restoring the damaged cartilage in connection with osteoarthritis or trauma. This article explains the current clinical approaches for repairing cartilage, as well as the research approaches and those under translation into clinical practice. Tissue engineering techniques are being employed with aims of repopulating a cartilage defect with hyaline cartilage containing living chondrocytes with hopes of improving the clinical outcomes. Cartilage tissue engineering involves the cell source, biomaterial and membranes, and growth stimulators. Tissue engineering is being applied to clinical medicine by autologous chondrocyte implantation or similar techniques. While basic science has refined orthopedic treatment of chondral lesions, available evidence does not conclude the superiority of tissue engineering methods over other techniques in improving the clinical symptoms or restoring the native joint mechanics.
Keywords
Cartilage, Tissue engineering, Chondrocyte
Figures
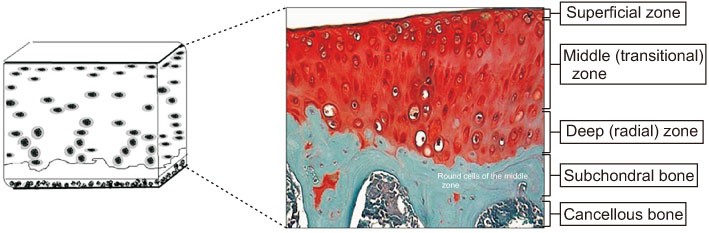
Fig. 1
Articular cartilage.
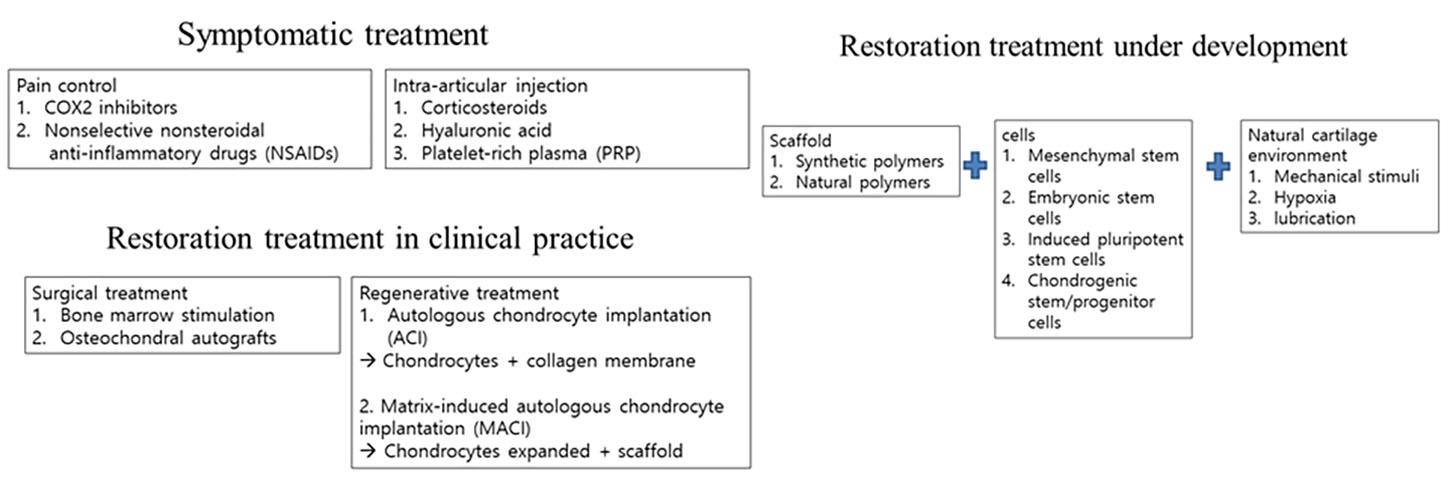
Fig. 2
Approaches to the restoration of cartilage.
