 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 36(3); 2023 > Article
- Original Article Outcomes of Minimally Invasive Surgery in Intra-Articular Calcaneal Fractures: Sanders Type III, Joint Depressive Type Calcaneal Fracture
- Je Hong Ryu, Jun Young Lee, Kang Yeol Ko, Sung Min Jo, Hyoung Tae Kim
-
Journal of Musculoskeletal Trauma 2023;36(3):85-94.
DOI: https://doi.org/10.12671/jkfs.2023.36.3.85
Published online: July 31, 2023
Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea
- 1,127 Views
- 3 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
To evaluate the radiologic and clinical outcomes of a minimally invasive technique using the tarsal sinus approach in the management of Sanders type III, joint depressive type calcaneal fractures.
Materials and Methods
Between July 2011 and September 2019, data of 29 patients who underwent a minimally invasive procedure with the sinus tarsi approach for Sanders type III joint depressive intra-articular calcaneal fractures, and were followed up for more than 1 year were analyzed. We evaluated the radiologic outcomes by assessing the radiologic parameters (Böhler angle, Gissane angle, calca-neal length, calcaneal height, calcaneal width). We also evaluated the clinical outcomes based on the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score and the complications associated with the technique.
Results
The radiological results showed an improvement in the Böhler angle from 2.5° to 18.6° and the Gissane angle from 132.4° to 119.1° after the operation. The mean AOFAS score during the clini-cal evaluation was 79.5. We observed 13 cases of posttraumatic arthritis, 1 case of subtalar arthrodesis, and no case of wound complication.
Conclusion
Minimally invasive technique for Sanders type III joint depressive calcaneal fractures resulted in relatively satisfactory radiologic and clinical outcomes. Open reduction and internal fixation through the sinus tarsi approach reduce complications including wound problems. This approach offers satisfactory results without long-term complications.
J Korean Fract Soc. 2023 Jul;36(3):85-94. Korean.
Published online Jul 21, 2023.
https://doi.org/10.12671/jkfs.2023.36.3.85
Published online Jul 21, 2023.
https://doi.org/10.12671/jkfs.2023.36.3.85
Copyright © 2023 The Korean Fracture Society.
Original Article
종골 관절내 골절에서 최소 침습적 내고정술의 결과: Sanders III형의 관절 함몰형 종골 골절
Outcomes of Minimally Invasive Surgery in Intra-Articular Calcaneal Fractures: Sanders Type III, Joint Depressive Type Calcaneal Fracture
Je Hong Ryu , M.D.,
Jun Young Lee, M.D., Ph.D.,
Kang Yeol Ko, M.D.,
Sung Min Jo, M.D.
and Hyoung Tae Kim, M.D.
, M.D.,
Jun Young Lee, M.D., Ph.D.,
Kang Yeol Ko, M.D.,
Sung Min Jo, M.D.
and Hyoung Tae Kim, M.D.
, M.D.,
Jun Young Lee, M.D., Ph.D.,
Kang Yeol Ko, M.D.,
Sung Min Jo, M.D.
and Hyoung Tae Kim, M.D.
초록
목적
Sanders III형의 관절 함몰형 종골 골절에서 족근동 접근법을 통한 최소 침습적 내고정술 시행 후 방사선학적 및 임상적 결과를 분석하고자 한다.
대상 및 방법
2011년 7월부터 2019년 9월까지 본원에서 치료한 Sanders III형의 관절 함몰형 종골 골절 환자 중 족근동 접근법을 통한 최소 침습적 수술 후 1년 이상 추시한 29예를 대상으로 하였고, 방사선학적 및 임상적 평가, 합병증 발생에 대해 조사하였다.
결과
방사선학적 검사상 Böhler 각 및 Gissane 각의 유의미한 호전을 보였고, 임상적인 평가를 위한 AOFAS 발목 점수상 평균 79.5점이었다. 합병증의 경우 창상 감염은 없었으며, 외상 후 관절염 13예, 그 중 1예에서는 거골하 관절 유합술을 시행하였다.
결론
Sanders III형의 관절 함몰형 종골 골절에서 족근동 접근법을 이용한 최소 침습적 내고정술은 방사선학적 및 임상적으로 만족스러운 결과를 보였다.
Abstract
Purpose
To evaluate the radiologic and clinical outcomes of a minimally invasive technique using the tarsal sinus approach in the management of Sanders type III, joint depressive type calcaneal fractures.
Materials and Methods
Between July 2011 and September 2019, data of 29 patients who underwent a minimally invasive procedure with the sinus tarsi approach for Sanders type III joint depressive intra-articular calcaneal fractures, and were followed up for more than 1 year were analyzed. We evaluated the radiologic outcomes by assessing the radiologic parameters (Böhler angle, Gissane angle, calcaneal length, calcaneal height, calcaneal width). We also evaluated the clinical outcomes based on the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot score and the complications associated with the technique.
Results
The radiological results showed an improvement in the Böhler angle from 2.5° to 18.6° and the Gissane angle from 132.4° to 119.1° after the operation. The mean AOFAS score during the clinical evaluation was 79.5. We observed 13 cases of posttraumatic arthritis, 1 case of subtalar arthrodesis, and no case of wound complication.
Conclusion
Minimally invasive technique for Sanders type III joint depressive calcaneal fractures resulted in relatively satisfactory radiologic and clinical outcomes. Open reduction and internal fixation through the sinus tarsi approach reduce complications including wound problems. This approach offers satisfactory results without long-term complications.
Keywords
Calcaneus, Intraarticular fractures, Minimally invasive surgery, Sinus tarsi
종골, 관절내골절, 최소 침습적 수술, 족근동
서론
종골은 족부에서 가장 큰 뼈로 해면골이 많은 부분을 차지하고 있으며 기능적으로 몸무게를 지탱하고 외측주의 길이를 유지하며 후내측 구조물들을 보호한다. 생역학적으로 하퇴 삼두근에 대한 지렛대 기능을 하며 족관절과 후족부 기능에 있어 매우 중요한 역할을 한다.1,2)
이러한 종골의 골절은 전체 골절의 2%를 차지하며3) 대부분 교통사고나 추락과 같은 고에너지 손상으로 발생하기 때문에 분쇄가 심하다. 종골은 해부학적 구조가 복잡하고 해면골이 많아서 분쇄와 함몰이 많고, 전위를 동반한 관절내 골절이 60%-70%를 차지하며, 주변 연부조직의 손상 등의 이유로 정형외과 의사에게 어려운 골절 중 하나이다.
