 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 30(3); 2017 > Article
-
Original Article
- Posterior Dual Plating for Distal Shaft Fractures of the Humerus
-
Chul-Hyun Cho, M.D., Ph.D.
 , Kwang-Yeung Jeong, M.D., Beom-Soo Kim, M.D.
, Kwang-Yeung Jeong, M.D., Beom-Soo Kim, M.D. -
Journal of the Korean Fracture Society 2017;30(3):117-123.
DOI: https://doi.org/10.12671/jkfs.2017.30.3.117
Published online: July 21, 2017
Department of Orthopedic Surgery, Keimyung University School of Medicine, Daegu, Korea.
- Correspondence to: Chul-Hyun Cho, M.D., Ph.D. Department of Orthopedic Surgery, Keimyung University School of Medicine, 56 Dalseong-ro, Jung-gu, Daegu 41931, Korea. Tel: +82-53-250-7729, Fax: +82-53-250-7205, oscho5362@dsmc.or.kr
• Received: November 22, 2016 • Revised: January 22, 2017 • Accepted: June 12, 2017
Copyright © 2017 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,295 Views
- 31 Download
- 1 Crossref
Abstract
-
Purpose
- To evaluate the results and efficacy of posterior dual plating for distal shaft fractures of the humerus.
-
Materials and Methods
- We retrospectively analyzed 12 patients, who underwent open reduction and internal fixation using posterior dual plating for distal shaft fractures of the humerus, between July 2007 and July 2015, with at least 6 months of follow-up. After locating the radial nerve without dissection via posterior triceps splitting, the fracture was stabilized using a short 3.5 mm locking compression plate. Then additional fixation, using a long 3.5 mm locking compression plate, was performed. The clinical outcomes were assessed in accordance with the Mayo Elbow Performance Index (MEPI) scoring system, and the radiological outcomes were assessed using serial plain radiographs.
-
Results
- Eleven patients (91.7%) had bony union, and the mean union period was 13.9 weeks. In one patient, delayed union was treated by autogenous iliac bone graft at 8 months after surgery, which resulted in bony union. The mean MEPI score was 95.8, and the clinical outcomes were excellent in 9 patients and good in 3 patients. Postoperative complications included 1 elbow stiffness by heterotopic ossification and 1 temporary radial nerve palsy. One patient with temporary radial nerve palsy was completely recovered within the first 4 days after surgery.
-
Conclusion
- Posterior dual plating for distal shaft fractures of the humerus revealed satisfactory clinical and radiological outcomes. It can be a useful alternative to provide stable fixation without the need for a dissection of the radial nerve.
- 1. Rhee SK, Lee JY, Suh YJ, Lee JH, Ahn NK. Lateral approach for internal fixation of the distal humeral shaft fractures. J Korean Fract Soc, 2004;17:83-89.Article
- 2. Kwon DG, Moon KH, Na SI, Shin BK, Lee TJ. Combined anterolateral and lateral approaches in treatment of extra-articular fracture of the distal humerus. J Korean Fract Soc, 2012;25:185-190.Article
- 3. Parmaksızoğlu AS, Özkaya U, Bilgili F, Mutlu H, Çetin Ü. Fixation of extra-articular distal humeral fractures with a lateral approach and a locked plate: an alternative method. Acta Orthop Traumatol Turc, 2016;50:132-138.
- 4. Prasarn ML, Ahn J, Paul O, et al. Dual plating for fractures of the distal third of the humeral shaft. J Orthop Trauma, 2011;25:57-63.Article
- 5. Rubel IF, Kloen P, Campbell D, et al. Open reduction and internal fixation of humeral nonunions: a biomechanical and clinical study. J Bone Joint Surg Am, 2002;84-A:1315-1322.
