 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 25(2); 2012 > Article
-
Review Article
- Operative Treatment of Humerus Shaft Fracture: Conventional Open Plating or Minimally Invasive Plate Osteosynthesis
- Hyun-Joo Lee, M.D., Chang-Wug Oh, M.D., Ph.D.
-
Journal of the Korean Fracture Society 2012;25(2):155-162.
DOI: https://doi.org/10.12671/jkfs.2012.25.2.155
Published online: April 17, 2012
Department of Orthopedic Surgery, Kyungpook National University Hospital, Daegu, Korea.
- Address reprint requests to: Chang-Wug Oh, M.D., Ph.D. Department of Orthopedic Surgery, Kyungpook National University Hospital, 130, Dongdeok-ro, Jung-gu, Daegu 700-721, Korea. Tel: 82-53-420-5630, Fax: 82-53-422-6605, cwoh@knu.ac.kr
Copyright © 2012 The Korean Fracture Society
- 1,059 Views
- 6 Download
- 3 Crossref
- 1. An Z, Zeng B, He X, Chen Q, Hu S. Plating osteosynthesis of mid-distal humeral shaft fractures: minimally invasive versus conventional open reduction technique. Int Orthop, 2010;34:131-135.ArticlePDF
- 2. Apivatthakakul T, Arpornchayanon O, Bavornratanavech S. Minimally invasive plate osteosynthesis (MIPO) of the humeral shaft fracture. Is it possible? A cadaveric study and preliminary report. Injury, 2005;36:530-538.Article
- 3. Apivatthakakul T, Patiyasikan S, Luevitoonvechkit S. Danger zone for locking screw placement in minimally invasive plate osteosynthesis (MIPO) of humeral shaft fractures: a cadaveric study. Injury, 2010;41:169-172.Article
- 4. Bhandari M, Devereaux PJ, McKee MD, Schemitsch EH. Compression plating versus intramedullary nailing of humeral shaft fractures--a meta-analysis. Acta Orthop, 2006;77:279-284.Article
- 5. Carlan D, Pratt J, Patterson JM, Weiland AJ, Boyer MI, Gelberman RH. The radial nerve in the brachium: an anatomic study in human cadavers. J Hand Surg Am, 2007;32:1177-1182.Article
- 6. Changulani M, Jain UK, Keswani T. Comparison of the use of the humerus intramedullary nail and dynamic compression plate for the management of diaphyseal fractures of the humerus. A randomised controlled study. Int Orthop, 2007;31:391-395.ArticlePDF
- 7. Chapman JR, Henley MB, Agel J, Benca PJ. Randomized prospective study of humeral shaft fracture fixation: intramedullary nails versus plates. J Orthop Trauma, 2000;14:162-166.Article
- 8. Chen AL, Joseph TN, Wolinksy PR, et al. Fixation stability of comminuted humeral shaft fractures: locked intramedullary nailing versus plate fixation. J Trauma, 2002;53:733-737.Article
- 9. Chiu FY, Chen CM, Lin CF, Lo WH, Huang YL, Chen TH. Closed humeral shaft fractures: a prospective evaluation of surgical treatment. J Trauma, 1997;43:947-951.
- 10. Concha JM, Sandoval A, Streubel PN. Minimally invasive plate osteosynthesis for humeral shaft fractures: are results reproducible? Int Orthop, 2010;34:1297-1305.ArticlePDF
- 11. Dabezies EJ, Banta CJ 2nd, Murphy CP, d'Ambrosia RD. Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries. J Orthop Trauma, 1992;6:10-13.
- 12. Farragos AF, Schemitsch EH, McKee MD. Complications of intramedullary nailing for fractures of the humeral shaft: a review. J Orthop Trauma, 1999;13:258-267.Article
- 13. Herscovici D Jr, Anglen JO, Archdeacon MT, Cannada LK, Scaduto JM. Avoiding complications in the treatment of pronation-external rotation ankle fractures, syndesmotic injuries, and talar neck fractures. Instr Course Lect, 2009;58:37-45.