Essex-Lopresti는 1952년 단순 방사선 촬영을 바탕으로 관절 골편이 조면 조각에 부착된 설상형 골절과 관절 골편이 인접한 조면과 분리된 관절 함몰형 골절의 2가지 관절 손상 형태를 제시하였으며(Fig. 1),4) Sanders 등5)은 관상면을 기준으로 관절면의 골절을 분류하였다(Fig. 2).
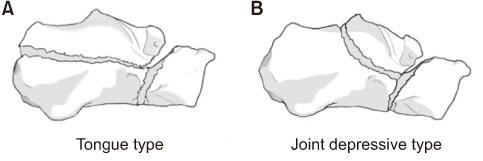
Fig. 1
Essex-Lopresti classification. (A) Tongue-type fracture, where the articular fragment remained attached to a tuberosity fragment. (B) Joint depressive-type fracture, in which the articular fragment was separate from the adjacent tuberosity.
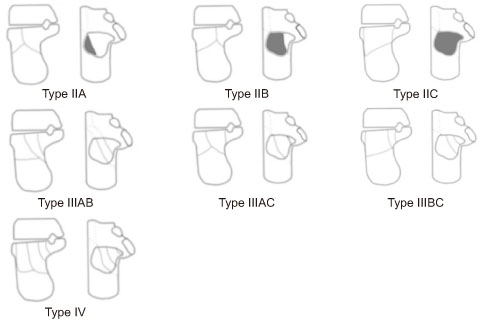
Fig. 2
Sanders classification based on computed tomography images in the coronal plane. Type I fracture includes all non-displaced articular fractures (less than 2 mm). Type II fractures are two-part fractures of the posterior facet. Three types—IIA, IIB, and IIC—are based on the location of the primary fracture line. Type III fractures are three-part fractures that usually feature a centrally depressed fragment. Types included IIIAB, IIIAC, and IIIBC were based on the location of the primary fracture line. Type IV fractures were highly comminuted and often had more than four articular fragments.
종골 골절은 골절 양상에 따라 정해진 치료법이 있는 것은 아니지만 크게 비수술적 치료, 관혈적 정복 및 내고정술, 최소 침습적 내고정술, 일차 거골하 관절 유합술로 나눠 볼 수 있다.6)
수술적 치료의 적응증으로는 전위성 관절내 골절, 종골의 전방돌기 골절(종입방 관절이 25% 이상 포함된 경우), 종골조면의 전위성 골절, 종골의 골절 탈구, 개방성 종골 골절이 해당한다. 이 중 전위를 동반한 관절내 종골 골절의 치료는 비수술적 치료와 수술적 치료에 따른 결과가 상당 부분 예측하기 어려워 논의의 대상이 되어 왔다.7,8,9) 그러나 최근 수술적 치료를 통한 해부학적 정복 및 관절면 회복, 종골 모양의 회복, 그리고 안정적인 고정을 해 기능적으로 조기 회복을 유도하면서 외상 후 관절염과 같은 합병증을 최소화하는 것이 비수술적 치료에 비해 좋은 결과를 보인다.6,9,10,11,12,13)
수술을 위한 접근법으로는 분쇄가 심한 관절내 골절을 동반하는 경우가 많으므로 광범위 외측 접근법을 이용한 관혈적 정복술 및 금속판 고정술이 주로 사용되어 왔다.14,15) 하지만 이 접근법은 수술 후 피부괴사 등 창상 문제, 비복신경 손상 등 합병증 발생빈도가 1.8%-27%까지 보고되고 있다.16,17)
족근동 접근법(sinus tarsi approach)은 최소 침습적 수술법으로 광범위 외측 도달법의 가장 큰 단점인 창상 문제를 줄이고 수술 시간 또한 줄일 수 있으며 족근동을 통한 후관절면을 직접 보면서 정복이 가능하다는 장점이 있어 최근 사용 비율이 점차 증가하고 있으며, 결과에 대해 많은 보고가 있으나 Sanders III형의 관절 함몰형 종골 골절에 적용한 연구는 드물다.6,18,19)
따라서 본 연구에서는 Sanders III형의 관절 함몰형 종골 골절에서 족근동 접근법을 이용한 최소 침습적 내고정술 시행 후 방사선학적 및 임상적 결과를 분석하고자 한다.
대상 및 방법
1. 연구 대상
2011년 7월부터 2019년 9월까지 조선대학교병원에서 치료한 종골 골절 환자 183명(209예) 중 관절외 골절은 43예, 관절 함몰형 153예, 설상형 골절 13예였다. 관절 함몰형 153예(130명) 중에서 Sanders III형은 68예로, 양측 골절인 경우 14예와 광범위 외측 접근법으로 수술한 17예, 외래 추시 기간이 1년 미만인 8예를 제외한 29예를 대상으로 하였고, 평균 연령은 48.7세(범위 20-74세)였으며, 남자 23명, 여자 6명이었다. 개방성 골절은 없었다(Table 1). 본 연구는 조선대학교병원 기관생명윤리위원회(Institutional Review Board, IRB)의 승인(IRB No. 2020-09-004)을 받아 후향적으로 시행하였으며, 후향적 의무기록 연구로 환자 서면동의서는 IRB에 의해 면제 받았다.