- 6. Tejwani NC, Murthy A, Park J, McLaurin TM, Egol KA, Kummer FJ. Fixation of extra-articular distal humerus fractures using one locking plate versus two reconstruction plates: a laboratory study. J Trauma, 2009;66:795-799.Article
- 7. Watts A, Weinhold P, Kesler W, Dahners L. A biomechanical comparison of short segment long bone fracture fixation techniques: single large fragment plate versus 2 small fragment plates. J Orthop Trauma, 2012;26:528-532.
- 8. Browner BD, Jupiter JB, Levine AM, et al. Skeletal trauma. 3rd ed. Philadelphia: Saunders; 2003. p. 1436-1511.
- 9. Jawa A, McCarty P, Doornberg J, Harris M, Ring D. Extraarticular distal-third diaphyseal fractures of the humerus. A comparison of functional bracing and plate fixation. J Bone Joint Surg Am, 2006;88:2343-2347.
- 10. Schatzker J. Fractures of the humerus. In: Schatzker J, editor. The rationale of operative fracture care. New York: Springer Verlag; 1987. p. 61-70.
- 11. Aitken GK, Rorabeck CH. Distal humeral fractures in the adult. Clin Orthop Relat Res, 1986;(207):191-197.Article
- 12. Scolaro JA, Voleti P, Makani A, Namdari S, Mirza A, Mehta S. Surgical fixation of extra-articular distal humerus fractures with a posterolateral plate through a triceps-reflecting technique. J Shoulder Elbow Surg, 2014;23:251-257.Article
- 13. Archdeacon MT, Wyrick JD. Reduction plating for provisional fracture fixation. J Orthop Trauma, 2006;20:206-211.Article
REFERENCES

Fig. 2
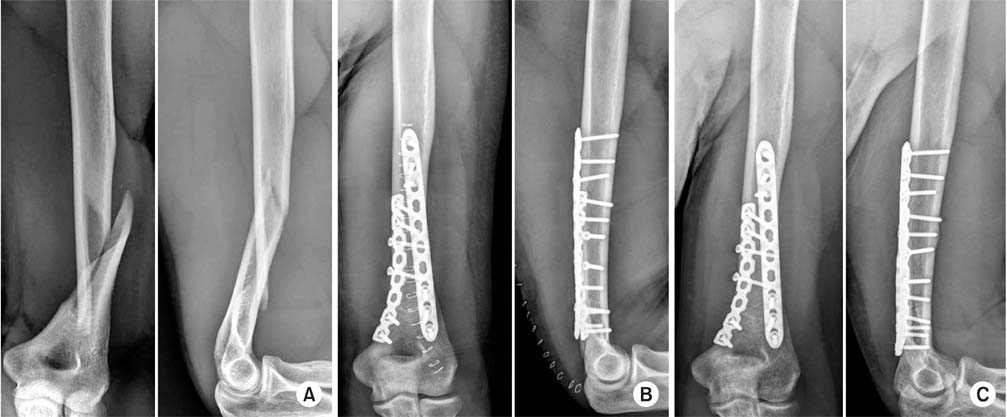
(A) Radiographs at the time of initial trauma show spiral distal shaft fracture of the left humerus. (B) Postoperative radiographs show anatomical reduction and stable fixation using posterior dual plating. (C) Radiographs at 10 weeks after surgery show bony union.