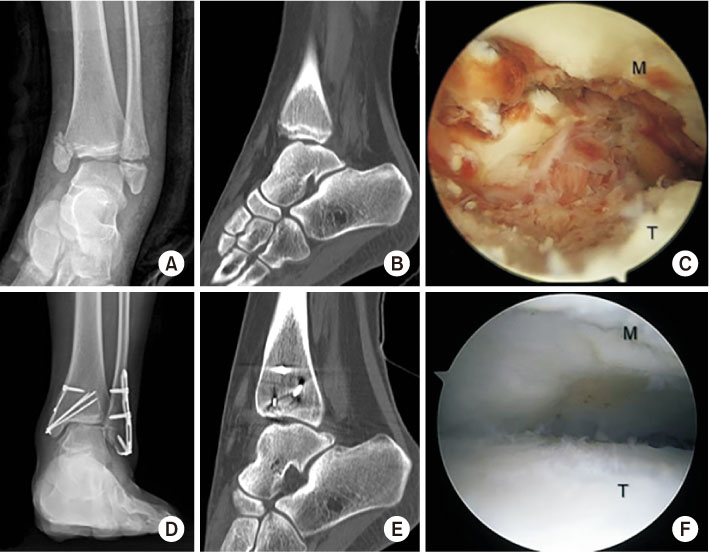
Fig. 3
Female, 12 years old, injured bimalleolar fracture and large osteochondral lesion of the talus on anteromedial talar dome. (A) Preoperative anteroposterior radiography. (B) Preoperative computed tomography (CT). (C) Intraoperative arthroscopy showed traumatic large osteochondral lesion of the talus. (D) Postoperative 8-month anteroposterior radiography. (E) Postoperative 8-month CT. (F) Postoperative 8-month second look arthroscopy showed a well-healed osteochondral lesion of the talus. M: medial malleolus, T: talus.
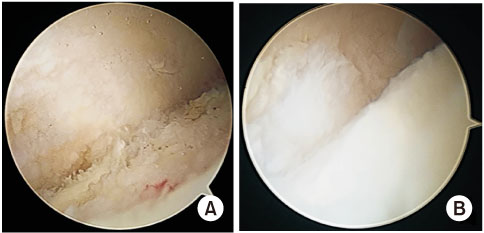
Fig. 4
Preoperative and postoperative photos of the patient undergoing microfracture for an osteochondral lesion of the talus. (A) Preoperative photo. (B) Postoperative photo.
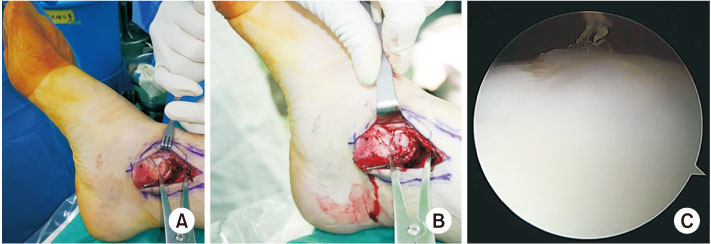
Fig. 5
Intraoperative and postoperative photographs of the osteochondral lesion with a talus cyst undergoing osteochondral autograft transplantation. (A) Photograph of osteochondral lesion of talus identification during operation. (B) Photograph of inserting a cylindrical plug during operation. (C) Arthroscopic photograph when removing metal implants.
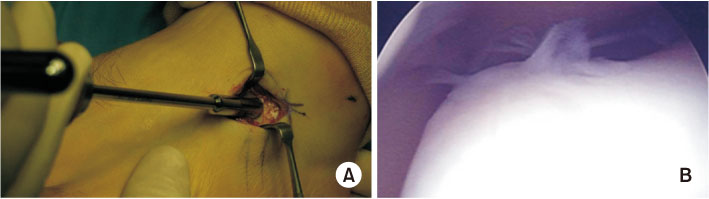
Fig. 6
Autologous chondrocyte implantation (ACI) operation. (A) Cartilage harvesting from the anterior process of the calcaneus. (B) Complete repair and filling of the defect, complete integration to the border zone when performing 2nd look arthroscopy after ACI of osteochondral lesion of the talus.
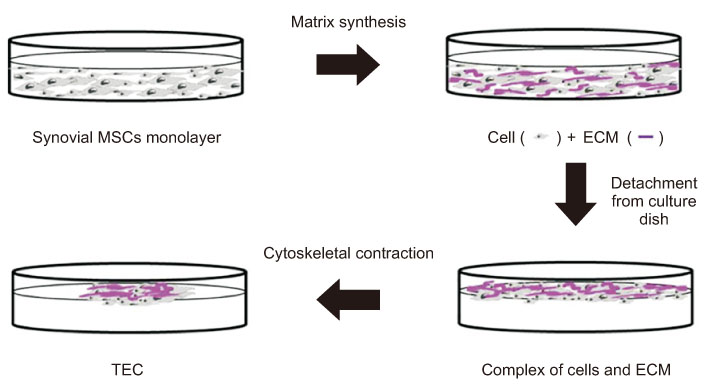
Fig. 7
Schematic representation of tissueengineered construct (TEC) development.