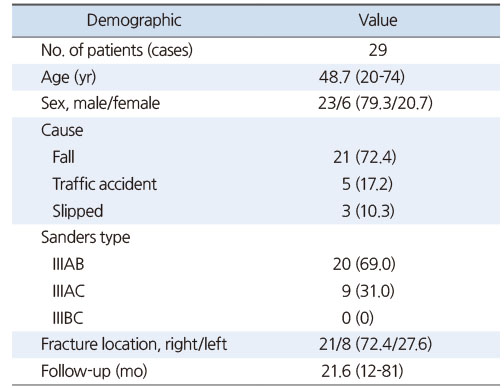
Table 1
Demographic Data of the Patients
2. 원인 및 동반 손상
골절의 원인으로는 추락사고가 21예(72.4%)로 가장 많았으며 교통사고가 5예(17.2%), 실족이 3예(10.3%)였다(Table 1). 11명(37.9%)에서 동반 손상을 보였으며 복사뼈를 포함한 경골 골절이 6예(20.7%)로 가장 많았고 족부 골절이 4예(13.8%), 대퇴골 골절, 척추 골절이 각각 3예(10.3%), 늑골 골절이 2예(6.9%)였다.
3. 수상 후 수술까지의 시간
수상 후 수술까지 평균 8.8일(범위 4-21일)이었고, 환자의 동반 손상 및 전신 상태, 골절 부위의 부종을 포함한 피부 상태를 고려하여 수술 시기를 결정하였다. 수술 부위 부종의 경우 하지 거상, 붕대 압박, 얼음찜질을 통해 감소시켰다.
4. 수술 방법
전신마취 또는 척추 마취 후 환측이 위로 오도록 측와위로 눕힌 다음 환측 하지에 지혈대(tourniquet)를 착용하였다. 소독 및 드레이프(drape)를 시행한 뒤 족근동 접근법을 위해 족근동을 중심으로 외과 1 cm 하방에서 종골 전외측면을 따라 종입방관절(calcaneocuboid joint) 전방까지 4 cm가량 피부를 절개하였다. 비골근 및 비복신경의 손상에 주의하면서 연부조직을 박리하고 골절 부위를 노출시킨다. Schantz 핀을 조면 골편(tuberosity fragment)에 고정한 후 하방 견인 및 외반력을 주면서 종골 높이를 회복한다. 정복을 유지하면서 프리어(freer)를 이용하여 함몰된 관절면을 거상 후 C-arm 영상으로 관절면의 정복 정도를 확인하고, 필요하다면 4.0 mm 유관 나사(4CIS® 4.0 mm Cannulated Screw [Titanium]; Solco Biomedical, Pyeongtaek, Korea)를 이용하여 정복된 골편과 제거돌기 골편을 고정한다. 종골 조면 상방에서 입방골 관절면 방향으로 일차 골절선을 지나 축방향으로 6.5 mm 유관 나사(4CIS® 6.5 mm Cannulated Screw [Titanium]; Solco Biomedical)를 이용하여 고정한다. 이어 종골 조면 하방에서 입방골을 향해 골절선을 지나 6.5 mm 유관 나사와 K-강선을 추가로 고정하고, C-arm 영상으로 측면, 축상 방사선사진으로 종골의 높이, 내반 교정 및 함몰된 관절면의 정복이 양호함을 확인한 후 골결손 부위에 대해 동종 골편을 이용하여 골이식을 하고, 세척 및 지혈 후 피부 봉합을 하고, 단하지 부목고정을 한다(Fig. 3).
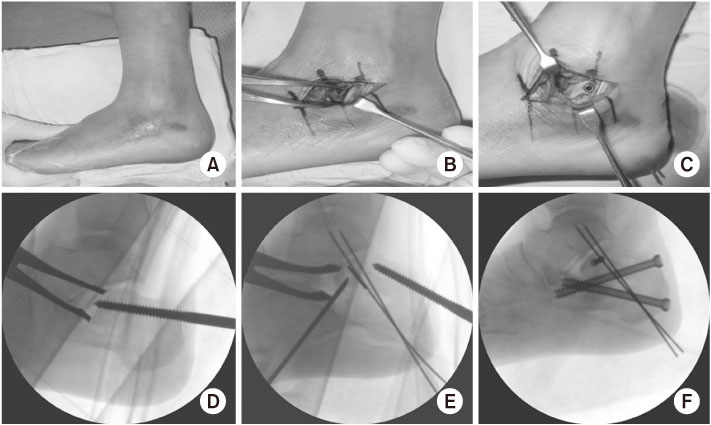
Fig. 3
Surgical technique (sinus tarsi approach and C-arm X-ray). Skin incision from the tip of the fibula toward the calcaneocuboid joint on sinus tarsi. Posterior facet and fracture site was exposed by soft tissue dissection (A, B). Reduction through gentle traction and valgus force using the Scantz pin in calcaneal tuberosity (D). After temporary fixation using a K-wire for the subtalar joint (E), the definitive fixation using 4.0-mm and 6.5-mm cannulated screws was performed (F). Photo after definitive fixation (C).
5. 수술 후 재활
수술 후 단하지 부목고정을 유지하면서 14일째 실밥 제거 후 단하지 석고고정으로 4주간(수술 후 6주) 적용하였다. 이후 석고고정 제거 후 능동적 관절운동 및 부분 체중부하를 시행하였고, 수술 후 12주째 전 체중부하 보행을 시행하였다.
6. 평가
방사선학적 평가로 응급실 내원 시 단순방사선 사진 촬영(전후면상, 측면상, 축상)과 컴퓨터 단층촬영을 시행하였으며 수술 후 방사선 사진(전후면상, 측면상, 축상), 마지막 외래에서 촬영한 단순방사선 사진(전후면상, 측면상, 축상)을 통해 Böhler 각, Gissane 각, 종골 높이, 종골 길이, 종골 너비를 측정하였다(Fig. 4,5,6,7). Böhler 각의 경우 측면상 사진에서 종골 후방 관절의 상방에서 거골 조면 상방과 접하는 선과 전방돌기의 상방과 접하는 선이 이루는 각이며, Gissane 각 역시 측면상 사진에서 종골의 후방 관절면과 전방 돌기가 이루는 각이다. 종골 높이는 측면상 사진에서 종골 하면에서 접하는 선과 종골의 가장 높은 곳까지의 직선거리로 하였으며, 종골 길이 역시 측면상 사진에서 종골의 가장 앞쪽과 가장 뒤쪽의 거리로 측정하였다. 종골 너비의 경우 축상 사진에서 재거돌기를 포함한 최장 길이로 확인하였다(Fig. 7).
