 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 25(2); 2012 > Article
-
Original Article
- Comparison of Plate Versus Threaded K-wire for Fixation of Midshaft Clavicular Fractures
- Young-Jin Ko, M.D., Chul-Hyun Park, M.D., Oog-Jin Shon, M.D., Jae-Sung Seo, M.D.
-
Journal of the Korean Fracture Society 2012;25(2):123-128.
DOI: https://doi.org/10.12671/jkfs.2012.25.2.123
Published online: April 17, 2012
Department of Orthopedic Surgery, Yeungnam University College of Medicine, Daegu, Korea.
- Address reprint requests to: Oog-Jin Shon, M.D. Department of Orthopedic Surgery, Yeungnam University Hospital, 317-1, Daemyeong-dong, Nam-gu, Daegu 705-717, Korea. Tel: 82-53-620-3640, Fax: 82-53-628-4020, ossoj@med.yu.ac.kr
• Received: December 23, 2011 • Accepted: January 24, 2012
Copyright © 2012 The Korean Fracture Society
- 1,070 Views
- 3 Download
- 3 Crossref
Abstract
-
Purpose
- To compare clinical outcomes of the plate and threaded K-wire for fixation of midshaft clavicular fractures.
-
Materials and Methods
- From 2005 Jan to 2009 May, medical records of 18 patients who underwent open reduction and internal fixation with plate (group 1) and 13 others who underwent intramedullary fixation with threaded K-wire (group 2) were reviewed. The mean follow up periods were 21.9 and 18.9months. The Functional results were evaluated with The Disabilities of the Arm, Shoulder and Hand (DASH) score and Constant shoulder score. The statistical evaluation was assessed with Paired T-test, Chi-square test.
-
Results
- The DASH score were 11.5±2.7 in group 1 and 12.4±4.3 in group 2. The constant shoulder score were 92.0±3.1 in group 1 and 87.1±2.8 in group 2. Length of surgical wound (cm) were 10.6±3.4 in group 1 and 4.8±1.5 in group 2. Postoperative pain and range of motion change were superior in group 1.
-
Conclusion
- There was no significant difference between the two groups in functional and radiological results. But, there were patient's complaints about length of surgical wound in group 1 and hardware irritation in group 2.
- 1. Beaton DE, Katz JN, Fossel AH, Wright JG, Tarasuk V, Bombardier C. Measuring the whole or the parts? Validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. J Hand Ther, 2001;14:128-146.
- 2. Boehm D, Wollmerstedt N, Doesch M, Handwerker M, Mehling E, Gohlke F. Development of a questionnaire based on the Constant-Murley-Score for self-evaluation of shoulder function by patients. Unfallchirurg, 2004;107:397-402.
- 3. Boehme D, Curtis RJ Jr, DeHaan JT, Kay SP, Young DC, Rockwood CA Jr. Non-union of fractures of the mid-shaft of the clavicle. Treatment with a modified Hagie intramedullary pin and autogenous bone-grafting. J Bone Joint Surg Am, 1991;73:1219-1226.Article
- 4. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am, 2007;89:1-10.
- 5. Ferran NA, Hodgson P, Vannet N, Williams R, Evans RO. Locked intramedullary fixation vs plating for displaced and shortened mid-shaft clavicle fractures: a randomized clinical trial. J Shoulder Elbow Surg, 2010;19:783-789.Article
- 6. Kang JD, Ha PS, Kim KU, Gwon YJ. Treatment of the fracture of the middle third of clavicle by intramedullary threaded Steinmann pin fixation. J Korean Orthop Assoc, 1989;24(3):811-816.ArticlePDF
- 7. Kang KS, Ahn JI, Oh HY, Kang YS, Lee SJ. Clinical study of clavicle fractures. J Korean Orthop Assoc, 1984;19(2):367-372.ArticlePDF
- 8. Kettler M, Schieker M, Braunstein V, König M, Mutschler W. Flexible intramedullary nailing for stabilization of displaced midshaft clavicle fractures: technique and results in 87 patients. Acta Orthop, 2007;78:424-429.Article
- 9. Kim BH, Im JI, Yim UK, Kim JJ. Operative treatment of clavicle fracture. J Korean Soc Fract, 1998;11:658-664.Article
- 10. Liu HH, Chang CH, Chia WT, Chen CH, Tarng YW, Wong CY. Comparison of plates versus intramedullary nails for fixation of displaced midshaft clavicular fractures. J Trauma, 2010;69:E82-E87.Article
- 11. Manske DJ, Szabo RM. The operative treatment of mid-shaft clavicular non-unions. J Bone Joint Surg Am, 1985;67:1367-1371.Article
- 12. Mckeever DC. Principles and ideals of intramedullary internal fixation. Clin Orthop, 1953;2:12-19.
