 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(3); 2026 > Article
-
Review Article
- Current concepts and applications of internal fixation for forearm diaphyseal fractures
- Sung Yoon Jung1, Min Kyun Cho1, Dong-hee Kim2, Sang Hyun Lee3
-
Journal of Musculoskeletal Trauma 2026;39(3):205-215.
DOI: https://doi.org/10.12671/jmt.2026.00087
Published online: July 3, 2026
1Department of Orthopedic Surgery, Dong-A University Hospital, Dong-A University School of Medicine, Busan, Korea
2Department of Orthopedic Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
3Department of Orthopedic Surgery, Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
- Correspondence to: Sang Hyun Lee Department of Orthopedic Surgery, Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Pusan 49241, Korea Tel: +82-51-240-8718 Email: handsurgeon@pusan.ac.kr
• Received: January 30, 2026 • Revised: May 8, 2026 • Accepted: May 11, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 224 Views
- 6 Download
Abstract
- Adult diaphyseal fractures of the forearm functionally behave as intra-articular injuries because forearm rotation depends on accurate restoration of length, axial alignment, rotation, and the native radial bow. This narrative review summarizes contemporary surgical options for adult forearm shaft fractures, including 3.5-mm plate osteosynthesis, dual mini-plate fixation, interlocking intramedullary nailing, and minimally invasive plate osteosynthesis (MIPO). Compression plating with 3.5-mm plates remains the reference standard for most fracture patterns, whereas other techniques should be regarded as selective, emerging, or salvage options according to their indication spectrum and evidence base. Mini-fragment dual plating may be useful for short segments or thin soft-tissue envelopes, although the supporting clinical evidence remains limited and meticulous biomechanical execution is essential. Interlocking intramedullary nailing is a viable alternative for carefully selected simple fracture patterns or soft-tissue-compromised situations, offering less invasive exposure but a narrower indication spectrum. MIPO may be considered for selected comminuted or soft-tissue-compromised diaphyseal fractures; however, its use in adult forearm fractures remains constrained by the high functional requirement for precise restoration of length, rotation, and the radial bow. To improve transparency, this review explicitly distinguishes established, evidence-supported methods from techniques supported mainly by limited retrospective data or institutional experience. A pattern-based pragmatic algorithm and expanded comparison table are provided to guide fixation selection according to the bone involved, fracture location, fracture morphology, soft-tissue condition, and evidence tier while minimizing complications such as nonunion, infection, nerve injury, refracture after plate removal, and radioulnar synostosis.
Introduction
Forearm diaphyseal fractures disrupt the radius-ulna unit, a functional ring whose coordinated rotation enables pronation-supination and positions the hand in space. A classic cadaveric biomechanical study about the biomechanics of forearm diaphysis stated that small errors in length, rotation, or the magnitude and location of the radial bow translate directly into motion loss and anatomical reduction is necessary in forearm diaphyseal fractures [1]. Several studies demonstrated clinically important reductions in forearm rotation with angular and rotational deformity and showed that restoration of the native radial bow correlates with functional recovery after fixation [1-3]. These biomechanical imperatives underpin contemporary surgical goals: accurate restoration of length and rotation, anatomic recreation of the radial bow (particularly in the radius), stable fixation matched to fracture morphology, and early motion. These biomechanical demands explain why forearm fracture fixation demands substantial rigidity and precise anatomical restoration for full pronation-supination, which clarifies the functional rationale for treatment selection for non-specialist readers. Open reduction and internal fixation using small-fragment plates has historically been the standard for adult both-bone forearm fractures. Landmark series reported high union rates and satisfactory motion with compression plating, and later cohort studies reinforced plating as the benchmark against which alternatives are compared [4-7]. Locking compression plates (LCP) are widely used; however, comparative series suggest broadly similar union and function between LCP and nonlocking compression plates when interfragmentary compression principles are respected [8-10]. Conversely, purely locking, noncompressive constructs may increase nonunion risk in some settings, underscoring that compression across simple fracture lines remains more important than plate technology itself. Interest in lower-profile implants and biologic fixation has expanded the contemporary armamentarium. Mini-fragment dual plating aims to reduce implant prominence and facilitate fixation in short segments or narrow corridors, but evidence remains limited and technique sensitivity is high [11,12]. Interlocking intramedullary (IM) nails have evolved to improve rotational and length control compared with historical flexible pins, and may be considered in selected simple patterns or soft-tissue-compromised situations, although recreating the radial bow—especially in the radius—remains challenging [13-21]. Selective application of minimally invasive plate osteosynthesis (MIPO) has also been reported for diaphyseal forearm fractures in comminuted patterns or compromised soft tissue; nonetheless, the forearm's high functional demand yields limited tolerance for malrotation or inadequate radial bow restoration [21]. In previous literature, “hybrid fixation” of the forearm typically refers to using different implant types in different bones (e.g., plating the radius and nailing the ulna). In contrast, placing a plate over an IM nail within the same bone is best termed a nail-plate construct (NPC) and should be viewed as a rare salvage strategy with limited supporting evidence. This review compares contemporary fixation options—3.5-mm plating, mini-fragment dual plating, interlocking IM nailing, selective MIPO, NPC, and wiring-assisted plating—integrating indications, technical pearls, outcomes, limitations, and complication avoidance. A practical, pattern-based decision algorithm is proposed to assist operative strategy selection.
This study was a narrative review and did not require institutional review board approval. Informed consent was obtained for publication of clinical images.