- 14. Ji F, Tong D, Tang H, et al. Minimally invasive percutaneous plate osteosynthesis (MIPPO) technique applied in the treatment of humeral shaft distal fractures through a lateral approach. Int Orthop, 2009;33:543-547.ArticlePDF
- 15. Jiang R, Luo CF, Zeng BF, Mei GH. Minimally invasive plating for complex humeral shaft fractures. Arch Orthop Trauma Surg, 2007;127:531-535.ArticlePDF
- 16. Lee HJ, Oh CW, Kim DH, Park KH. Minimally invasive anterior plating of humeral shaft fractures. J Korean Fract Soc, 2011;24:341-346.Article
- 17. Lin J, Shen PW, Hou SM. Complications of locked nailing in humeral shaft fractures. J Trauma, 2003;54:943-949.Article
- 18. Livani B, Belangero WD. Bridging plate osteosynthesis of humeral shaft fractures. Injury, 2004;35:587-595.Article
- 19. McCormack RG, Brien D, Buckley RE, McKee MD, Powell J, Schemitsch EH. Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail. A prospective, randomised trial. J Bone Joint Surg Br, 2000;82:336-339.
- 20. Oh CW, Byun YS, Oh JK, et al. Plating of humeral shaft fractures: Comparison of standard conventional plating versus minimally invasive plating. Orthop Traumatol Surg Res, 2012;98:54-60.Article
- 21. Volgas DA, Stannard JP, Alonso JE, et al. Nonunions of the humerus. Clin Orthop Relat Res, 2004;(419):46-50.Article
REFERENCES
Fig. 1
(A, B) A 41-year-old female with segmental fracture of the humerus shaft, which is AO/OTA classification C2.
(C, D) Intraoperative fluoroscopic images showing Schanz screws is inserted from the lateral sides of the greater tuberosity and lateral condyle of the humerus with the distal and proximal fragments faced anteriorly. Note that insertion point to avoid injury to the radial nerve.
(E) Reduction is maintained with a unilateral external fixator. A roll of elastic bandage can be used.
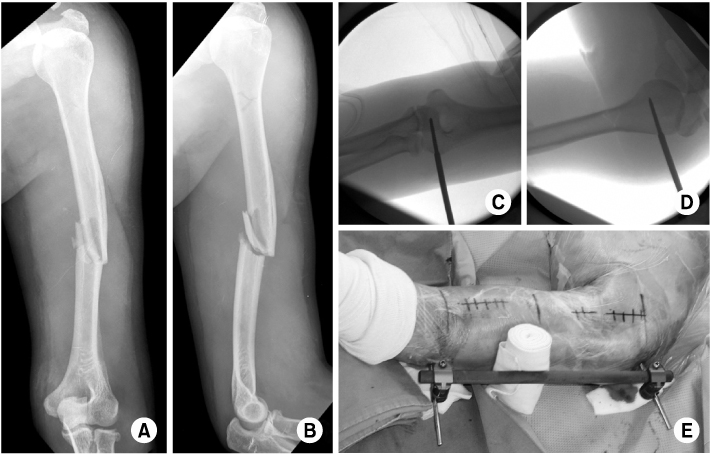
Fig. 2
(A~D) A metaphyseal locking compression plate is inserted from the proximal incision while maintaining reduction with external fixator. The position of the plate is determined by fluoroscopy. Kirschner wires are used for provisional fixation of the plate.
(E~G) Immediate postoperative radiographs showing acceptable alignment. The screws are inserted under direct visualization through the proximal and distal incisions.
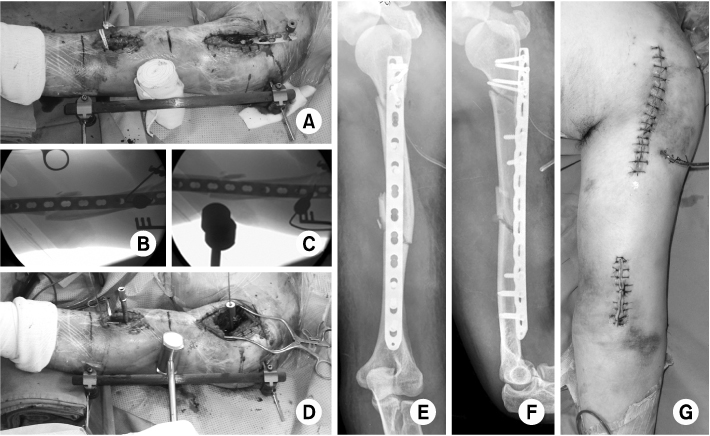
Fig. 3
(A, B) Radiographs taken eight months after the index surgery show complete bone healing.