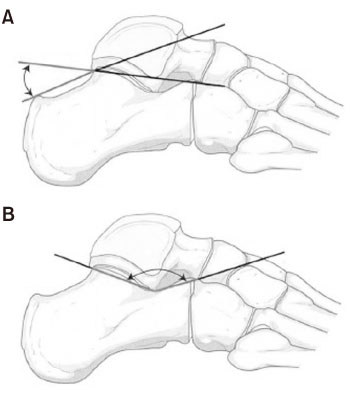
Fig. 4
(A) Böhler angle. (B) Gissane angle. The Böhler angle comprises a line drawn from the highest point of the anterior process of the calcaneus to the highest point of the posterior facet and a line drawn tangential to the superior edge of the tuberosity. The Gissane angle is formed by the downward and upward slopes of the calcaneal superior surface.

Fig. 5
Preoperative radiography. Preoperative X-ray (A: ankle lateral view, B: calcaneal axial view). It is a joint depressive calcaneal fracture, the posterior joint surface is depressive and the Böhler angle is reduced on the lateral view. The lateral wall is bulging on the calcaneal axial view. Preoperative computed tomographies (C: sagittal view, D: semicoronal view) show a joint depressive type, Sanders type IIIAB calcaneal fracture.

Fig. 6
Postoperative radiography. Postoperative X-ray (A: ankle lateral view, B: calcaneal axial view). Böhler angle and Gissane angle have recovered (Böhler angle is 32.2°, Gissane angle is 105.5°, calcaneal length is 79.4 mm, calcaneal height is 44.0 mm, calcaneal width is 52.0 mm). Computed tomographies after 4 months of surgery (C: sagittal view, D: semicoronal view) show a well articular fracture reduction.
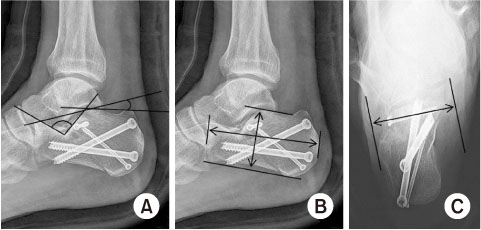
Fig. 7
Radiologic Assessment. (A) Ankle lateral X-ray, Gissane angle, Böhler angle. (B) Ankle lateral X-ray, calcaneal height, calcaneal length. (C) Calcaneal axial view, calcaneal width. The calcaneal height and calcaneal length were measured at the highest and lowest length and the longest length from anterior to posterior in the lateral X-ray. Calcaneal width measures the widest width including sustentaculum tali on the calcaneal axial view.
골유합은 방사선 전후면상, 측면상과 축상 사진상 최소 세개 이상의 피질골에서 골유합이 보이고 체중부하 시 통증이 없는 경우로 정의하였다.
임상적 평가로는 최종 추시 시 미국 족부정형외과 족관절 및 후족부 평가표(American Orthopedic Foot and Ankle Society [AOFAS] ankle-hindfoot score)를 이용하여 분석하였고, 90점 이상을 매우 만족, 80점 이상을 만족, 70점 이상을 보통, 70점 이하는 불만족으로 평가하였다. 수술 후 창상 감염, 후외상성 관절염으로 인한 거골하 관절 유합술 시행 여부를 확인하였다.
통계 분석은 IBM SPSS Statistical software 26.0 (IBM, Armonk, NY, USA)을 사용하였으며 모든 측정은 2명의 정형외과 의사가 한 뒤, 측정 후 측정자 간 신뢰도는 급내상관계수(intraclass correlation coefficient, ICC)를 이용하여 확인하였다. 수술 전과 수술 후, 마지막 외래에서의 Böhler 각, Gissane 각, 종골 높이, 종골 길이, 종골 너비를 대응표본 t 검정(paired t-test)으로 확인하였다.
결과
모든 환자에서 평균 17주(범위 10-44주)에 골유합을 얻었고, 평균 추시 기간은 21.6개월(범위 12-81개월)이었다. 6.5 mm 유관 나사의 경우 1예에서만 3개를 사용하였고 나머지 28예에서 2개를 사용하였으며, 4.0 mm 유관 나사의 경우 평균 1.0±0.9개(범위 0-4개), K-강선의 경우 평균 0.6±0.9개(범위 0-3개)를 사용하였다.
Böhler 각의 경우 수술 전 평균 2.5°±11.7° (범위 –18.2°-24.9°)에서 수술 직후 평균 18.6°±5.0° (범위 11.4°-27.2°)로 회복되었으며(p<0.001), 마지막 외래 추시 때 평균 18.7°±4.6° (범위 12.1°-27.6°)로 유의미한 변화 없이 유지되었다(p=0.802). Gissane 각의 경우 수술 전 평균 132.2°±9.0° (범위 115.7°-158.8°)에서 수술 직후 평균 119.1°±8.4° (범위 106.1°-133.2°)로 감소하였으며(p<0.001), 마지막 외래 추시 때 평균 119.4°±7.3° (범위 108.2°-132.7°)로 유의미한 변화 없이 유지되었다(p=0.824). 종골 길이의 경우 수술 전 평균 78.3±4.2 mm (범위 68.2-86.0 mm)에서 수술 직후 평균 79.1±5.6 mm (범위 70.7-93.8 mm)로 큰 변화가 없었으며(p=0.295), 마지막 외래 추시 때 평균 79.7±4.9 mm (범위 71.8-90.7 mm)였다(p=0.401). 종골 높이의 경우 수술 전 평균 38.8±4.2 mm (범위 30.5-49.8 mm)에서 수술 후 평균 44.7±3.2 mm (범위 37.7-53.7 mm)로 회복되었으며(p<0.001), 마지막 외래 추시 때 평균 45.4±3.1 mm (범위 39.4-54.1 mm)였다(p=0.014). 종골 너비의 경우 수술 전 평균 60.9±6.7 mm (범위 49.8-80.8 mm)에서 수술 후 평균 59.5±5.3 mm (범위 49.8-72.8 mm)로 감소하였으나 통계적으로 유의미하지 않았고(p=0.116), 마지막 외래 추시 때 평균 59.1±5.0 mm (범위 48.8-68.8 mm)였다(p=0.406) (Table 2).