Literature search strategy
This narrative review was informed by a structured search of PubMed/MEDLINE, Embase, Scopus, Google Scholar, and the Cochrane Central Register of Controlled Trials (CENTRAL), covering from inception through December 2025. Search terms included combinations of: “adult forearm fracture,” “both-bone forearm fracture,” “diaphyseal radius fracture,” “diaphyseal ulna fracture,” “plate fixation,” “locking compression plate,” “dynamic compression plate,” “mini-plate,” “2.7 mm plate,” “intramedullary nail,” “interlocking nail,” “MIPO forearm,” “radial bow,” “radioulnar synostosis,” and “refracture plate removal.” Priority was given to adult clinical studies, comparative cohorts, systematic reviews/meta-analyses, and biomechanical studies directly relevant to fixation stability. Pediatric populations, metaphyseal-only fracture studies, isolated case reports lacking transferable technical relevance, and non-English reports with equivalent English evidence were excluded. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-style flow diagram was added to enhance transparency regarding screening and inclusion (Fig. 1). In this review framework, 312 records were identified, 74 duplicates were removed, 238 titles/abstracts were screened, 54 full-text reports were assessed, and 25 studies were included in the final narrative synthesis.
Surgical options and techniques
Indications
Plate fixation using 3.5-mm systems remains the reference standard for most adult forearm diaphyseal fractures, including the majority of simple and wedge patterns (AO/OTA 22-A/B) and many complex patterns (22-C) that permit anatomic reconstruction [4-7]. In both-bone injuries, plating is particularly advantageous because it most reliably enables restoration of length, rotational alignment, and the native radial bow, which is a critical determinant of functional recovery [1-3].
Key technical points
From a technical standpoint, separate surgical approaches to the radius and ulna are generally preferred to protect the interosseous membrane and mitigate the risk of radioulnar synostosis [22]. In many cases, the ulna is addressed first to re-establish length and serve as a template, after which the radius is reduced and contoured to restore both the magnitude and apex location of the radial bow (Fig. 2) [1-3]. For simple fracture lines, interfragmentary compression and absolute stability should be prioritized. Adequate fixation typically requires at least three bicortical screws (≥6 cortices) in each main fragment with an appropriate working length [7,9]. During proximal radial exposure and drilling through anterior (Henry approach), meticulous protection of the posterior interosseous nerve (PIN) is essential, including full supination and careful dissection.
Clinical outcomes
Large clinical series have consistently demonstrated high union rates and reliable functional recovery when anatomic and biomechanical principles are respected [4-7].
Level of evidence
Overall, the evidence supporting 3.5-mm plating is the strongest among available techniques, consisting of multiple foundational and contemporary cohort studies [4-7].
Indications
Mini-fragment dual plating has been introduced as a lower-profile strategy intended to reduce implant prominence and facilitate fixation in anatomically constrained corridors. In adult forearm diaphyseal fractures, this approach may be considered selectively in short proximal radius segments where achieving secure purchase with a single 3.5-mm plate is difficult, in patients with thin soft-tissue envelopes at risk for symptomatic prominence, or in peri-articular/metaphyseal-diaphyseal junctional extensions [11,12].
Key technical points
Mechanically, dual-plate constructs—often arranged orthogonally—can distribute screw density and improve torsional resistance while maintaining a lower profile (Fig. 3) [11,12]. Similarly, during the anterior approach for proximal radial fractures, drilling beyond the far cortex can endanger the PIN. In that case, orthogonal dual-plate fixation with unicortical screws can avoid this complication.
Clinical outcomes and limitations
Biomechanical studies suggest that well-executed 2.7-mm constructs can approach the stability of 3.5-mm plating in selected patterns [11,12,23]. Nevertheless, the clinical evidence base is smaller and heterogeneous. This technique should be clearly framed as a selective or emerging option rather than equivalent to standard 3.5-mm plating. Risks include mechanical insufficiency, loss of alignment, and nonunion when stability principles are compromised [11,12].
Level of evidence
The evidence supporting mini-fragment dual plating is limited, consisting primarily of small retrospective series and biomechanical studies [11,12,23].
Indications
Modern interlocking IM nails have evolved to improve rotational and length control compared with historical flexible pins and may offer advantages of smaller incisions and reduced periosteal stripping [13-18]. In adult forearm diaphyseal fractures, interlocking IM nailing can be considered selectively for simple transverse or short-oblique patterns where rotational control and length restoration can be reliably achieved. It may also be attractive in soft-tissue-compromised situations (including selected open injuries after adequate debridement) and in selected polytrauma scenarios where minimizing operative time and dissection is desirable [13-21].
Situations to avoid or use with caution
Despite these potential benefits, indications are constrained by the forearm's unique functional demand—particularly the need to recreate the radial bow and avoid rotational malalignment.
Key technical points
Technically, accurate entry point selection and high-quality reduction are essential, and rotational alignment and length should be confirmed intraoperatively using fluoroscopy with the shoulder abducted and elbow flexed to 90°, comparing with the contralateral limb. Even with multiplanar interlocking, bow recreation in the radius is often less predictable than with plating, and this limitation should be explicitly acknowledged when counseling patients and selecting cases (Fig. 4). Intraoperative strategies to mitigate malalignment include careful fluoroscopic assessment of the radial bow profile in the anteroposterior view, provisional reduction with external manipulation or pointed reduction forceps, and confirmation of rotational alignment by comparing cortical thickness patterns with the contralateral side.
Clinical outcomes
Systematic reviews and comparative series suggest that interlocking IM nails can achieve union with acceptable complication profiles in carefully selected indications, sometimes with shorter operative time, although high-quality randomized data remain limited [14-16].
Level of evidence
Moderate evidence base consisting of systematic reviews, meta-analyses, and comparative cohort studies [13-16].