(C~E) Minimal scar with nearly full range of motion in the shoulder and elbow joints.
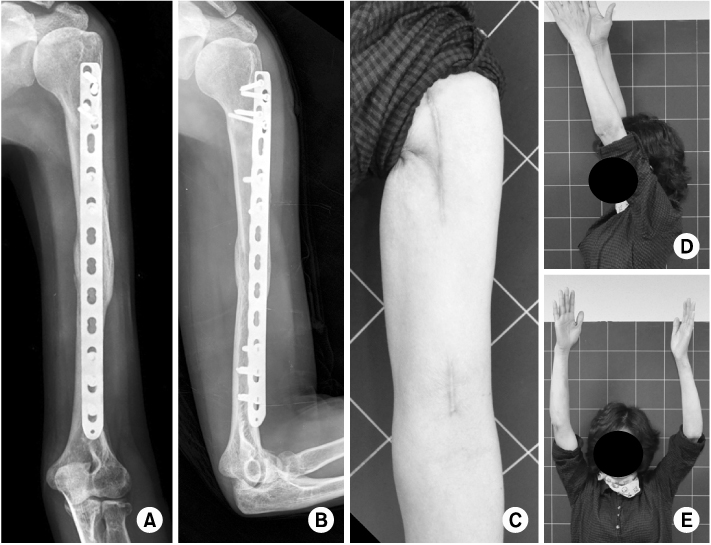
Fig. 4
(A, B) A 61-year-old male with AO/OTA classification C2 fracture of the humerus.
(C~H) The fracture is reduced and maintained by utilizing a elastic nail inserted from the lateral condyle of the humerus.
(I) After making a submuscular tunnel, a locking plate is inserted. Locking drill sleeves can be used as a handle. Note that biceps brachii muscle, split medial part of the brachialis, and the cutaneous brance of the musculocutaneous nerve is retracted medially at the distal incision.
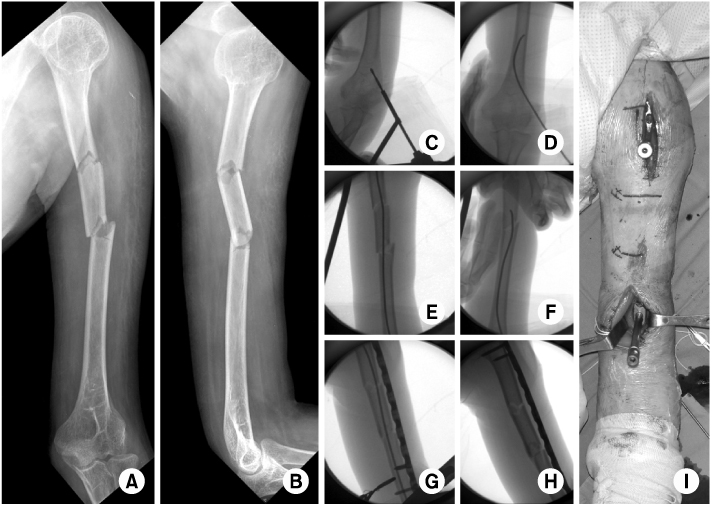
Fig. 5
(A~C) Immediate postoperative radiographs and picture of the surgical wound.
(D, E) Radiographs show complete healing of the fracture eight months after the index surgery.
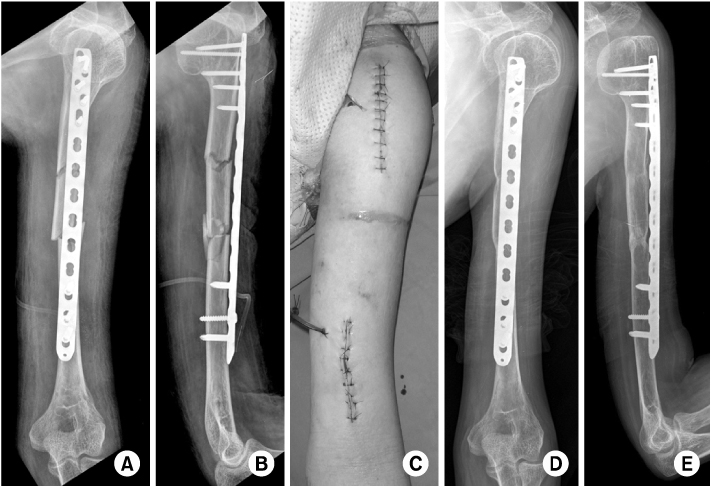
Fig. 6
(A, B) A 64-year-old male showed comminuted humerus shaft fracture of AO/OTA classification B3.