Table 2
Results of Radiologic Assessment
임상적인 평가를 위해 시행한 AOFAS ankle-hindfoot score는 평균 79.5±4.9점(범위 67-88점)이었고, 매우 만족 0예, 만족 11예, 보통 7예, 불만족 1예로 비교적 양호한 결과를 보였다.
합병증의 경우 창상 감염은 모든 환자에게서 나타나지 않았으며, 외상 후 관절염의 경우 13예에서 확인되었고 12예에서는 약물을 통해 조절 중이며 약물치료에도 통증의 호전을 보이지 않은 1예에서 수술 후 7개월째 금속나사 제거술을 시행하였으나 증상이 지속되어 8개월째 거골하 관절 유합술을 시행하였다(Fig. 8). 1예에서 나사에 의한 자극 증상으로 불편감을 호소하여 제거하였고, 이를 포함한 23예에서 수술 후 평균 12.4±2.9개월(범위 7-19개월) 시점에 금속제거술을 시행하였다(Table 3).
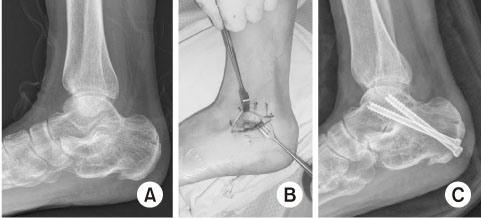
Fig. 8
Case of subtalar arthrodesis. A 51-year-old male patient underwent subtalar arthrodesis, 8 months after his first surgery. (A) Preoperative ankle lateral X-ray shows post-traumatic osteoarthritis of the subtalar joint. (B) Subtalar arthrodesis was done using the sinus tarsi approach. (C) Postoperative ankle lateral X-ray.
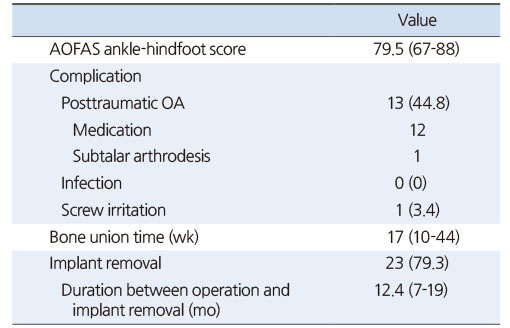
Table 3
Results of Clinical Assessment
측정자 간 신뢰도 ICC는 Böhler 각 0.80, Gissane 각 0.79, 종골 높이 0.89, 종골 길이 0.90, 종골 너비 0.85로, Gissane 각에서는 중등도의 신뢰도를 보이고 나머지 항목에서는 높은 신뢰도를 보였다.
고찰
종골 골절 치료의 공통된 목표는 (1) 거골하 관절의 후방 관절면의 회복, (2) 종골 높이의 회복, (3) 종골 너비의 회복, (4) 비골건을 위한 비골하 공간의 감압, (5) 외반족 자세로 조면을 조정, (6) 종입방 관절의 골절 정복이다.
수술적 치료의 방법으로 많이 사용되던 광범위 외측 접근법은 비골 원위부 2-3 cm 근위부부터 비골 후방과 아킬레스건의 외측으로 종절개를 한 뒤, L자 모양으로 뒤꿈치 지방층과 족부 외측 피부 경계를 따라 발바닥과 평행하게 절개하는 수술법으로, 관절내 골절 및 종골의 외벽을 포함하는 관절외 골절에서 매우 훌륭한 시야를 제공하는 접근법이나 광범위한 피부 및 연부조직 절개, 골절 부위 골막 손상, 혈관 및 비복 신경 손상 등의 합병증 발생이 많다는 단점이 있다.16,17,20,21)
이와 비교하여 족근동 접근법을 이용한 최소 침습적 수술은 외측 접근법에 비해 창상 문제 및 혈관, 비복 신경의 손상을 줄일 수 있으며 수술 시간을 줄이고 만족스러운 결과를 얻을 수 있다.22,23) 또한 최소 침습적 내고정술은 해부학적 정복 및 안정적인 고정으로 조기 관절운동을 가능하게 해주지만, 광범위 외측 접근법에 비해 시야가 좁아 모든 골편을 정복하거나 고정할 수 없다는 단점이 있다. 특히 종골 외벽의 돌출을 줄이기 어렵다. 이러한 이유로 본 연구기간 중 후관절 골절 양상이 Sanders III형에 해당하지만 후관절을 제외한 종골 다른 부위 골절 양상이 분쇄가 매우 심하여 족근동 접근법만으로는 정복이 어렵겠다고 판단되어 광범위 외측 접근법을 사용한 17예는 연구에서 제외하였다.
Bedigrew 등18)은 카데바 연구를 통해 광범위 외측 접근법과 족근동 접근법을 비교하였고, 족근동 접근법이 외측벽을 보기 어려웠으나 관절면의 노출은 광범위 외측 접근법과 비슷하게 노출시켰고 정복 또는 좋은 결과를 보였다고 보고하였다. Rammelt 등24)은 최소절개 및 경피적 나사못 고정술로 만족스러운 임상 결과 및 정상에 가까운 Böhler 각을 얻었다고 보고하면서 복잡 골절, 개방성 골절이 있으면서 당뇨병이나 흡연 등의 위험인자가 있는 환자에서도 권장할 만한 치료 방법이라고 소개하였다. Carr25)은 최소 절개 방법으로도 후방 관절면의 충분한 시야를 확보할 수 있으며 종골 관절 내 골절의 정복도 가능하다고 소개하였다. Meraj 등21)도 족근동 접근법을 이용한 최소 침습적 수술을 통해 Böhler 각 및 Gissane 각, 종골 높이 및 너비와 임상 점수 역시 좋은 결과를 보였으며 합병증 역시 발생하지 않았다고 보고하였다. 이렇듯 창상 문제 등을 줄이기 위해 최소 침습적 내고정술의 비율이 점차 증가하고 있는 추세이나 Sanders 등5)의 관절 함몰형 종골 골절에 적용한 연구는 드물며, 본 연구에서는 Sanders III형의 관절 함몰형 종골 골절에서 족근동 접근법을 이용한 최소 침습적 내고정술을 시행하여 양호한 결과를 얻었다.