Terminology clarification
Terminology in this area requires precision. In established orthopedic trauma usage, “hybrid fixation” generally refers to applying different implant types to different bones (e.g., plating the radius and nailing the ulna). In contrast, applying a plate over an IM nail within the same bone is best termed an NPC and should be framed as a rare salvage strategy with limited supporting evidence.
Indications
NPC may be considered in exceptional situations such as severe comminution or revision nonunion where long-span plating alone is judged biologically or mechanically unfavorable, or in selected atypical ulnar fractures requiring additional internal support and load sharing.
Key technical points and limitations
However, the technique carries important hazards. Bicortical screw purchase around a nail within the narrow ulnar canal can be technically demanding and may risk screw-nail interference, iatrogenic fracture, or compromised fixation if executed improperly. For these reasons, NPC should not be presented as a routine alternative to standard plating. In typical execution, a prebent flexible nail is inserted—commonly via proximal ulnar/olecranon entry—to provide internal support and load sharing, after which a plate is applied to provide rotational and bending stability (Fig. 5). Variable-angle locking may facilitate screw placement around the nail, and cancellous grafting may be considered in revision nonunion settings according to biological risk.
Level of evidence
Overall, published clinical evidence remains limited, and NPC should be reserved for carefully selected salvage indications rather than generalized indications. Statements based on institutional experience should be clearly distinguished from evidence-based conclusions.
Indications
Simple transverse diaphyseal fractures require absolute stability, yet do not reliably permit interfragmentary lag-screw compression in the same manner as oblique patterns. In selected transverse diaphyseal fractures where lag-screw fixation is not feasible and maintaining compression during plating is challenging, transosseous wiring may serve as an adjunct to facilitate interfragmentary compression and reduction control [24].
Key technical points and limitations
This technique should be explicitly framed as adjunctive only and should not be used as standalone definitive fixation in adult diaphyseal forearm fractures (Fig. 6).
Clinical outcomes and level of evidence
Evidence supporting this method remains limited to small retrospective reports [24]. The main value of wiring is as a technical adjunct to achieve compression and maintain reduction during plating, rather than as an independent fixation strategy. This technique represents an application of principles from the authors' institutional experience and should be used judiciously in appropriately selected cases.
Indications
MIPO aims to preserve fracture biology via indirect reduction and bridge-plating principles while providing relative stability. In adult forearm diaphyseal fractures, its role remains selective because the forearm has limited tolerance for malrotation or inadequate radial bow restoration, particularly in the radius [21]. MIPO may be considered in comminuted or segmental diaphyseal fractures where bridge-plating principles are appropriate, and in soft-tissue-compromised situations including selected open injuries after adequate debridement (Fig. 7) [21].
Situations to avoid or use with caution
Conversely, MIPO should be avoided or used with extreme caution in the following situations: simple fractures where compression and absolute stability are required; cases where acceptable restoration of rotational alignment and radial bow cannot be confidently achieved by indirect means—especially in radius fractures; early learning curve cases without reliable fluoroscopic reduction control; and proximal third radius fractures with high risk of rotational malalignment.
Key technical points
Key technical considerations include meticulous intraoperative assessment of length, rotation, and overall alignment, with explicit confirmation that the radius demonstrates an acceptable radial bow restoration under fluoroscopy (Fig. 7). Specific intraoperative strategies to mitigate malalignment include: (1) use of external distractor or manual traction to restore length, (2) fluoroscopic comparison of radial bow with contralateral side, (3) assessment of rotational alignment by comparing cortical symmetry, (4) judicious use of percutaneous pointed reduction forceps, (5) careful screw placement with heightened awareness of PIN risk during proximal radius fixation.
Clinical outcomes and limitations
Clinical series suggest that union can be achieved at rates comparable to open plating in carefully selected patterns, but the evidence base remains limited and largely retrospective [21].
Level of evidence
Limited evidence base consisting primarily of retrospective comparative studies [21].
Taken together, these six fixation strategies illustrate the spectrum of contemporary approaches to adult forearm diaphyseal fractures, each with distinct indications, strengths, and limitations. A comparative overview of these techniques is provided in Table 1 [4-7,11-16,21,24,25].
Complications and avoidance
Complications following operative management of adult forearm diaphyseal fractures are strongly influenced by mechanical execution and soft-tissue condition. Nonunion or delayed union is multifactorial, reflecting biological compromise, instability, and patient factors. Reported rates of nonunion after plate fixation range from 2% to 10% in large series [6,7]. Infection rates range from 1% to 6%, implant prominence or irritation from 10% to 30%, radioulnar synostosis from 2% to 6%, nerve injury from 1% to 5%, and refracture after plate removal from 4% to 12% [6,7,22,25]. These complication rates provide a unified risk-benefit framework across techniques.
Pattern-based practical algorithm
A pattern-based decision algorithm is proposed to assist selection of fixation strategies according to the bone involved, fracture morphology, fracture location, and soft-tissue condition. The primary objective is restoration of forearm function through accurate reconstruction of length, rotational alignment, and, particularly in radius fractures, the native radial bow (Fig. 8).
The algorithm incorporates six techniques—3.5-mm plating, mini-fragment dual plating, interlocking IM nailing, NPC, transosseous wiring-assisted plating, and MIPO—and to incorporate fracture pattern, bone quality, soft-tissue condition, and surgeon experience rather than generic branching alone.
Conclusions
Regardless of implant selection, successful treatment of adult forearm diaphyseal fractures fundamentally depends on accurate restoration of length, rotation, axial alignment, and—particularly for the radius—the native radial bow. Compression plate osteosynthesis using 3.5-mm plates remains the most dependable treatment for adult diaphyseal forearm fractures because it most reliably restores anatomy and provides stable fixation across a wide range of patterns.