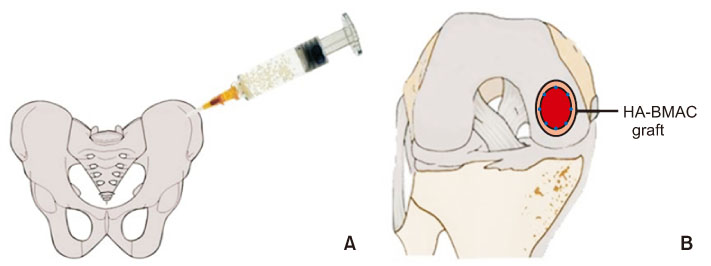
Fig. 8
Cartilage repair in the knee with a hyaluronic acid-based scaffold embedded with bone marrow aspirate concentrate (HA-BMAC). (A) Bone marrow aspirate. (B) HA-BMAC implanted into the chondral defect.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Mithoefer K. Complex articular cartilage restoration. Sports Med Arthrosc Rev 2013;21:31–37.
-
-
Heinegård D. Fell-Muir Lecture: proteoglycans and more--from molecules to biology. Int J Exp Pathol 2009;90:575–586.
-
-
Buckwalter JA, Mankin HJ. Articular cartilage: degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487–504.
-
-
Allan KS, Pilliar RM, Wang J, Grynpas MD, Kandel RA. Formation of biphasic constructs containing cartilage with a calcified zone interface. Tissue Eng 2007;13:167–177.
-
-
Williamson AK, Chen AC, Masuda K, Thonar EJ, Sah RL. Tensile mechanical properties of bovine articular cartilage: variations with growth and relationships to collagen network components. J Orthop Res 2003;21:872–880.
-
-
Williamson AK, Chen AC, Sah RL. Compressive properties and function-composition relationships of developing bovine articular cartilage. J Orthop Res 2001;19:1113–1121.
-
-
Hunziker EB. Articular cartilage repair: basic science and clinical progress. A review of the current status and prospects. Osteoarthritis Cartilage 2002;10:432–463.
-
-
Widuchowski W, Lukasik P, Kwiatkowski G, et al. Isolated full thickness chondral injuries. Prevalance and outcome of treatment. A retrospective study of 5233 knee arthroscopies. Acta Chir Orthop Traumatol Cech 2008;75:382–386.
-
-
Bedi A, Feeley BT, Williams RJ 3rd. Management of articular cartilage defects of the knee. J Bone Joint Surg Am 2010;92:994–1009.
-
-
Medvedeva EV, Grebenik EA, Gornostaeva SN, et al. Repair of damaged articular cartilage: current approaches and future directions. Int J Mol Sci 2018;19:2366
-
-
Horisberger M, Valderrabano V, Hintermann B. Posttraumatic ankle osteoarthritis after ankle-related fractures. J Orthop Trauma 2009;23:60–67.
-
-
Aktas S, Kocaoglu B, Gereli A, Nalbantodlu U, Güven O. Incidence of chondral lesions of talar dome in ankle fracture types. Foot Ankle Int 2008;29:287–292.
-
-
Nwankwo EC Jr, Labaran LA, Athas V, Olson S, Adams SB. Pathogenesis of posttraumatic osteoarthritis of the ankle. Orthop Clin North Am 2019;50:529–537.
-
-
Franke O, Durst K, Maier V, et al. Mechanical properties of hyaline and repair cartilage studied by nanoindentation. Acta Biomater 2007;3:873–881.
-
-
Widuchowski W, Widuchowski J, Trzaska T. Articular cartilage defects: study of 25,124 knee arthroscopies. Knee 2007;14:177–182.
-
-
Williams SK, Amiel D, Ball ST, et al. Prolonged storage effects on the articular cartilage of fresh human osteochondral allografts. J Bone Joint Surg Am 2003;85:2111–2120.
-
-
Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889–895.
-
-
Lee KT, Choi YS, Lee YK, Cha SD, Koo HM. Comparison of MRI and arthroscopy in modified MOCART scoring system after autologous chondrocyte implantation for osteochondral lesion of the talus. Orthopedics 2011;34:e356–e362.
-
-
Lee KT, Choi YS, Lee YK, Cha SD, Koo HM. Comparison of MRI and arthroscopy after autologous chondrocyte implantation in patients with osteochondral lesion of the talus. Orthopedics. 2011 [doi: 10.3928/01477447-20110627-10][epub].