(C~E) Indirect reduction and maintaining reduction was assisted by a unilateral external fixator.
(F) A locking compression plate is introduced into submuscular tunnel.
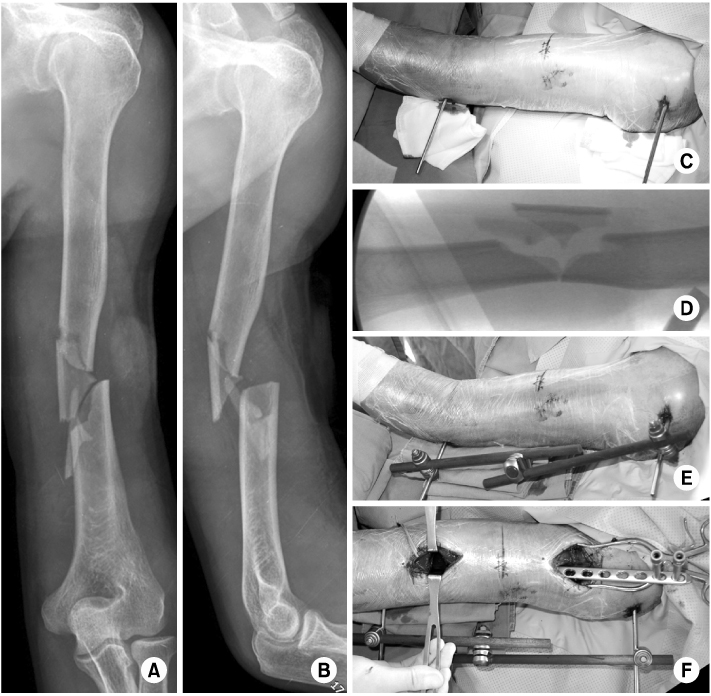
Fig. 7
(A, B) Immediate postoperative radiographs show reduced fracture in anatomical alignment.
(C, D) Nine months after the index surgery, radiographs show complete healing.
(E, F) Minimal scar with recovered range of motion in the shoulder and elbow joints.
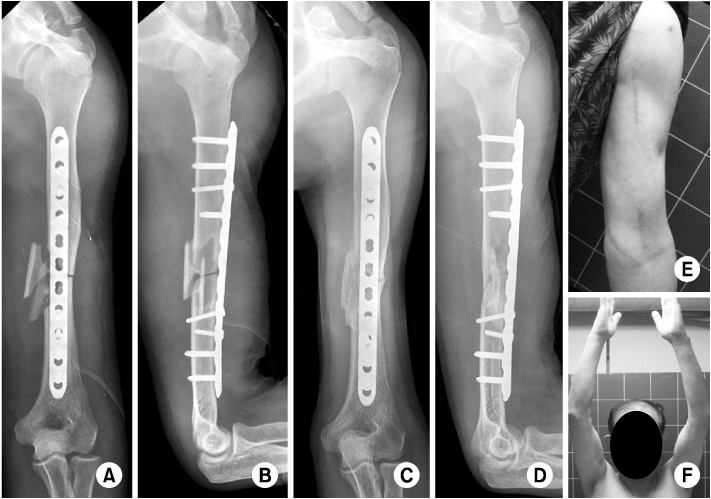
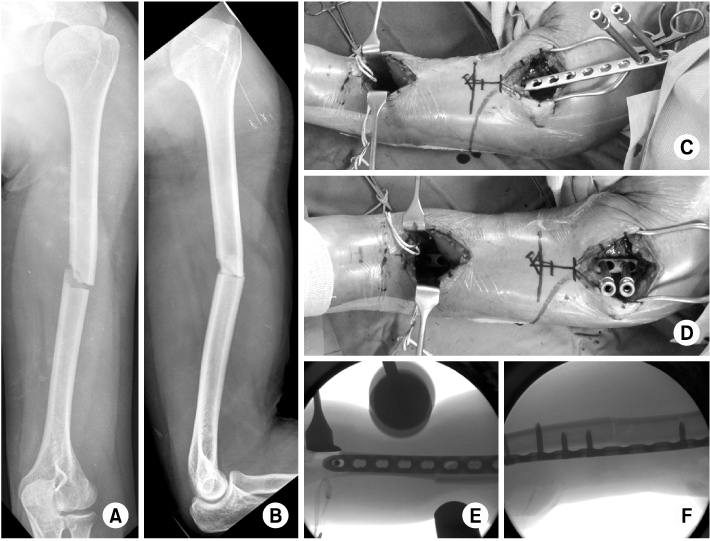
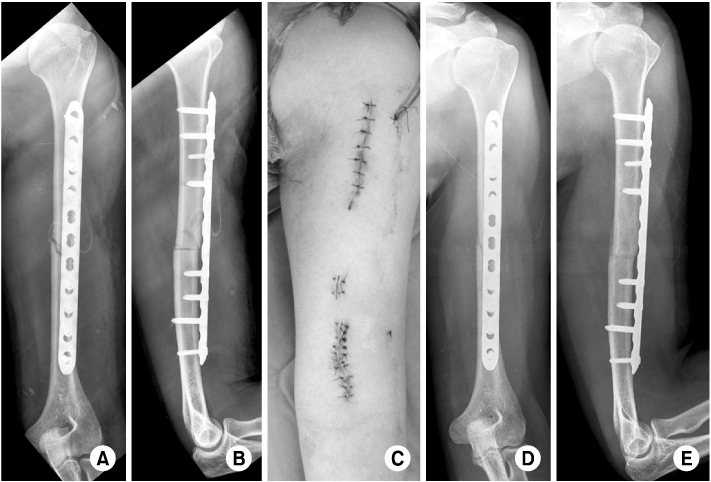
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- A study of functional outcome of humeral shaft fracture treated with anterior bridge plating
Nishant V. SHIVADE, Nitin PATIL, Paresh PATIL, Sapan VORA, Jaykumar K
Minerva Orthopedics.2021;[Epub] CrossRef - Comparing the Use of Single and Double Interlocking Distal Screws on a Polarus Intramedullary Nail for Humeral Shaft Fractures