Contemporary alternatives—including mini-fragment dual plating, interlocking IM nailing, MIPO, transosseous wiring-assisted plating, and rare NPCs—may broaden options in carefully selected scenarios, but their indications are narrower and their evidence base is generally more limited. These techniques should be clearly presented as selective, emerging, adjunctive, or salvage options, and claims regarding their efficacy should be calibrated to the available evidence.
-
Author contributions
Conceptualization: SYJ, DK. Data curation: SYJ. Formal analysis: MKC, DK, SHL. Supervision: SHL. Writing–original draft: SYJ, MKC. Writing–review & editing: MKC, DK, SHL. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.

PRISMA-style flow diagram showing literature identification, screening, eligibility assessment, and study inclusion for this narrative review.
Fig. 2.

A 40-year-old male patient with a radial shaft fracture. (A) Preoperative anteroposterior and lateral radiographs demonstrating a diaphyseal radial fracture. (B) Immediate postoperative radiographs after open reduction and internal fixation using a 3.5-mm plate.
Fig. 3.

A 62-year-old male patient with a radial shaft fracture. (A) Preoperative anteroposterior and lateral radiographs showing a diaphyseal radial fracture. (B) Immediate postoperative radiographs after mini-fragment dual plating with 2.4–2.7-mm plates.
Fig. 4.

A 38-year-old male patient with both-bone forearm shaft fractures treated with interlocking intramedullary nailing. (A) Preoperative radiographs. (B) Immediate postoperative radiographs after interlocking intramedullary nail fixation.
Fig. 5.

A 65-year-old female patient with established nonunion after prior ulnar fixation. (A) Preoperative radiographs. (B) Immediate postoperative radiographs after revision fixation using a nail-plate construct.
Fig. 6.

A 63-year-old male patient. Immediate postoperative (A) anteroposterior and (B) lateral radiographs after transosseous wiring-assisted plate fixation.
Fig. 7.

A 43-year-old female patient with a comminuted radial shaft fracture treated with minimally invasive plate osteosynthesis. (A) Preoperative radiographs. (B) Intraoperative clinical photograph demonstrating external distractor-assisted indirect reduction. (C) Immediate postoperative radiographs after bridge plating using minimally invasive plate osteosynthesis.
Fig. 8.

Pattern-based decision-tree flowchart for fixation selection in adult forearm diaphyseal fractures, incorporating the bone involved (radius vs. ulna), fracture location (proximal, middle, or distal third), fracture morphology, and explicit contraindications. MIPO, minimally invasive plate osteosynthesis; IM, intramedullary; NPC, nail-plate construct.