-
-
Hettrich CM, Crawford D, Rodeo SA. Cartilage repair: third-generation cell-based technologies--basic science, surgical techniques, clinical outcomes. Sports Med Arthrosc Rev 2008;16:230–235.
-
-
Pittenger MF, Mackay AM, Beck SC, et al. Multilineage potential of adult human mesenchymal stem cells. Science 1999;284:143–147.
-
-
Dominici M, Le Blanc K, Mueller I, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006;8:315–317.
-
-
Toh WS, Foldager CB, Pei M, Hui JH. Advances in mesenchymal stem cell-based strategies for cartilage repair and regeneration. Stem Cell Rev Rep 2014;10:686–696.
-
-
Aicher WK, Bühring HJ, Hart M, Rolauffs B, Badke A, Klein G. Regeneration of cartilage and bone by defined subsets of mesenchymal stromal cells--potential and pitfalls. Adv Drug Deliv Rev 2011;63:342–351.
-
-
Wakitani S, Okabe T, Horibe S, et al. Safety of autologous bone marrow-derived mesenchymal stem cell transplantation for cartilage repair in 41 patients with 45 joints followed for up to 11 years and 5 months. J Tissue Eng Regen Med 2011;5:146–150.
-
-
Thomson JA, Itskovitz-Eldor J, Shapiro SS, et al. Embryonic stem cell lines derived from human blastocysts. Science 1998;282:1145–1147.
-
-
Hwang NS, Varghese S, Lee HJ, et al. In vivo commitment and functional tissue regeneration using human embryonic stem cell-derived mesenchymal cells. Proc Natl Acad Sci U S A 2008;105:20641–20646.
-
-
Toh WS, Yang Z, Liu H, Heng BC, Lee EH, Cao T. Effects of culture conditions and bone morphogenetic protein 2 on extent of chondrogenesis from human embryonic stem cells. Stem Cells 2007;25:950–960.
-
-
Toh WS, Lee EH, Cao T. Potential of human embryonic stem cells in cartilage tissue engineering and regenerative medicine. Stem Cell Rev Rep 2011;7:544–559.
-
-
Gille J, Behrens P, Volpi P, et al. Outcome of Autologous Matrix Induced Chondrogenesis (AMIC) in cartilage knee surgery: data of the AMIC Registry. Arch Orthop Trauma Surg 2013;133:87–93.
-
-
Marcacci M, Berruto M, Brocchetta D, et al. Articular cartilage engineering with Hyalograft C: 3-year clinical results. Clin Orthop Relat Res 2005;(435):96–105.
-
-
Crawford DC, Heveran CM, Cannon WD Jr, Foo LF, Potter HG. An autologous cartilage tissue implant NeoCart for treatment of grade III chondral injury to the distal femur: prospective clinical safety trial at 2 years. Am J Sports Med 2009;37:1334–1343.
-
-
Spiller KL, Maher SA, Lowman AM. Hydrogels for the repair of articular cartilage defects. Tissue Eng Part B Rev 2011;17:281–299.
-
-
Fortier LA, Barker JU, Strauss EJ, McCarrel TM, Cole BJ. The role of growth factors in cartilage repair. Clin Orthop Relat Res 2011;469:2706–2715.
-
-
Harris JD, Siston RA, Pan X, Flanigan DC. Autologous chondrocyte implantation: a systematic review. J Bone Joint Surg Am 2010;92:2220–2233.
-
-
Clar C, Cummins E, McIntyre L, et al. Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation. Health Technol Assess 2005;9:iii–iv. ix–x, 1–82.
-
-
Vasiliadis HS, Lindahl A, Georgoulis AD, Peterson L. Malalignment and cartilage lesions in the patellofemoral joint treated with autologous chondrocyte implantation. Knee Surg Sports Traumatol Arthrosc 2011;19:452–457.
-
-
Vavken P, Samartzis D. Effectiveness of autologous chondrocyte implantation in cartilage repair of the knee: a systematic review of controlled trials. Osteoarthritis Cartilage 2010;18:857–863.
-
-
Harris JD, Siston RA, Brophy RH, Lattermann C, Carey JL, Flanigan DC. Failures, re-operations, and complications after autologous chondrocyte implantation--a systematic review. Osteoarthritis Cartilage 2011;19:779–791.
-
 Cite
Cite