본 연구에서 종골 너비의 경우 수술 전 평균 60.9±6.7 mm (범위 49.8-80.8 mm)에서 수술 후 평균 59.5±5.3 mm (범위 50.0-72.9 mm)로 감소하였으나 통계적으로 유의미하지 않았고(p=0.116), 마지막 외래 추시 때 평균 59.1±5.0 mm (범위 49.8-72.8 mm)였다(p=0.406) (Table 2). 이는 종골 골절 목표 중 비골건을 위한 비골하 공간의 감압이라는 점에서 부족하게 보여질 수 있으나 본 연구에서 비골건 문제를 호소하는 사례는 없었다. 이는 수술 중 술자가 족근동 접근법에서 보이는 외측 벽의 근위부를 최대한 정복 및 하방으로 이동시켜 비골건을 위한 공간을 확보하나 측정 시에는 축상 사진에서 재거돌기를 포함한 최장 길이로 확인하였기에 본 연구에서 사용된 종골 너비 측정법이 비골건 문제를 반영하지 못했을 가능성이 있거나, 또는 본 연구의 한계점인 적은 환자 수와 길지 않은 추시 기간으로 인해 발생한 문제라고 생각된다.
Loucks와 Buckley26)는 종골 골절에서 종골 높이 소실로 인한 Böhler 각의 소실은 결과에 매우 중요한 부정적 요소라고 하였으며, Csizy 등27)은 Böhler 각이 편평하거나 음각을 보일 경우 그렇지 않은 군에 비해 거골하 관절 유합술의 가능성이 올라간다고 하였다. 따라서 비수술적 치료보다 수술적 치료를 통한 Böhler 각의 회복이 종골 치료에 있어 중요하게 여겨지고 있다.6,12,28) 본 연구에서도 Böhler 각은 수술 전 2.5°에서 수술 후 18.6°로 회복되었고(p<0.001), 마지막 외래 추시 시에도 18.7°로 잘 유지되는 것으로 보였으며(p=0.802), 이는 Jo 등29)의 17예의 관절 함몰형 종골 골절에서 최소 침습적 내 고정술을 시행한 연구에서 수술 전 7.9°에서 수술 후 19.8°로 회복된 것과 비슷한 결과이다. 다른 연구들과 비교하였을 때 Kikuchi 등30)의 연구에서 22예의 종골 골절 수술을 시행하였으며 Böhler 각이 수술 전 13.3°에서 수술 후 22.1°로 회복된 소견을 보였다. Biggi 등31)의 연구에서 Böhler 각은 수술 전 9.9°에서 수술 후 22.1°로 회복된 소견을 보였다. 이 외에도 van Hoeve와 Poeze22)가 보고한 1,776명(2,018예)의 종골 골절을 포함한 46개의 연구를 대상으로 한 systematic review에서 Böhler 각은 평균 수술 전 5° (범위 –15°-25°)에서 수술 후 24° (범위 14°-35°)로, 이는 본 연구의 결과 또한 양호하였으며 외래 추시 때까지 잘 유지되었다고 볼 수 있다.
본 연구에서 Gissane 각은 수술 전 132.2°에서 수술 후 119.1° 및 마지막 외래 추시 때 119.4°로 유지되었다. Jo 등29)의 연구에서는 수술 전 102.1°에서 수술 후 116.2°, 마지막 외래 추시 때 115.1°로 보고하였고 이와 비교하였을 때 수술 전 Gissane 각은 차이가 크나 수술 후 모두 양호하게 회복되었다. 다른 연구들과 비교하였을 때 Kikuchi 등30)이 시행한 22예의 연구에서 수술 전 133.6°에서 수술 후 134°로 변화가 없었다. Kesemenli 등32)의 연구에서는 수술 전 100.7°에서 수술 후 112°로 회복된 소견을 보였으며, van Hoeve와 Poeze22)가 보고한 1,776명(2,018예)의 종골 골절을 포함한 46개의 연구를 대상으로 한 systematic review에서 Gissane 각은 수술 전 115°에서 수술 후 119°로 측정되었다. 따라서 본 연구에서의 Gissane 각은 다른 연구들과 비슷하게 잘 회복되었음을 알 수 있다.
Suh 등19)은 Sanders II형과 III형에 한해서 15예의 최소 침습 접근법을 통한 금속판 고정술과 64예의 광범위 외측접근법을 통한 금속판 고정술을 비교하였으며, 방사선학적 측정에서는 두 군 간의 차이가 적었으나 AOFAS 점수는 각각 90점, 80점으로 최소 침습 접근법을 이용한 군에서 유의미하게 높게 나타났으며, 내번(inversion)과 외번(eversion)을 통해 측정한 관절운동 범위에서 각각 최소 침습 접근법을 이용한 군이 유의미하게 높게 나타났다. 따라서 Sanders II, III형에서 최소 침습 접근법을 이용한 금속판 고정술이 광범위 외측 접근법을 통한 금속판 고정술과 비교하여 비슷한 정도의 정복 및 높은 기능 점수를 보이므로 좋은 대안이 될 수 있다고 주장하였다.
골절로 함몰된 관절면을 정복하면서 종골 높이를 회복하는 과정에서 발생한 해면골의 결손 부위에 대해서는 골이식에 관한 여러 연구 결과들이 있다. 골이식을 할 경우 골유합 시까지 회복된 관절면의 유지와 골절 치유 촉진 효과가 있는 것으로 알려져 있으나, 수술 시간이 길어지고 자가 골이식의 경우 공여부의 추가 수술을 요하며 이에 따른 합병증 및 감염 등의 단점도 있다.5,33,34) 이러한 단점들과 함께 여러 저자들은 종골은 혈액 공급이 좋고 해면골이 풍부한 골로서 8주 이내 골 결손 부위에 가골이 생성되며 지연 나사만으로도 정복 유지가 충분하므로 골이식이 꼭 필요하지 않다라고 주장하는 보고들이 있다.5,35,36)
저자들은 수술 중 종골 높이를 회복하면서 관절면을 정복한 뒤 비어 있는 해면골에 대해 동종 골편을 이용하여 골이식을 시행하였고, 본 연구에 포함된 29예 모두에서 후향적으로 확인한 결과 동종 골편 골이식을 시행하였으며 모든 환자에서 골유합을 얻었다. 동종 골편을 이용하였기에 자가골을 얻기 위한 추가적인 수술 부위는 없었으며 수술 시간 또한 큰 차이가 없었고 자가골 채취로 인한 감염 등의 합병증은 없었다. 수술 직후 종골 높이는 44.7±3.2 mm (범위 37.7-53.7 mm)에서 마지막 외래 추시 시 45.4±3.1 mm (범위 39.4-54.1 mm)로 줄어들지 않고 유지되었다(p=0.014).