Table 1.
Summary of fixation techniques for adult forearm diaphyseal fractures
| Technique | Best indications | Key advantages | Primary caveats | Evidence tier/quantitative note |
|---|---|---|---|---|
| 3.5-mm LCP plating | Simple or wedge diaphyseal patterns; most both-bone fractures; cases requiring precise restoration of the radial bow | Enables anatomic reduction and strong rotational control; has the strongest evidence base | Requires soft-tissue stripping; may cause implant prominence; carries a risk of refracture after implant removal [4-7,25] | Tier 1; nonunion, 2%–10%; infection, 1%–6% |
| Mini-plate/dual-plate fixation (2.4–2.7 mm) | Narrow corridors, short segments, thin soft-tissue envelopes, or situations requiring a lower-profile construct | Provides a low-profile construct and contouring versatility; can distribute fixation through orthogonal dual plates | Supported by limited clinical evidence; may be mechanically insufficient if fixation principles are not respected [11,12] | Tier 2; no robust pooled benchmark |
| Interlocking IM nailing | Simple transverse or short-oblique patterns; soft-tissue compromise; polytrauma | Requires less dissection and shorter incisions; may reduce operative time | Recreation of the radial bow and rotational control remain challenging; careful patient selection is required [13-16] | Tier 2; acceptable union in selected cases |
| NPC (same-bone fixation) | Severe comminution, revision nonunion, or selected salvage situations | Provides internal support and load sharing in complex cases | Supported by limited clinical evidence; technically demanding; risk of screw-nail interference | Tier 3; no published comparative outcome data |
| Transosseous wiring plus plate fixation | Simple transverse fractures without a lag-screw option | Facilitates interfragmentary compression as an adjunctive technique | Adjunctive technique only; excessive wiring may compromise periosteal blood supply [24] | Tier 3; small retrospective reports only |
| MIPO (bridge plating) | Comminuted or segmental fractures; soft-tissue-compromised injuries | Preserves fracture biology and reduces soft-tissue disruption | Limited capacity for precise rotational control and radial bow restoration [21] | Tier 2; retrospective evidence only |
- 1. Matthews LS, Kaufer H, Garver DF, Sonstegard DA. The effect on supination-pronation of angular malalignment of fractures of both bones of the forearm. J Bone Joint Surg Am 1982;64:14-7.ArticlePubMed