Hee Seok Yang, Jeong Woo Kim, Hong Je Kang, Jung Hyun Park, Yong Chan Lee, Kwang Mee Kim
Clinics in Shoulder and Elbow.2015; 18(2): 91. CrossRef - Polarus Intramedullary Nail for Proximal Humeral and Humeral Shaft Fractures in Elderly Patients with Osteoporosis
Youn-Soo Hwang, Kwang-Yeol Kim, Hyung-Chun Kim, Su-Han Ahn, Dong-Eun Lee
Journal of the Korean Fracture Society.2013; 26(1): 14. CrossRef
 Cite
CiteOperative Treatment of Humerus Shaft Fracture: Conventional Open Plating or Minimally Invasive Plate Osteosynthesis
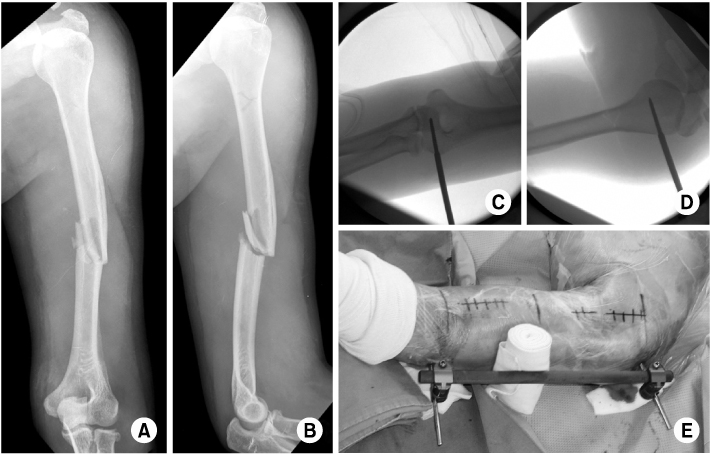
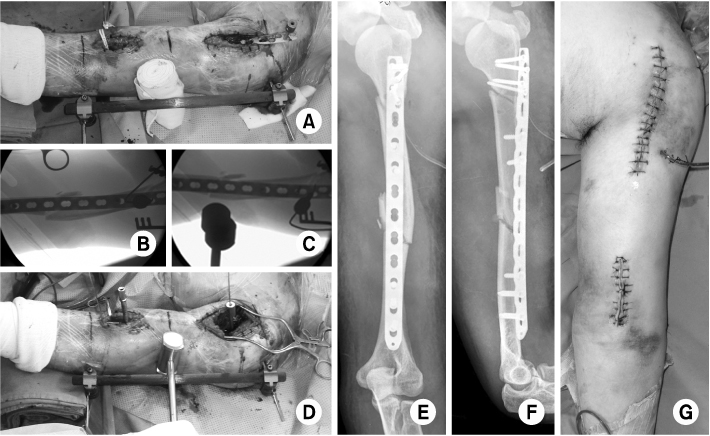
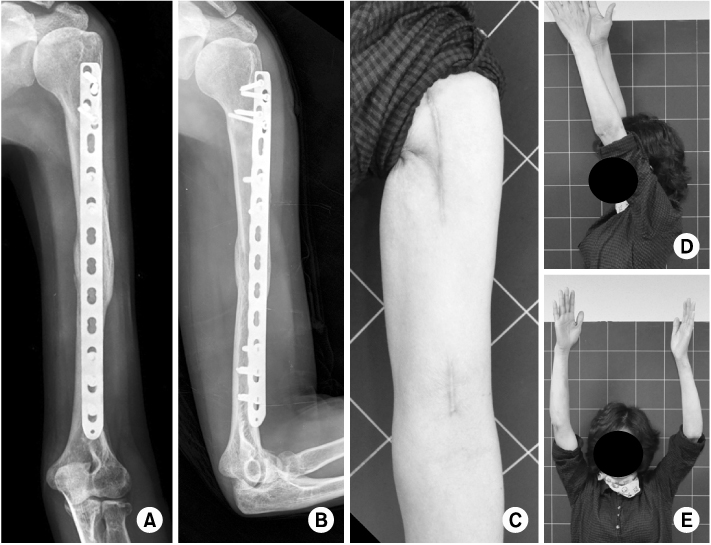
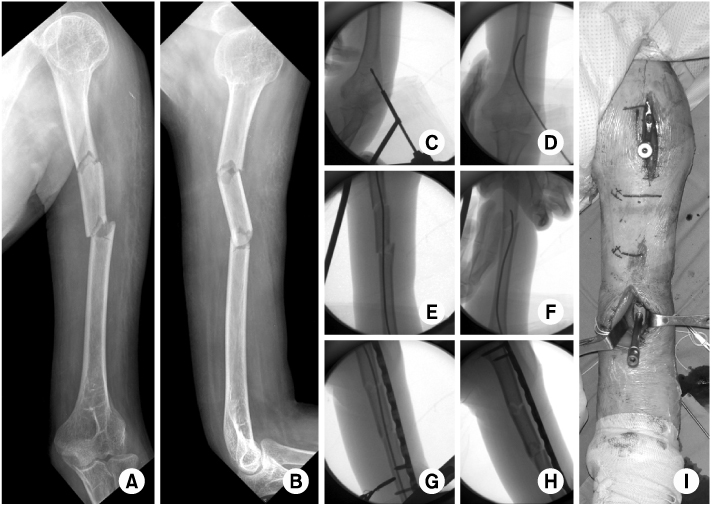
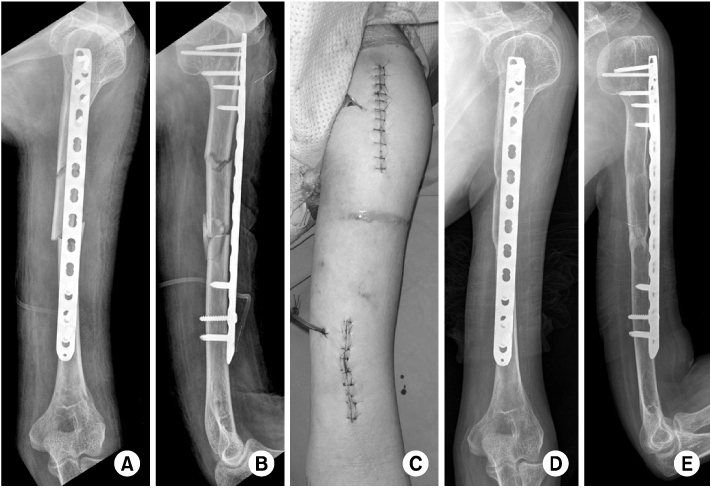
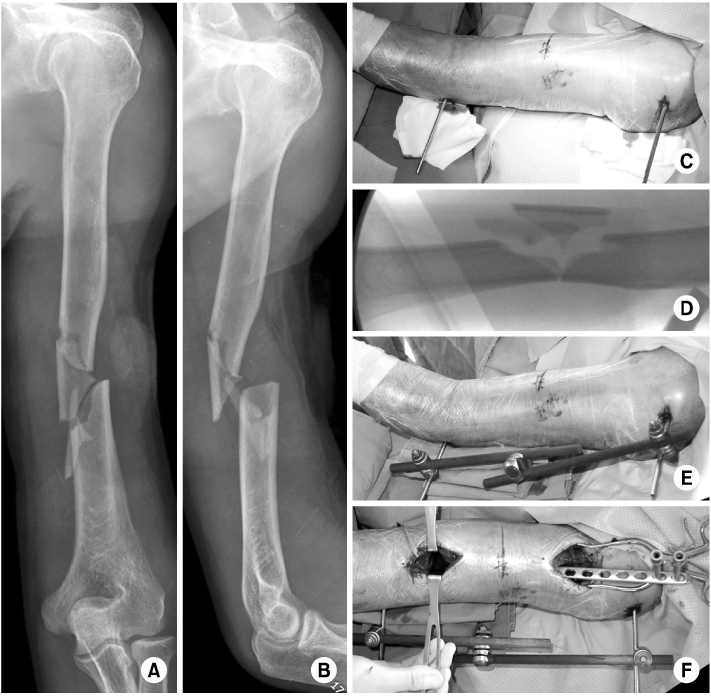
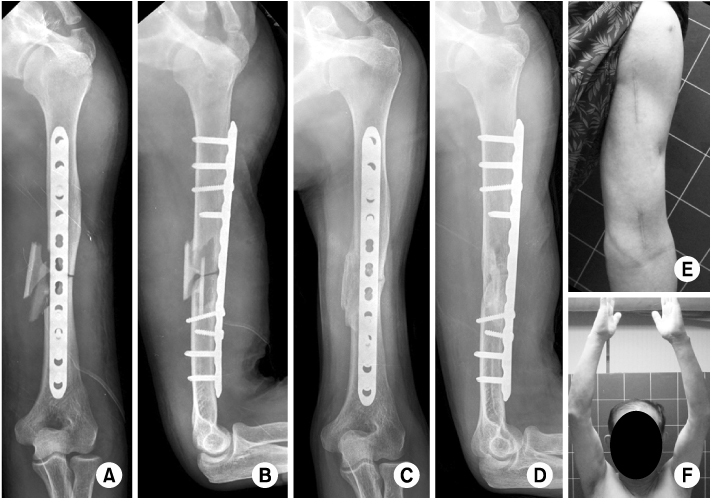
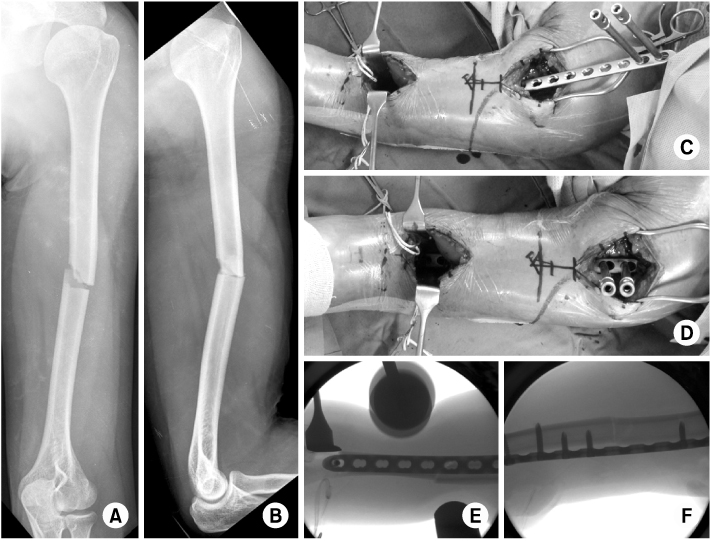
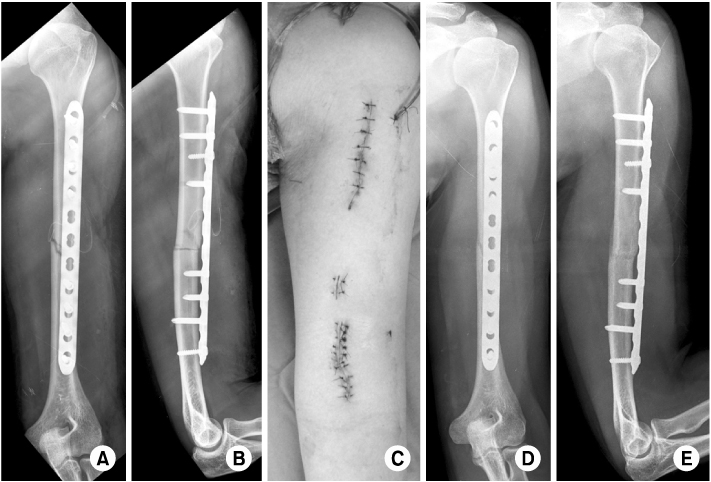
Fig. 1