종골 골절의 합병증으로는 (1) 비골건의 문제(비골 구의 협착, 비골건의 포착 또는 전위), (2) 발뒤꿈치 통증 및 골극 형성, (3) 신경 손상(비복신경, 후경골 신경의 종골 분지) 및 후경골 신경 포착, (4) 복합 부위 동통 증후군, (5) 수술 부위 피부 괴사 및 종골 골수염, (6) 거골하 관절 및 종입방 관절의 관절염, (7) 부정유합(내반 및 외반 변형), (8) 뒤꿈치 높이가 낮아지고 넓어지는 문제, (9) 지면과 거골 종축 간의 거골 경사각이 감소하여, 거골이 배굴된 상태가 되어 발생하는 발목 관절의 배굴 제한, (10) 아킬레스건의 부착부가 근위부로 이동하여 발생하는 하퇴 삼두근의 약화, (11) 갈퀴 족지 등이 있는 것으로 알려져 있다.37,38) 본 연구에서는 (1) 비골건의 문제, (3) 신경손상 및 후경골 신경 포착, (4) 복합 부위 동통 증후군, (5) 수술 부위 피부 괴사 및 종골 골수염은 발생하지 않았으며, 거골하 관절염이 13예(44.8%)에서 발생하였고 12예에서 약물치료로 조절되었으며 1예에서만 거골하 관절 유합술이 시행되었다.
본 연구에서 29예 모두에서 창상 감염은 관찰되지 않았다. 수술 전후 예방적 항생제를 사용하였고 수술 후 24시간 내에 중단하였다. 본 연구의 계획 당시 실험 대상을 모집하는 과정에서 개방성 골절을 제외하지 않았으나 29예에는 포함되지 않아 개방성 골절에서의 합병증 발생 정도를 비교할 수 없었다. 이는 환자 수가 적어 발생한 한계로 생각되며 수술 시간 및 기저질환 등 감염의 발생에 영향을 미칠 수 있는 요소에 대한 추가적인 평가가 필요할 것으로 생각된다.
본 연구의 제한점으로는 환자 수가 적으며 평균 추시 기간이 21.6개월로 짧다는 점을 들 수 있겠고, 개방성 골절이 포함되지 않았고 Sanders III BC형은 0예였다. Sanders III형임에도 분쇄가 심한 경우 광범위 접근법을 사용한 17예를 제외하였고, 이는 Sanders 분류만으로 설명하기 힘든 골절 양상이 존재하고 이런 경우 족근동 접근법만으로는 좋은 결과를 얻기 어려울 수 있어 후향적 연구인 점과 한 명의 술자가 수술했음에도 어느 정도 선택 편향의 가능성이 있을 것으로 생각된다.
또한, 종골 높이의 경우 수술 직후보다 마지막 외래 추시 시에 약간 증가하였고 이는 통계적으로 의미 있게 나왔으나, 이것은 촬영 당시 족부와 X선 검출기(X-ray detector) 간의 거리 문제와 측정 시의 오류로 인해 모든 예에서 정확한 기준의 측면 촬영이 이루어지지 않았기 때문일 것으로 생각된다.
이 외에도 불유합 등 합병증에 영향을 줄 수 있는 당뇨병과 흡연 등 기저질환(co-morbidities)을 확인하지 않았으며 수술 전 환자의 기능적 능력의 평가 및 수술 후 변화를 고려하지 않았다는 제한점이 있다.
결론
Sanders III형의 관절 함몰형 종골 골절에서 족근동 접근법을 이용하여 최소 침습적 접근법을 통한 내고정술은 방사선학적 및 임상적으로 비교적 만족스러운 결과를 보였다. 따라서 Sanders III형의 관절 함몰형 종골 골절에서 창상 문제를 포함한 합병증을 줄이고 비교적 만족스러운 정복 및 유지가 가능한 족근동 접근법을 통한 내고정술이 좋은 치료방안이 될 수 있을 거라고 생각된다.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Campbell DA. Open reduction and internal fixation of intra articular and unstable fractures of the distal radius using the AO distal radius plate. J Hand Surg Br 2000;25:528–534.
-
-
Park BM, Kim NH, Han DY, Oh DS. A clinical study on the fractures of the calcaneus. J Korean Orthop Assoc 1982;17:697–703.
-
-
Eastwood DM, Gregg PJ, Atkins RM. Intra-articular fractures of the calcaneum. Part I: pathological anatomy and classification. J Bone Joint Surg Br 1993;75:183–188.
-
-
Tornetta P 3rd. The Essex-Lopresti reduction for calcaneal fractures revisited. J Orthop Trauma 1998;12:469–473.
-
-
Sanders R, Fortin P, DiPasquale T, Walling A. Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;(290):87–95.
-
-
Sharr PJ, Mangupli MM, Winson IG, Buckley RE. Current management options for displaced intra-articular calcaneal fractures: non-operative, ORIF, minimally invasive reduction and fixation or primary ORIF and subtalar arthrodesis. A contemporary review. Foot Ankle Surg 2016;22:1–8.
-
-
Randle JA, Kreder HJ, Stephen D, Williams J, Jaglal S, Hu R. Should calcaneal fractures be treated surgically? A meta-analysis. Clin Orthop Relat Res 2000;(377):217–227.