- 2. Tarr RR, Garfinkel AI, Sarmiento A. The effects of angular and rotational deformities of both bones of the forearm: an in vitro study. J Bone Joint Surg Am 1984;66:65-70.ArticlePubMed
- 3. Schemitsch EH, Richards RR. The effect of malunion on functional outcome after plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 1992;74:1068-78.ArticlePubMed
- 4. Anderson LD, Sisk D, Tooms RE, Park WI. Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-97.ArticlePubMed
- 5. Chapman MW, Gordon JE, Zissimos AG. Compression-plate fixation of acute fractures of the diaphysis of the radius and ulna. J Bone Joint Surg Am 1989;71:159-69.ArticlePubMed
- 6. Stern PJ, Drury WJ. Complications of plate fixation of forearm fractures. Clin Orthop Relat Res 1983;175:25-9.Article
- 7. Droll KP, Perna P, Potter J, Harniman E, Schemitsch EH, McKee MD. Outcomes following plate fixation of fractures of both bones of the forearm in adults. J Bone Joint Surg Am 2007;89:2619-24.ArticlePubMed
- 8. Saikia K, Bhuyan S, Bhattacharya T, Borgohain M, Jitesh P, Ahmed F. Internal fixation of fractures of both bones forearm: comparison of locked compression and limited contact dynamic compression plate. Indian J Orthop 2011;45:417-21.ArticlePubMedPMCPDF
- 9. Azboy I, Demirtas A, Uçar BY, Bulut M, Alemdar C, Ozkul E. Effectiveness of locking versus dynamic compression plates for diaphyseal forearm fractures. Orthopedics 2013;36:e917-22.ArticlePubMed
- 10. Kim SB, Heo YM, Yi JW, Lee JB, Lim BG. Shaft fractures of both forearm bones: the outcomes of surgical treatment with plating only and combined plating and intramedullary nailing. Clin Orthop Surg 2015;7:282-90.ArticlePubMedPMC
- 11. Wahbeh JM, Kelley BV, Shokoohi C, et al. Comparison of a 2.7-mm and 3.5-mm locking compression plate for ulnar fractures: a biomechanical evaluation. OTA Int 2023;6:e278.ArticlePubMedPMC
- 12. Justice W, Adams A, Kasper A, Takagi-Stewart J, Ilyas AM. Forearm fracture fixation with locking plates: does size matter. J Hand Surg Glob Online 2024;6:319-22.ArticlePubMedPMC
- 13. Lari A, Hassan Y, Altammar A, et al. Interlocking intramedullary nail for forearm diaphyseal fractures in adults: a systematic review and meta-analysis of outcomes and complications. J Orthop Traumatol 2024;25:16.ArticlePubMedPMCPDF
- 14. Box MW, Stegelmann SD, Domingue GA, et al. Intramedullary nail fixation versus open reduction and internal fixation for treatment of adult diaphyseal forearm fractures: a systematic review and meta-analysis. J Orthop Surg Res 2024;19:719.ArticlePubMedPMCPDF