- 13. Muller ME, Allgower M, Schneider R, Willenegger H. Manual of internal fixation: technique recommended by the AO group, 1979;2nd ed. Heidelberg, New York, Springe-Verlag. 166.
- 14. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res, 1968;58:43-50.
- 15. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc, 1960;172:1006-1011.Article
- 16. Ngarmukos C, Parkpian V, Patradul A. Fixation of fractures of the midshaft of the clavicle with Kirschner wires. Results in 108 patients. J Bone Joint Surg Br, 1998;80:106-108.
- 17. Poigenfürst J, Reiler T, Fischer W. Plating of fresh clavicular fractures. Experience with 60 operations. Unfallchirurgie, 1988;14:26-37.
- 18. Rowe CR. An atlas of anatomy and treatment of midclavicular fractures. Clin Orthop Relat Res, 1968;58:29-42.
- 19. Stanley D, Norris SH. Recovery following fractures of the clavicle treated conservatively. Injury, 1988;19:162-164.Article
- 20. Zenni EJ Jr, Krieg JK, Rosen MJ. Open reduction and internal fixation of clavicular fractures. J Bone Joint Surg Am, 1981;63:147-151.Article
REFERENCES
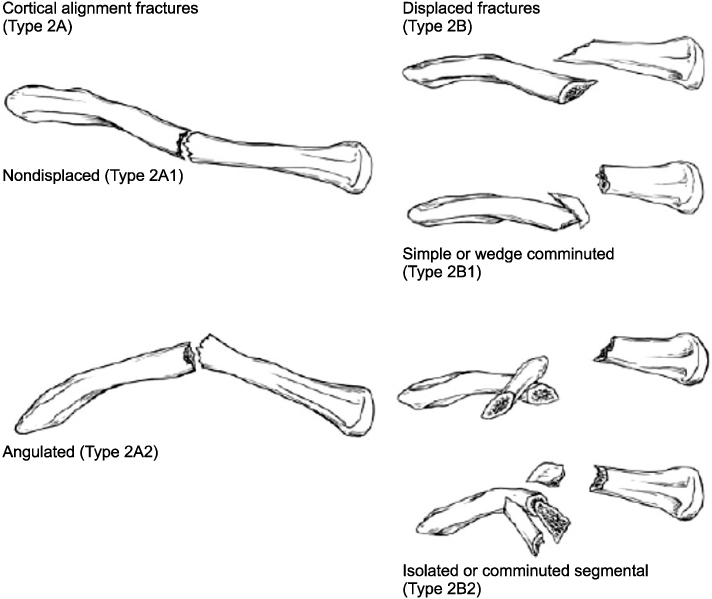
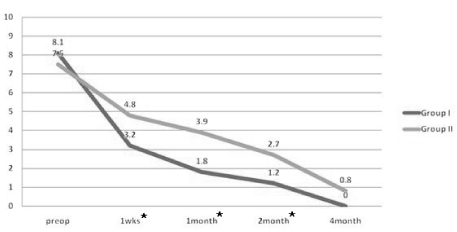
Fig. 3Postoperative range of motion change (A: abduction, F: flexion, *stastistically significant period).
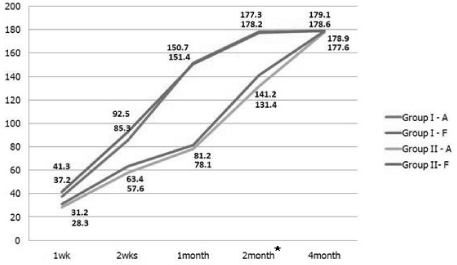
Fig. 4Metal failure cases using 3.5 mm locking compression plate reconstruction plate, AO. (A) Preoperation, (B) postoperation, (C) post operation day (POD) 2 weeks, (D) POD 3 months.