-
-
Shigemasa C, Abe K, Taniguchi S, et al. The influence of diabetes mellitus on thyrotropin response to thyrotropin-releasing hormone in untreated acromegalic patients. J Endocrinol Invest 1988;11:231–237.
-
-
Thordarson DB, Krieger LE. Operative vs. nonoperative treatment of intra-articular fractures of the calcaneus: a prospective randomized trial. Foot Ankle Int 1996;17:2–9.
-
-
Bajammal S, Tornetta P 3rd, Sanders D, Bhandari M. Displaced intra-articular calcaneal fractures. J Orthop Trauma 2005;19:360–364.
-
-
Coughlin MJ. Calcaneal fractures in the industrial patient. Foot Ankle Int 2000;21:896–905.
-
-
Kakwani R, Siddique M. Operative compared with nonoperative treatment of displaced intra-articular calaneal fractures: a prospective, randomized, controlled multicenter trial. In: Banaszkiewicz P, Kader D, editors. Classic papers in orthopaedics. London: Springer; 2014. pp. 229-231.
-
-
Richards PJ, Bridgman S. Review of the radiology in randomised controlled trials in open reduction and internal fixation (ORIF) of displaced intraarticular calcaneal fractures. Injury 2001;32:633–636.
-
-
Tennent TD, Calder PR, Salisbury RD, Allen PW, Eastwood DM. The operative management of displaced intra-articular fractures of the calcaneum: a two-centre study using a defined protocol. Injury 2001;32:491–496.
-
-
Song JH, Kang C, Hwang DS, Kang DH, Park JW. Extended sinus tarsi approach for treatment of displaced intraarticular calcaneal fractures compared to extended lateral approach. Foot Ankle Int 2019;40:167–177.
-
-
Folk JW, Starr AJ, Early JS. Early wound complications of operative treatment of calcaneus fractures: analysis of 190 fractures. J Orthop Trauma 1999;13:369–372.
-
-
Harvey EJ, Grujic L, Early JS, Benirschke SK, Sangeorzan BJ. Morbidity associated with ORIF of intra-articular calcaneus fractures using a lateral approach. Foot Ankle Int 2001;22:868–873.
-
-
Bedigrew KM, Blair JA, Possley DR, Kirk KL, Hsu JR. Comparison of calcaneal exposure through the extensile lateral and sinus tarsi approaches. Foot Ankle Spec 2018;11:142–147.
-
-
Suh JW, Yang JH, Park HW. Clinical results of surgical treatment with minimally invasive percutaneous plate osteosynthesis for displaced intra-articular fractures of calcaneus. J Korean Foot Ankle Soc 2020;24:87–93.
-
-
Kitaoka HB, Schaap EJ, Chao EY, An KN. Displaced intra-articular fractures of the calcaneus treated non-operatively. Clinical results and analysis of motion and ground-reaction and temporal forces. J Bone Joint Surg Am 1994;76:1531–1540.
-
-
Meraj A, Zahid M, Ahmad S. Management of intraarticular calcaneal fractures by minimally invasive sinus tarsi approach-early results. Malays Orthop J 2012;6:13–17.
-
-
van Hoeve S, Poeze M. Outcome of minimally invasive open and percutaneous techniques for repair of calcaneal fractures: a systematic review. J Foot Ankle Surg 2016;55:1256–1263.
-
-
Zeng Z, Yuan L, Zheng S, Sun Y, Huang F. Minimally invasive versus extensile lateral approach for sanders type II and III calcaneal fractures: a meta-analysis of randomized controlled trials. Int J Surg 2018;50:146–153.
-
-
Rammelt S, Amlang M, Barthel S, Zwipp H. Minimally-invasive treatment of calcaneal fractures. Injury 2004;35 Suppl 2:SB55–SB63.
-
-
Carr JB. Surgical treatment of intra-articular calcaneal fractures: a review of small incision approaches. J Orthop Trauma 2005;19:109–117.
-
-
Loucks C, Buckley R. Bohler’s angle: correlation with outcome in displaced intra-articular calcaneal fractures. J Orthop Trauma 1999;13:554–558.
-
-
Csizy M, Buckley R, Tough S, et al. Displaced intra-articular calcaneal fractures: variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106–112.
-
-
van Tetering EA, Buckley RE. Functional outcome (SF-36) of patients with displaced calcaneal fractures compared to SF-36 normative data. Foot Ankle Int 2004;25:733–738.
-
-
Jo SH, Lee JY, Ha SH, Cho SW, Park SH. The result treated by open reduction and internal fixation with minimally invasive technique in joint depressive calcaneal fracture. J Korean Fract Soc 2013;26:126–132.
-
-
Kikuchi C, Charlton TP, Thordarson DB. Limited sinus tarsi approach for intra-articular calcaneus fractures. Foot Ankle Int 2013;34:1689–1694.
-
-
Biggi F, Di Fabio S, D’Antimo C, Isoni F, Salfi C, Trevisani S. Percutaneous calcaneoplasty in displaced intraarticular calcaneal fractures. J Orthop Traumatol 2013;14:307–310.
-
-
Kesemenli CC, Memisoglu K, Atmaca H. A minimally invasive technique for the reduction of calcaneal fractures using the Endobutton®. J Foot Ankle Surg 2013;52:215–220.
-
-
McLaughlin HL. Treatment of late complications after os calcis fractures. Clin Orthop Relat Res 1963;30:111–115.
-
-
Fernandez DL, Koella C. Combined percutaneous and “minimal” internal fixation for displaced articular fractures of the calcaneus. Clin Orthop Relat Res 1993;(290):108–116.
-
-
Tornetta P 3rd. Percutaneous treatment of calcaneal fractures. Clin Orthop Relat Res 2000;(375):91–96.
-
-
Huang PJ, Huang HT, Chen TB, et al. Open reduction and internal fixation of displaced intra-articular fractures of the calcaneus. J Trauma 2002;52:946–950.
-
-
Watson TS. Soft tissue complications following calcaneal fractures. Foot Ankle Clin 2007;12:107–123.
-
-
Lim EV, Leung JP. Complications of intraarticular calcaneal fractures. Clin Orthop Relat Res 2001;(391):7–16.
-
 Cite
Cite