- 15. Zhao L, Wang B, Bai X, Liu Z, Gao H, Li Y. Plate fixation versus intramedullary nailing for both-bone forearm fractures: a meta-analysis of randomized controlled trials and cohort studies. World J Surg 2017;41:722-33.ArticlePubMedPDF
- 16. Kale SY, Singh SD, Samant P, Bukalsaria D, Chaudhari P, Ghodke RJ. Treatment of diaphyseal forearm fracture with interlocking intramedullary nailing: a pilot study. J Clin Orthop Trauma 2021;17:195-200.ArticlePubMedPMC
- 17. Köse A, Aydın A, Ezirmik N, Topal M, Can CE, Yılar S. Intramedullary nailing of adult isolated diaphyseal radius fractures. Ulus Travma Acil Cerrahi Derg 2016;22:184-91.ArticlePubMed
- 18. Blažević D, Benčić I, Ćuti T, et al. Intramedullary nailing of adult forearm fractures: results and complications. Injury 2021;52 Suppl 5:S44-8.ArticlePubMed
- 19. Lee SK, Kim KJ, Lee JW, Choy WS. Plate osteosynthesis versus intramedullary nailing for both forearm bones fractures. Eur J Orthop Surg Traumatol 2014;24:769-76.ArticlePubMedPDF
- 20. Lee YH, Lee SK, Chung MS, Baek GH, Gong HS, Kim KH. Interlocking contoured intramedullary nail fixation for selected diaphyseal fractures of the forearm in adults. J Bone Joint Surg Am 2008;90:1891-8.ArticlePubMed
- 21. Kang HT, Jo YH, Kang HJ. Comparison of minimally invasive plate osteosynthesis (MIPO) and open reduction and internal fixation (ORIF) for the treatment of radial shaft fractures: a retrospective study. BMC Musculoskelet Disord 2025;26:320.ArticlePubMedPMCPDF
- 22. Abdul Azeem M, Alhojailan K, Awad M, Khaja AF. Post-traumatic radioulnar synostosis: a retrospective case series of 10 patients in Kuwait. J Shoulder Elbow Surg 2022;31:1595-602.ArticlePubMed
- 23. Crow BD, Mundis G, Anglen JO. Clinical results of minimal screw plate fixation of forearm fractures. Am J Orthop (Belle Mead NJ) 2007;36:477-80.PubMed
- 24. Choi SJ, Jung SY, Kim MB. Transosseous wiring method for simple transverse shaft fracture of the upper extremity. Arch Hand Microsurg 2024;29:34-9.ArticlePDF
- 25. Beaupre GS, Csongradi JJ. Refracture risk after plate removal in the forearm. J Orthop Trauma 1996;10:87-92.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteCurrent concepts and applications of internal fixation for forearm diaphyseal fractures
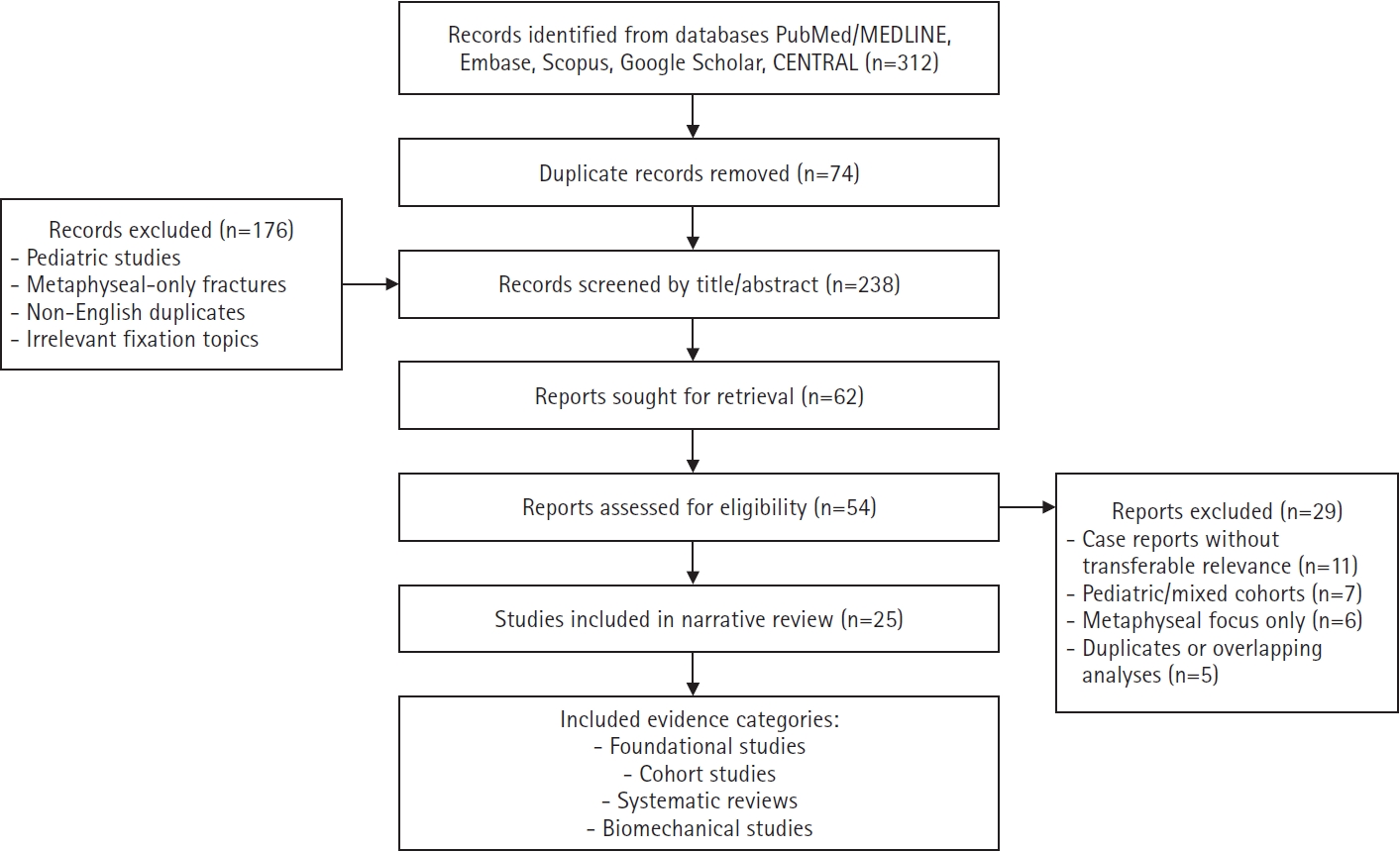



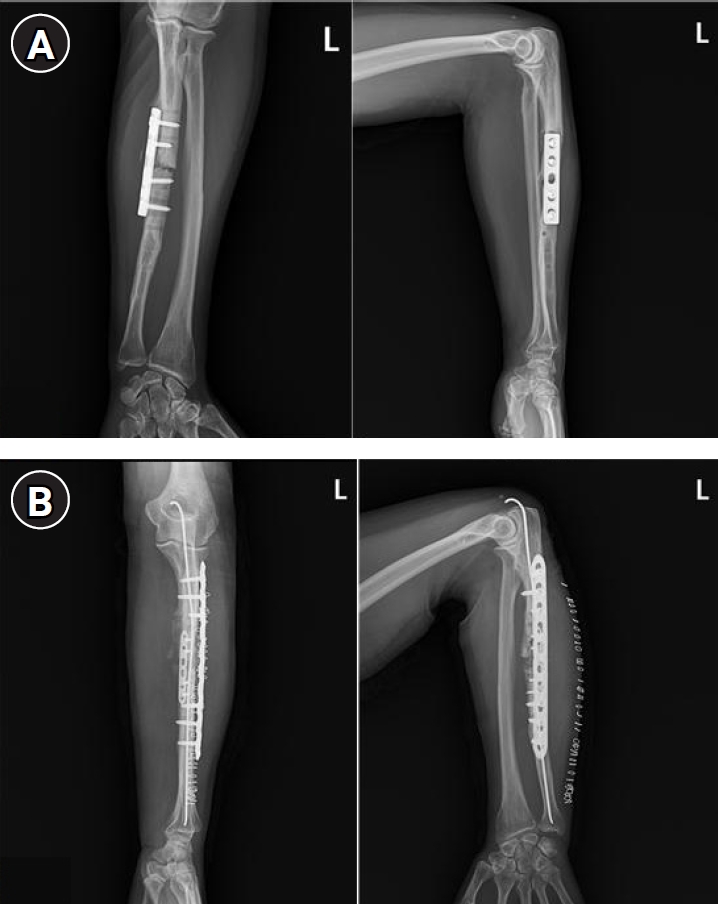
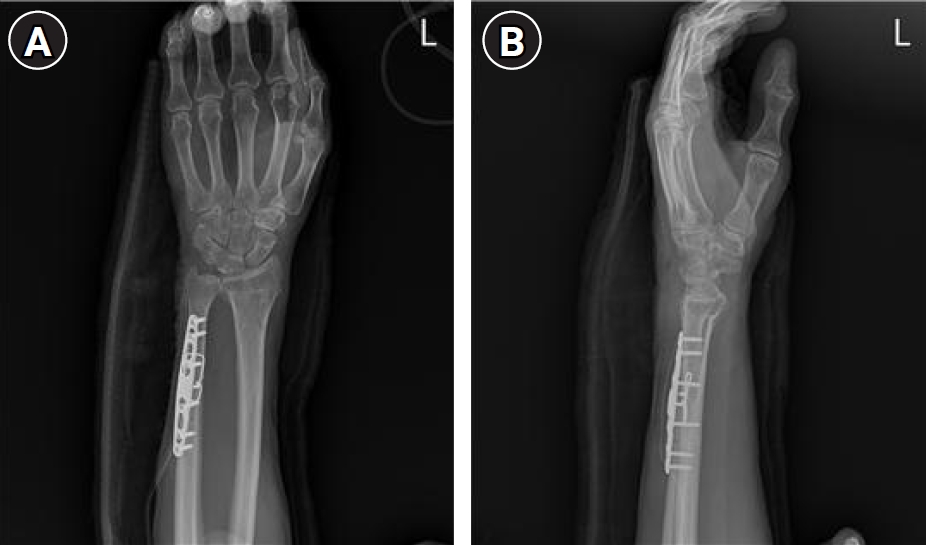
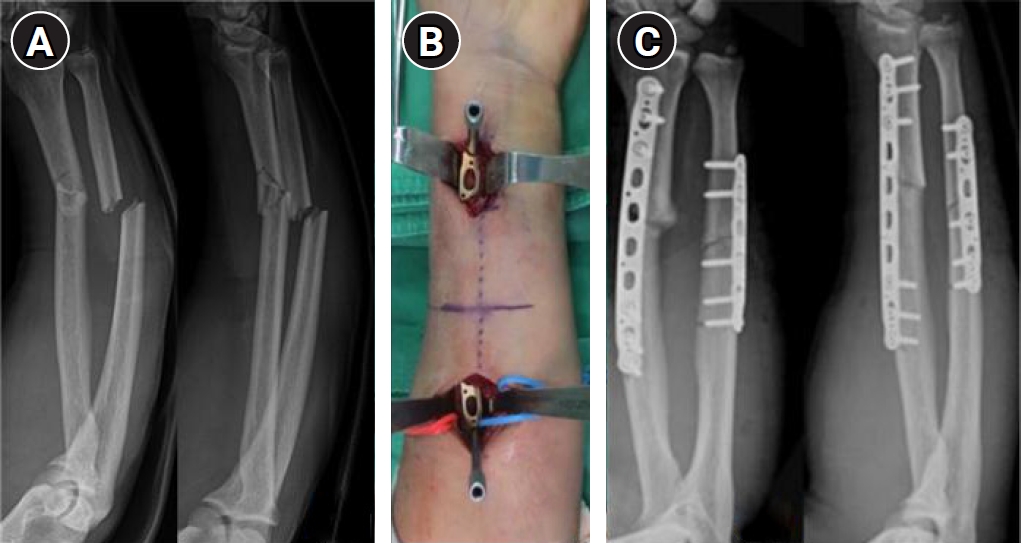
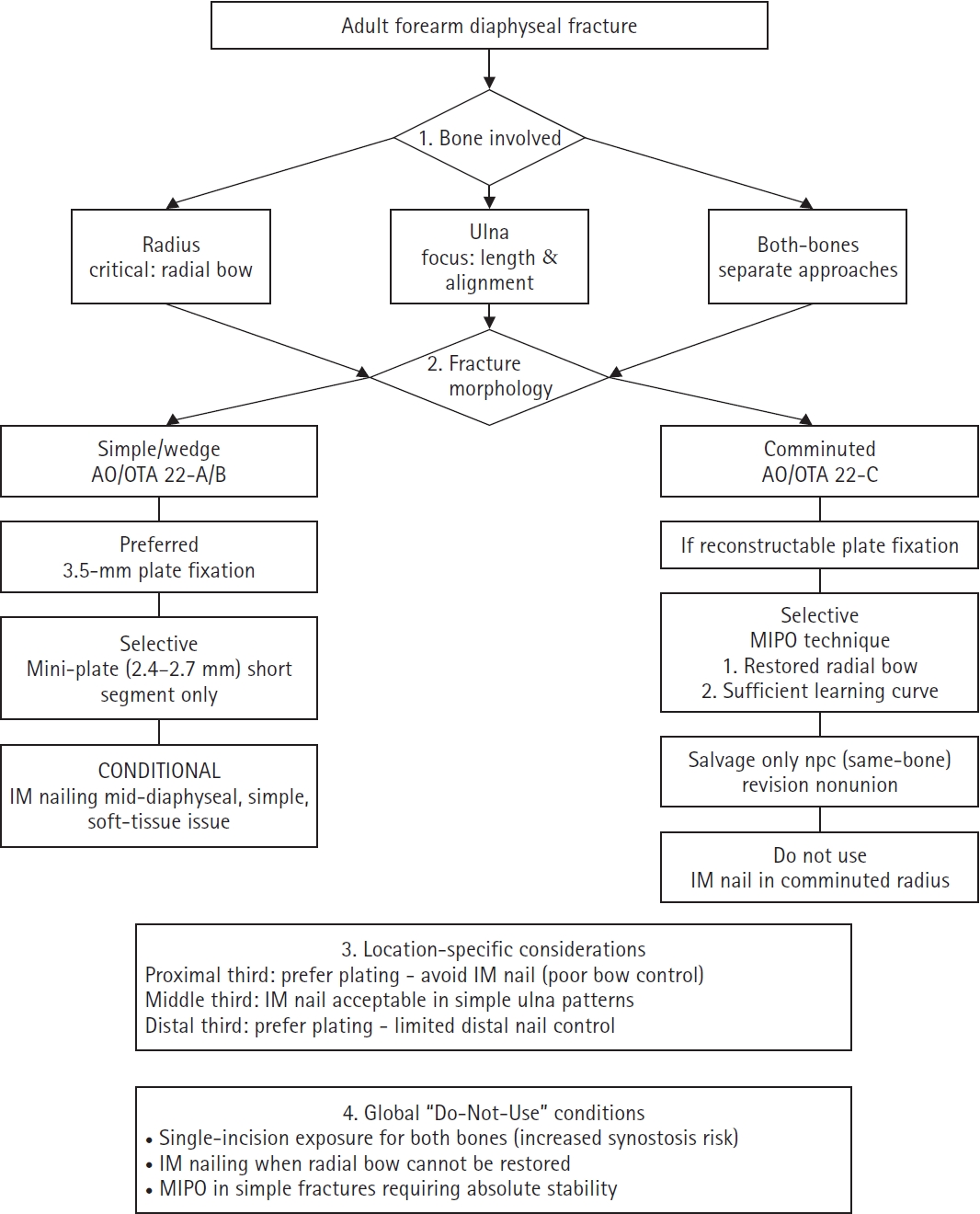
Fig. 1. PRISMA-style flow diagram showing literature identification, screening, eligibility assessment, and study inclusion for this narrative review.