(A, B) A 41-year-old female with segmental fracture of the humerus shaft, which is AO/OTA classification C2.
(C, D) Intraoperative fluoroscopic images showing Schanz screws is inserted from the lateral sides of the greater tuberosity and lateral condyle of the humerus with the distal and proximal fragments faced anteriorly. Note that insertion point to avoid injury to the radial nerve.
(E) Reduction is maintained with a unilateral external fixator. A roll of elastic bandage can be used.
Fig. 2
(A~D) A metaphyseal locking compression plate is inserted from the proximal incision while maintaining reduction with external fixator. The position of the plate is determined by fluoroscopy. Kirschner wires are used for provisional fixation of the plate.
(E~G) Immediate postoperative radiographs showing acceptable alignment. The screws are inserted under direct visualization through the proximal and distal incisions.
Fig. 3
(A, B) Radiographs taken eight months after the index surgery show complete bone healing.
(C~E) Minimal scar with nearly full range of motion in the shoulder and elbow joints.
Fig. 4
(A, B) A 61-year-old male with AO/OTA classification C2 fracture of the humerus.
(C~H) The fracture is reduced and maintained by utilizing a elastic nail inserted from the lateral condyle of the humerus.
(I) After making a submuscular tunnel, a locking plate is inserted. Locking drill sleeves can be used as a handle. Note that biceps brachii muscle, split medial part of the brachialis, and the cutaneous brance of the musculocutaneous nerve is retracted medially at the distal incision.
Fig. 5
(A~C) Immediate postoperative radiographs and picture of the surgical wound.
(D, E) Radiographs show complete healing of the fracture eight months after the index surgery.
Fig. 6
(A, B) A 64-year-old male showed comminuted humerus shaft fracture of AO/OTA classification B3.
(C~E) Indirect reduction and maintaining reduction was assisted by a unilateral external fixator.
(F) A locking compression plate is introduced into submuscular tunnel.
Fig. 7
(A, B) Immediate postoperative radiographs show reduced fracture in anatomical alignment.
(C, D) Nine months after the index surgery, radiographs show complete healing.
(E, F) Minimal scar with recovered range of motion in the shoulder and elbow joints.
Fig. 8
(A, B) A 30-year-old male sustained simple, transverse fracture of the humerus shaft (AO/OTA classification A3).
(C~F) Submuscular plating under the fluoroscopy guidance.
Fig. 9
(A~C) Immediate postoperative radiographs and picture of the surgical wound. Percutaneous insertion of screws is used with caution because of possible injury to the musculocutaneous nerve.
(D, E) Radiographs show complete healing in anatomical alignment ten months after the index surgery.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Operative Treatment of Humerus Shaft Fracture: Conventional Open Plating or Minimally Invasive Plate Osteosynthesis