Fig. 3
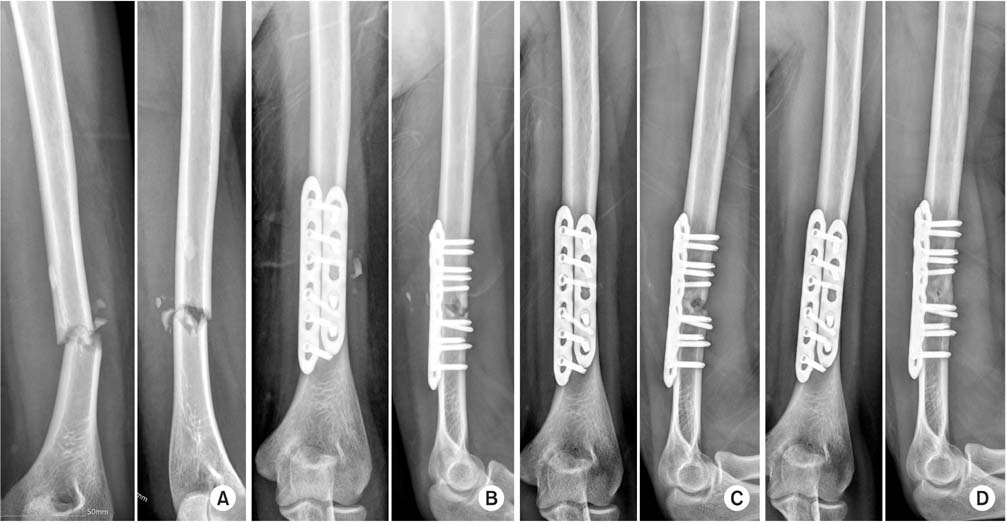
(A) Radiographs at the time of initial trauma show transverse distal shaft fracture of the left humerus. (B) Postoperative radiographs show posterior dual plating. (C) Radiographs at 8 months after the surgery show delayed union. (D) Radiographs at the final follow-up show bony union.
Table 1
![jkfs-30-117-i001.jpg]()
Demographic and Clinical Data
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Quantitative Analysis of the Radial Nerve Pathway Relative to the Humerus Shaft Length: A Cadaveric Study Aimed at Minimizing Nerve Injury in Fracture Treatment
Chang-Jin Yon, Beom-Soo Kim, Eun-Seok Son, Chul-Hyun Cho
Clinics in Orthopedic Surgery.2026; 18(3): 405. CrossRef
 Cite
CitePosterior Dual Plating for Distal Shaft Fractures of the Humerus

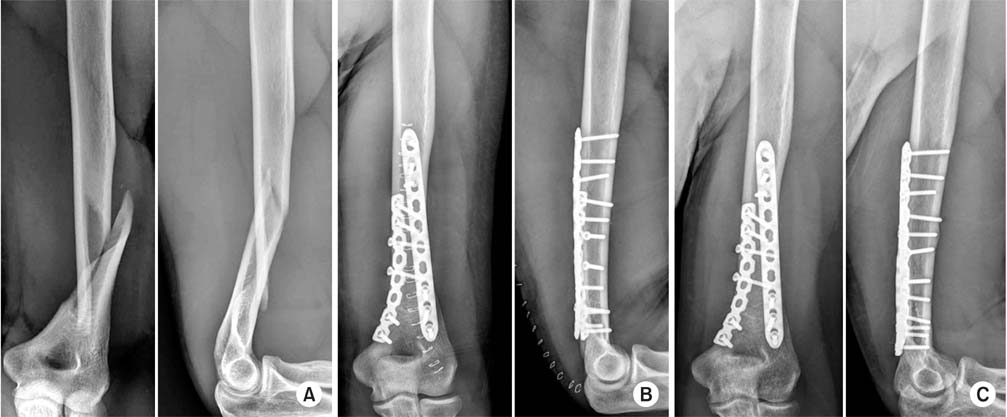
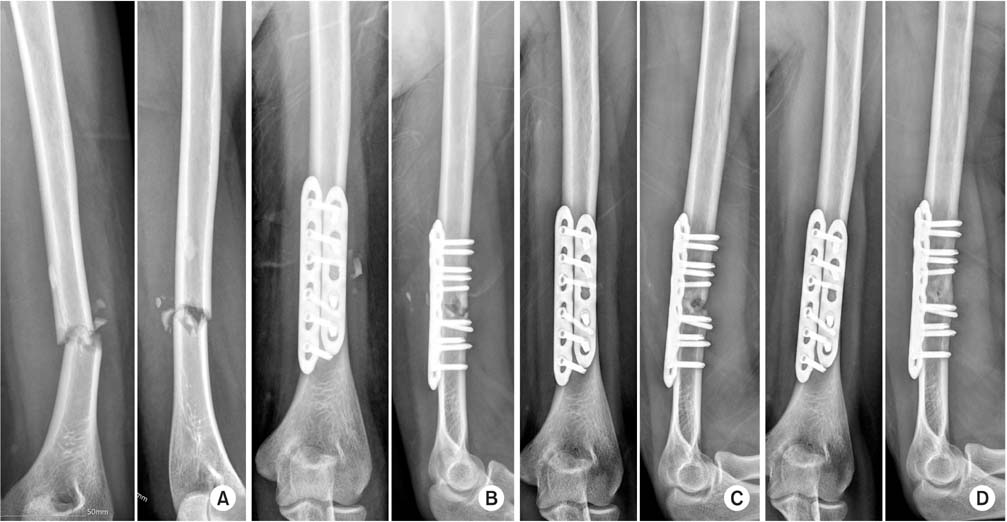
Fig. 1
Preoperative drawing on an anteroposterior plain radiograph.