Fig. 2. A 40-year-old male patient with a radial shaft fracture. (A) Preoperative anteroposterior and lateral radiographs demonstrating a diaphyseal radial fracture. (B) Immediate postoperative radiographs after open reduction and internal fixation using a 3.5-mm plate.
Fig. 3. A 62-year-old male patient with a radial shaft fracture. (A) Preoperative anteroposterior and lateral radiographs showing a diaphyseal radial fracture. (B) Immediate postoperative radiographs after mini-fragment dual plating with 2.4–2.7-mm plates.
Fig. 4. A 38-year-old male patient with both-bone forearm shaft fractures treated with interlocking intramedullary nailing. (A) Preoperative radiographs. (B) Immediate postoperative radiographs after interlocking intramedullary nail fixation.
Fig. 5. A 65-year-old female patient with established nonunion after prior ulnar fixation. (A) Preoperative radiographs. (B) Immediate postoperative radiographs after revision fixation using a nail-plate construct.
Fig. 6. A 63-year-old male patient. Immediate postoperative (A) anteroposterior and (B) lateral radiographs after transosseous wiring-assisted plate fixation.
Fig. 7. A 43-year-old female patient with a comminuted radial shaft fracture treated with minimally invasive plate osteosynthesis. (A) Preoperative radiographs. (B) Intraoperative clinical photograph demonstrating external distractor-assisted indirect reduction. (C) Immediate postoperative radiographs after bridge plating using minimally invasive plate osteosynthesis.
Fig. 8. Pattern-based decision-tree flowchart for fixation selection in adult forearm diaphyseal fractures, incorporating the bone involved (radius vs. ulna), fracture location (proximal, middle, or distal third), fracture morphology, and explicit contraindications. MIPO, minimally invasive plate osteosynthesis; IM, intramedullary; NPC, nail-plate construct.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fig. 5.
Fig. 6.
Fig. 7.
Fig. 8.
Current concepts and applications of internal fixation for forearm diaphyseal fractures
| Technique | Best indications | Key advantages | Primary caveats | Evidence tier/quantitative note |
|---|---|---|---|---|
| 3.5-mm LCP plating | Simple or wedge diaphyseal patterns; most both-bone fractures; cases requiring precise restoration of the radial bow | Enables anatomic reduction and strong rotational control; has the strongest evidence base | Requires soft-tissue stripping; may cause implant prominence; carries a risk of refracture after implant removal [4-7,25] | Tier 1; nonunion, 2%–10%; infection, 1%–6% |
| Mini-plate/dual-plate fixation (2.4–2.7 mm) | Narrow corridors, short segments, thin soft-tissue envelopes, or situations requiring a lower-profile construct | Provides a low-profile construct and contouring versatility; can distribute fixation through orthogonal dual plates | Supported by limited clinical evidence; may be mechanically insufficient if fixation principles are not respected [11,12] | Tier 2; no robust pooled benchmark |
| Interlocking IM nailing | Simple transverse or short-oblique patterns; soft-tissue compromise; polytrauma | Requires less dissection and shorter incisions; may reduce operative time | Recreation of the radial bow and rotational control remain challenging; careful patient selection is required [13-16] | Tier 2; acceptable union in selected cases |
| NPC (same-bone fixation) | Severe comminution, revision nonunion, or selected salvage situations | Provides internal support and load sharing in complex cases | Supported by limited clinical evidence; technically demanding; risk of screw-nail interference | Tier 3; no published comparative outcome data |
| Transosseous wiring plus plate fixation | Simple transverse fractures without a lag-screw option | Facilitates interfragmentary compression as an adjunctive technique | Adjunctive technique only; excessive wiring may compromise periosteal blood supply [24] | Tier 3; small retrospective reports only |
| MIPO (bridge plating) | Comminuted or segmental fractures; soft-tissue-compromised injuries | Preserves fracture biology and reduces soft-tissue disruption | Limited capacity for precise rotational control and radial bow restoration [21] | Tier 2; retrospective evidence only |
Table 1. Summary of fixation techniques for adult forearm diaphyseal fractures
LCP, locking compression plate; IM, intramedullary; NPC, nail-plate construct; MIPO, minimally invasive plate osteosynthesis.