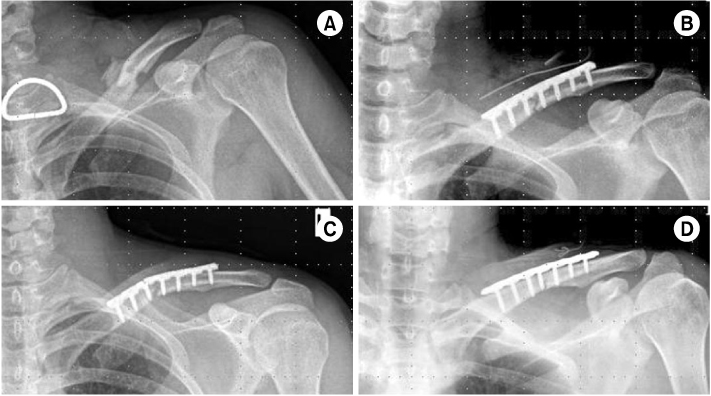
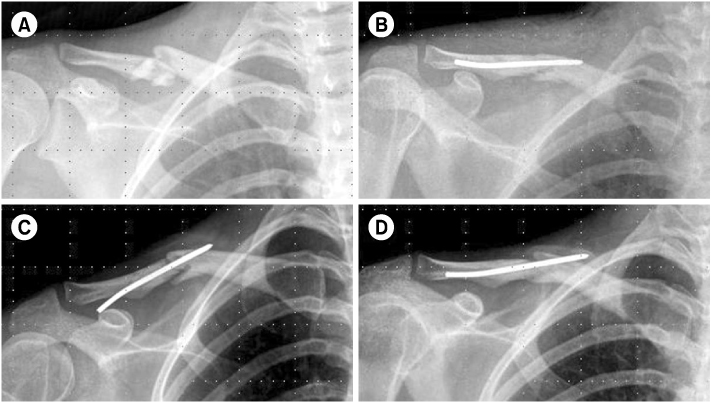
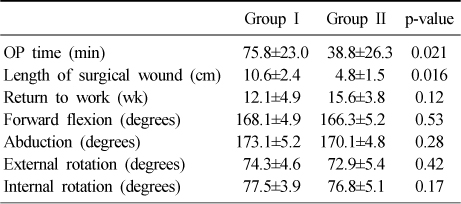
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- A Comparison between Minimally Invasive Percutaneous Plate Osteosynthesis and Plate Fixation in the Treatment of Clavicle Midshaft Fracture
Seong-Ho Yoo, Suk-Woong Kang, Bu-Hwan Kim, Moo-Ho Song, Yeong-Joon Kim, Gyu-Taek Park, Chang-Hun Kwack
Journal of the Korean Orthopaedic Association.2017; 52(1): 1. CrossRef - Plate fixation versus intramedullary fixation for midshaft clavicle fractures: Meta-analysis of complications and functional outcomes
Hao Xiao, Hengbo Gao, Tuokang Zheng, Jianhui Zhao, Yingping Tian
Journal of International Medical Research.2016; 44(2): 201. CrossRef - Meta-analysis of plate fixation versus intramedullary fixation for the treatment of mid-shaft clavicle fractures
Bing Zhang, Yanbin Zhu, Fei Zhang, Wei Chen, Ye Tian, Yingze Zhang
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine.2015;[Epub] CrossRef
 Cite