Fig. 2
(A) Radiographs at the time of initial trauma show spiral distal shaft fracture of the left humerus. (B) Postoperative radiographs show anatomical reduction and stable fixation using posterior dual plating. (C) Radiographs at 10 weeks after surgery show bony union.
Fig. 3
(A) Radiographs at the time of initial trauma show transverse distal shaft fracture of the left humerus. (B) Postoperative radiographs show posterior dual plating. (C) Radiographs at 8 months after the surgery show delayed union. (D) Radiographs at the final follow-up show bony union.
Fig. 1
Fig. 2
Fig. 3
Posterior Dual Plating for Distal Shaft Fractures of the Humerus
Demographic and Clinical Data
| Case No. | Age (yr) | Sex | Injury mechanism | OTA classification | Union (wk) | Followup (mo) | Elbow ROM (°) | MEPI score | Clinical outcome | Complication |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 26 | M | TA | 12-A3 | 9 | 89 | 5-140 | 100 | Excellent | - |
| 2 | 21 | F | TA | 12-A3 | 48 | 87 | 0-140 | 100 | Excellent | Delayed union |
| 3 | 40 | F | TA | 12-B1 | 14 | 69 | 10-140 | 85 | Good | - |
| 4 | 20 | M | Arm wrestling | 12-C1 | 7 | 18 | 0-140 | 100 | Excellent | - |
| 5 | 24 | M | Traction | 12-A1 | 12 | 16 | 0-140 | 100 | Excellent | - |
| 6 | 25 | M | Arm wrestling | 12-A1 | 10 | 16 | 0-140 | 100 | Excellent | - |
| 7 | 26 | M | Pitching | 12-A1 | 12 | 15 | 0-140 | 85 | Good | Temporary radial nerve palsy |
| 8 | 81 | F | TA | 12-A1 | 16 | 12 | 10-130 | 100 | Excellent | - |
| 9 | 23 | F | Slip down | 12-C1 | 16 | 51 | 0-130 | 100 | Excellent | - |
| 10 | 75 | F | TA | 12-A2 | 21 | 84 | 40-110 | 80 | Good | Elbow stiffness |
| 11 | 63 | F | Slip down | 12-B1 | 16 | 7 | 0-140 | 100 | Excellent | - |
| 12 | 29 | M | Slip down | 12-A3 | 20 | 20 | 0-140 | 100 | Excellent | - |
OTA: Orthopaedic Trauma Association, ROM: range of motion, MEPI: Mayo Elbow Performance Index, M: male, F: female, TA: traffic accident.
Table 1
Demographic and Clinical Data
OTA: Orthopaedic Trauma Association, ROM: range of motion, MEPI: Mayo Elbow Performance Index, M: male, F: female, TA: traffic accident.

