 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 23(3); 2010 > Article
-
Original Article
- Arthroscopic Treatment of Acromioclavicular Joint Dislocation Using TightRope(R): Preliminary Report
- Eui-Sung Choi, M.D., Kyoung-Jin Park, M.D., Yong-Min Kim, M.D., Dong-Soo Kim, M.D., Hyun-Chul Shon, M.D., Byung-Ki Cho, M.D., Ji-Kang Park, M.D, Hyun-Chul Lee, M.D.
-
Journal of the Korean Fracture Society 2010;23(3):310-316.
DOI: https://doi.org/10.12671/jkfs.2010.23.3.310
Published online: July 31, 2010
Department of Orthopedic Surgery, College of Medicine, Chungbuk National University, Cheongju, Korea.
- Address reprint requests to: Kyoung-Jin Park, M.D. Department of Orthopedic Surgery, College of Medicine, Chungbuk National University, 62, Gaesin-dong, Heungdeok-gu, Cheongju 360-711, Korea. Tel: 82-43-269-6077, Fax: 82-43-274-8719, oslion@chungbuk.ac.kr
• Received: November 30, 2009 • Revised: February 16, 2010 • Accepted: April 5, 2010
Copyright © 2010 The Korean Fracture Society
- 1,126 Views
- 6 Download
- 2 Crossref
Abstract
-
Purpose
- To evaluate the clinical and radiologic results of the arthroscopic treatment using TightRope® (Arthrex, Inc, Naples, FL) for management of acute acromioclavicular dislocation.
-
Materials and Methods
- Twelve patients with acromioclavicular joint dislocation Rockwood type V are underwent the arthroscopic acromioclavicular joint reconstruction using TightRope® between March, 2008 and March, 2009. The average age was 40.4 years (range 25~63 years) and mean follow-up was 10 months (range 8~16 months). The shoulders were evaluated using parameters include radiologic measurements by comparing the clavicle posteroanterior and lateral radiographs with the contralateral one. Clinical evaluation was made for pain, function, and range of joint motion by Constant score and KSS (Korean Shoulder Score).
-
Results
- All twelve patients returned to their work without pain in 3 months after operation. The average Constant score and KSS score was 98.4 (range 97~100) and 97.8 (range 97~100) at the last follow-up. Because of technical error and indication error, two patients showed failures of TightRope® fixation on the coracoid side and the acromioclavicular joint was redislocated, so these cases were excluded. 10 patients were satisfied with functional results and cosmetic appearance.
-
Conclusion
- Considering its less morbidity, less hospitalization, excellent cosmesis, early rehabilitation, this new technique offers an attractive alternative in acromioclavicular joint stabilization if the early technical error would be overcome.
- 1. Bae KC, Sohn SW, Cho CH, Jung SW. Surgical treatment of acromioclavicular dislocation -Comparison of modified Weaver-Dunn method and modified Phemister method-. J Korean Shoulder Elbow Soc, 2006;9:155-161.Article
- 2. Ball SV, Sankey A, Cobiella C. Clavicle fracture following tight rope fixation of acromioclavicular joint dislocation. Injury Extra, 2007;38:430-432.Article
- 3. Bannister GC, Wallace WA, Stableforth PG, Hutson MA. The management of acute acromioclavicular dislocation. A randomised prospective controlled trial. J Bone Joint Surg Br, 1989;71:848-850.ArticlePDF
- 4. Baumgarten KM, Altchek DW, Cordasco FA. Arthroscopically assisted acromioclavicular joint reconstruction. Arthroscopy, 2006;22:228.e1-228.e6.Article
- 5. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res, 1987;214:160-164.Article
- 6. Fukuda K, Craig EV, An KN, Cofield RH, Chao EY. Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am, 1986;68:434-440.Article
- 7. Habernek H, Weinstabl R, Schmid L, Fialka C. A crook plate for treatment of acromioclavicular joint separation: indication, technique, and results after one year. J Trauma, 1993;35:893-901.
- 8. Jari R, Costic RS, Rodosky MW, Debski RE. Biomechanical function of surgical procedures for acromioclavicular joint dislocations. Arthroscopy, 2004;20:237-245.Article
- 9. Kocher MS, Dupre MM, Feagin JAJ. Shoulder injuries from alpine skiing and snowboarding. Aetiology, treatment and prevention. Sports Med, 1998;25:201-211.
- 10. Lafosse L, Baier GP, Leuzinger J. Arthroscopic treatment of acute and chronic acromioclavicular joint dislocation. Arthroscopy, 2005;21:1017. Article
- 11. Mazzocca AD, Conway JE, Johnson S. The anatomic coracoclavicular ligament reconstruction. Oper Tech Sports Med, 2004;12:56-61.Article
- 12. Rolla PR, Surace MF, Murena L. Arthroscopic treatment of acute acromioclavicular joint dislocation. Arthroscopy, 2004;20:662-668.Article
- 13. Shin SJ, Roh KJ, Jeong BJ. Coracoclavicular ligament reconstruction for acromioclavicular dislocation using two suture anchors and coracoacromial ligament transfer. J Korean Shoulder Elbow Soc, 2008;11:46-52.