CiteComparison of Plate Versus Threaded K-wire for Fixation of Midshaft Clavicular Fractures
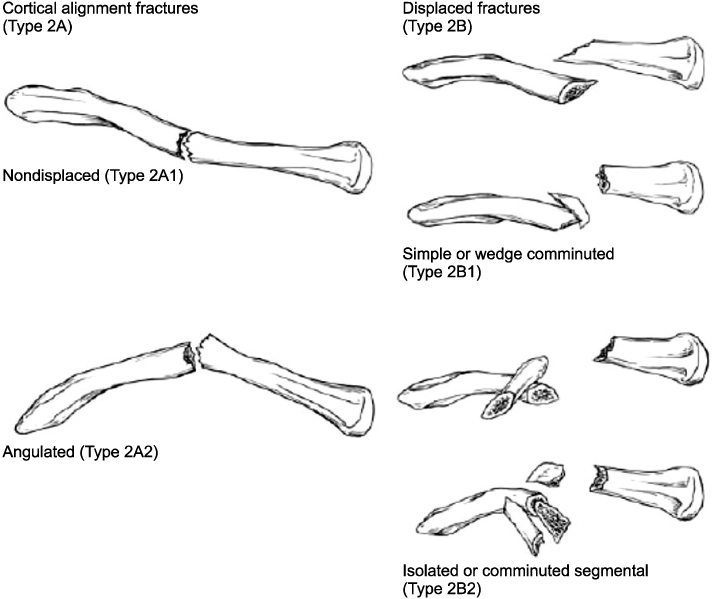
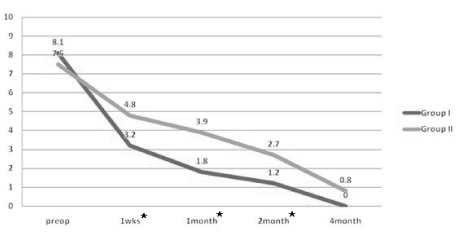
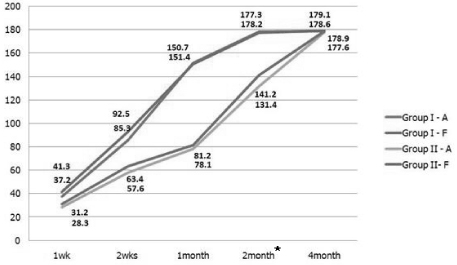
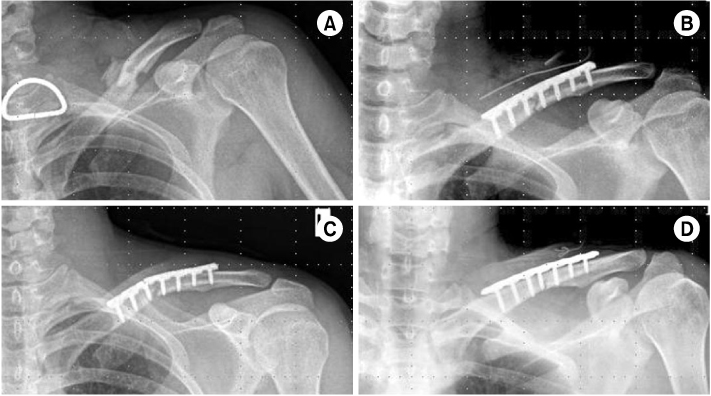
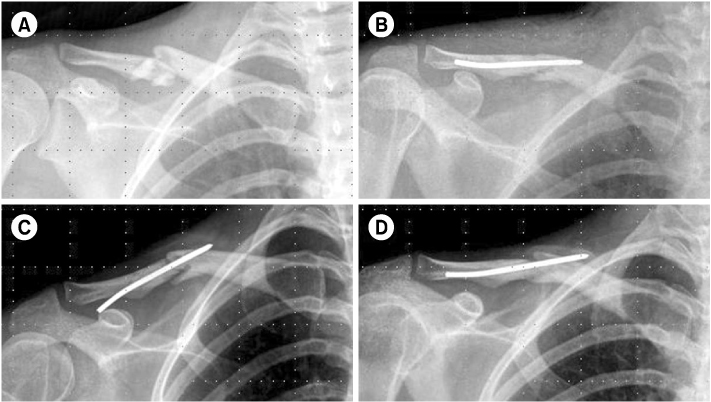
Fig. 1
Robinson's classification system for midshaft clavicular fractures.
Fig. 2
Postoperative pain change (*statistically significant period).
Fig. 3
Postoperative range of motion change (A: abduction, F: flexion, *stastistically significant period).
Fig. 4
Metal failure cases using 3.5 mm locking compression plate reconstruction plate, AO. (A) Preoperation, (B) postoperation, (C) post operation day (POD) 2 weeks, (D) POD 3 months.
Fig. 5
Migration case using 2.8 mm threaded K-wire, AO. (A) Preoperation, (B) postoperation, (C) post operation day 3 months, (D) second postopation.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Comparison of Plate Versus Threaded K-wire for Fixation of Midshaft Clavicular Fractures
Clinical outcomes
OP: Operational.
Table 1
Clinical outcomes
OP: Operational.