- 14. Sim E, Schwarz N, Höcker K, Berzlanovich A. Repair of complete acromioclavicular seperations using the acromioclavicular-hook plate. Clin Orthop Relat Res, 1995;314:134-142.
- 15. Taft TN, Wilson FC, Oglesby JW. Dislocation of the acromioclavicular joint. An end-result study. J Bone Joint Surg Am, 1987;69:1045-1051.Article
- 16. Tomlinson DP, Altchek DW, Davila J, Cordasco FA. A modified technique of arthroscopically assisted AC joint reconstruction and preliminary results. Clin Orthop Relat Res, 2008;466:639-645.Article
- 17. Trikha SP, Acton D, Wilson AJ, Curtis MJ. A new method of arthroscopic reconstruction of the dislocated acromio-clavicular joint. Ann R Coll Surg Engl, 2004;86:161-164.Article
- 18. Weitzman G. Treatment of acute acromioclavicular joint dislocation by a modified Bosworth method. J Bone Joint Surg Am, 1967;49:1167-1178.Article
- 19. Wolf EM, Pennington WT. Arthroscopic reconstruction for acromioclavicular joint dislocation. Arthroscopy, 2001;17:558-563.Article
REFERENCES
Figure 1
(A, B) Preoperative radiographs of a type V acromioclavicular dislocation (arrow).
(C, D) Postoperative radiographs shows anatomical reduction of the right acromioclavicular joint using TightRope® (arrow).

Figure 2
(A) The base of corcacoid process is visualized with the 70 degree scope by the posterior portal. The tip of the guide pin is stopped by the drill stop at the base of the coracoid process under direct visualization.
(B) Identification of the coracoid button and the security of reduction is confirmed.

Figure 3
(A) Postoperative 6 months later, radiograph shows the sinking of superior endobutton (arrow).
(B) MRI confirms the healing of coracoclavicular ligament (arrow).
(C) After removing TightRope®, photograph shows residual hole in clavicle (arrow).
(D) Postoperative radiograph shows no increasement of the coracoclavicular distance (arrow).


Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Coracoclavicular Ligament Augmentation Using Tight-Rope®for Acute Acromioclavicular Joint Dislocation - Preliminary Report -
Seok Hyun Kweon, Sang Su Choi, Seong In Lee, Jeong Woo Kim, Kwang Mee Kim
The Journal of the Korean Shoulder and Elbow Society.2013; 16(2): 115. CrossRef - Coracoclavicular Ligament Augmentation Using Endobutton for Unstable Distal Clavicle Fractures - Preliminary Report -
Chul-Hyun Cho, Gu-Hee Jung, Hong-Kwan Sin, Young-Kuk Lee, Jin-Hyun Park
The Journal of the Korean Shoulder and Elbow Society.2011; 14(1): 1. CrossRef
 Cite
CiteArthroscopic Treatment of Acromioclavicular Joint Dislocation Using TightRope(R): Preliminary Report
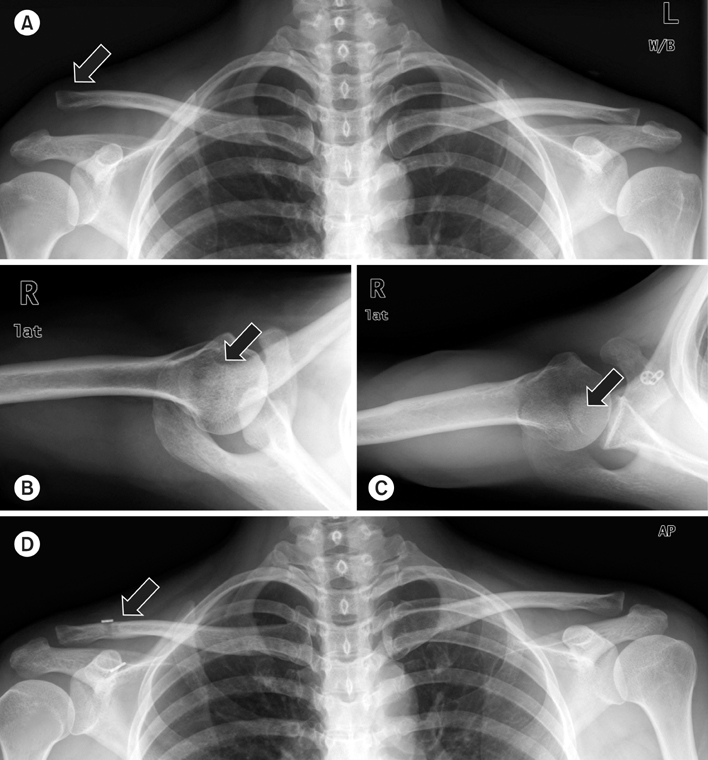
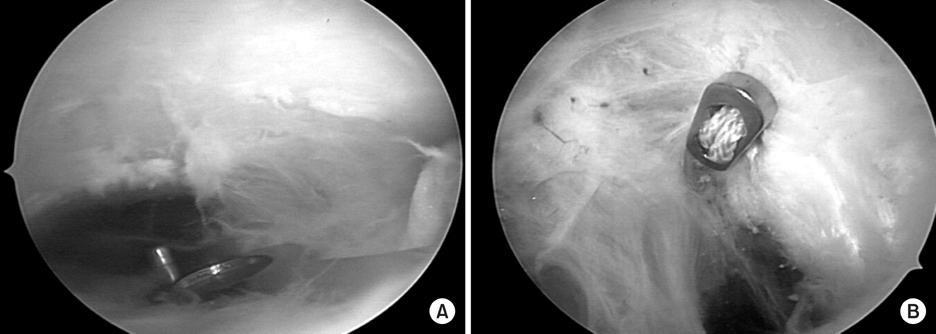
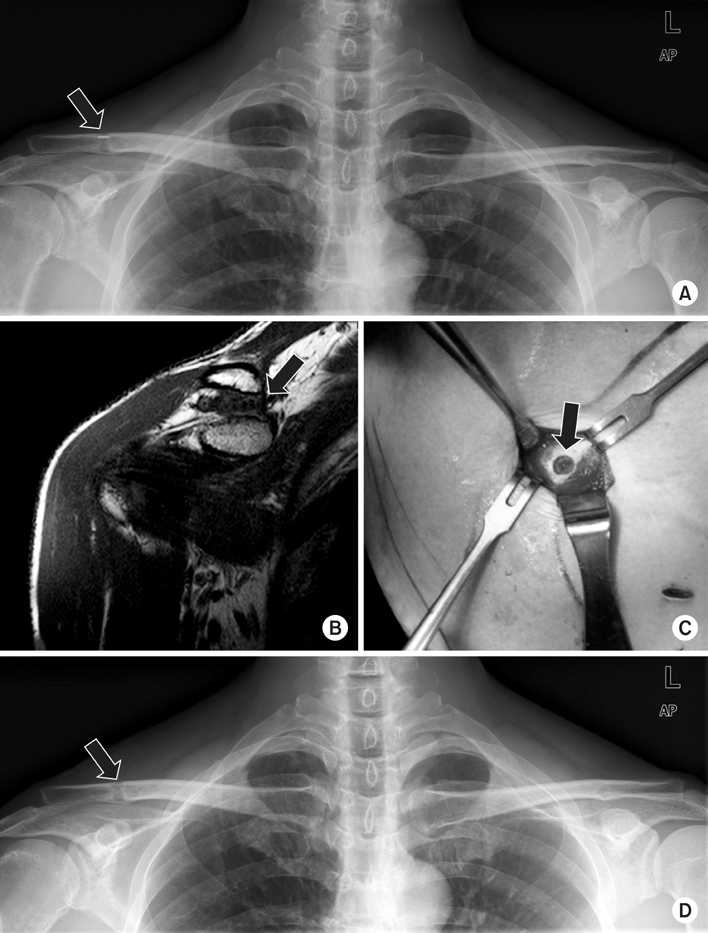
Figure 1
(A, B) Preoperative radiographs of a type V acromioclavicular dislocation (arrow).
(C, D) Postoperative radiographs shows anatomical reduction of the right acromioclavicular joint using TightRope® (arrow).
Figure 2
(A) The base of corcacoid process is visualized with the 70 degree scope by the posterior portal. The tip of the guide pin is stopped by the drill stop at the base of the coracoid process under direct visualization.
(B) Identification of the coracoid button and the security of reduction is confirmed.
Figure 3
(A) Postoperative 6 months later, radiograph shows the sinking of superior endobutton (arrow).
(B) MRI confirms the healing of coracoclavicular ligament (arrow).
(C) After removing TightRope®, photograph shows residual hole in clavicle (arrow).
(D) Postoperative radiograph shows no increasement of the coracoclavicular distance (arrow).
Figure 1
Figure 2
Figure 3
Arthroscopic Treatment of Acromioclavicular Joint Dislocation Using TightRope(R): Preliminary Report
Comparison of radiologic and clinical results
Table 1
Comparison of radiologic and clinical results

