 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 35(2); 2022 > Article
- Original Article Posterior Anti-Glide Plating for Supination External Rotation Type Lateral Malleolar Fractures: Clinical Comparison of Locking versus Non-Locking One-Third Semi-Tubular Plate Fixation
- Jun Young Lee, Yong Jin Cho, Dong Hyuk Cha, Hyun Bai Choi, Jung Ho Lee
-
Journal of Musculoskeletal Trauma 2022;35(2):57-62.
DOI: https://doi.org/10.12671/jkfs.2022.35.2.57
Published online: April 30, 2022
Department of Orthopaedic Surgery, Chosun University School of Medicine, Gwangju, Korea
- 714 Views
- 4 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
The purpose of this study was to evaluate and compare the clinical and radiological outcomes between locking plates and non-locking plates using posterior anti-glide plating for supination external rotation type lateral malleolar fractures.
Materials and Methods
A total of 50 patients who underwent internal fixation of posterior anti-glide plating due to lateral malleolar fractures, classified as supination-external rotation (SER) as per the Lauge-Hansen classification system, at our hospital from January 2017 to November 2018 were retro-spectively evaluated. Patients were divided into two groups: 1/3 semi-tubular locking plate (24 patients) and 1/3 semi-tubular non-locking plate (26 patients). A radiographic assessment was performed after surgery to evaluate the time of bone union. The American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot functional score was measured after the surgery to evaluate the clinical outcomes.
Results
The two groups showed similar distributions in sex, age, height, body mass index, fracture pattern, and mean follow-up period. Complete bone union was obtained in all cases and the mean bone union time was 13.00±3.38 weeks in Group 1 and 12.92±3.26 weeks in Group 2 (p=0.87). The mean AOFAS score at 24 weeks was 95.66±2.86 in Group 1 and 95.84±2.79 in Group 2 (p=0.82). The mean AOFAS score at 48 weeks was 97.25±3.54 in Group 1 and 96.57±3.07 in Group 2 (p=0.47). Two cases of complications were observed in the non-locking plate group.
Conclusion
For the treatment of Lauge-Hansen SER type lateral malleolar fracture, internal fixation us-ing locking 1/3 semi-tubular plate and non-locking 1/3 semi-tubular plate are both favorable fixation methods.
J Korean Fract Soc. 2022 Apr;35(2):57-62. Korean.
Published online Apr 25, 2022.
https://doi.org/10.12671/jkfs.2022.35.2.57
Published online Apr 25, 2022.
https://doi.org/10.12671/jkfs.2022.35.2.57
Copyright © 2022 The Korean Fracture Society.
Original Article
Lauge-Hansen 분류 회외-외회전 외복사 골절에서 후방 항활주 고정 시 잠김 금속판 및 비잠김 금속판을 이용한 내고정의 임상적 비교
Posterior Anti-Glide Plating for Supination External Rotation Type Lateral Malleolar Fractures: Clinical Comparison of Locking versus Non-Locking One-Third Semi-Tubular Plate Fixation
Jun Young Lee , M.D., Ph.D.,
Yong Jin Cho, M.D., Ph.D.,
Dong Hyuk Cha, M.D.,
Hyun Bai Choi, M.D.
and Jung Ho Lee, M.D.
, M.D., Ph.D.,
Yong Jin Cho, M.D., Ph.D.,
Dong Hyuk Cha, M.D.,
Hyun Bai Choi, M.D.
and Jung Ho Lee, M.D.
, M.D., Ph.D.,
Yong Jin Cho, M.D., Ph.D.,
Dong Hyuk Cha, M.D.,
Hyun Bai Choi, M.D.
and Jung Ho Lee, M.D.
초록
목적
Lauge-Hansen 분류 회외-외회전 외복사 골절에서 후방 항활주 고정 시 잠김, 비잠김 금속판을 이용한 내고정에 따른 임상적 및 방사선학적 결과를 비교하고자 한다.
대상 및 방법
2017년 1월부터 2018년 11월까지 Lauge-Hansen 분류 회외-외회전 외복사 골절에서 1/3 원통 잠김 금속판을 이용한 경우(24예, 1군)와 1/3 원통 비잠김 금속판을 이용한 경우(26예, 2군)로 분류하였다. 방사선학적 골유합 시기를 확인하였고, 임상적 평가로 AOFAS score를 시행하고 합병증 여부를 확인하였다.
결과
두 군은 성별, 나이, 신장, 체질량지수, 골절 양상, 평균 추시 기간에서 유의한 차이를 보이지 않았다. 평균 골유합 기간은 1군과 2군에서 유의한 차이가 없었다. AOFAS score는 술 후 24주, 48주에서 유의한 차이가 없었으나 2군에서 2예의 합병증이 관찰되었다.
결론
Lauge-Hansen 분류 회외-외회전 외복사 골절에서 1/3 원통 잠김, 비잠김 금속판을 이용한 후방 항활주 고정 술식은 모두 적절한 선택이 될 수 있을 것으로 생각된다.
Abstract
Purpose
The purpose of this study was to evaluate and compare the clinical and radiological outcomes between locking plates and non-locking plates using posterior anti-glide plating for supination external rotation type lateral malleolar fractures.
Materials and Methods
A total of 50 patients who underwent internal fixation of posterior anti-glide plating due to lateral malleolar fractures, classified as supination-external rotation (SER) as per the Lauge-Hansen classification system, at our hospital from January 2017 to November 2018 were retrospectively evaluated. Patients were divided into two groups: 1/3 semi-tubular locking plate (24 patients) and 1/3 semi-tubular non-locking plate (26 patients). A radiographic assessment was performed after surgery to evaluate the time of bone union. The American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot functional score was measured after the surgery to evaluate the clinical outcomes.
Results
The two groups showed similar distributions in sex, age, height, body mass index, fracture pattern, and mean follow-up period. Complete bone union was obtained in all cases and the mean bone union time was 13.00±3.38 weeks in Group 1 and 12.92±3.26 weeks in Group 2 (p=0.87). The mean AOFAS score at 24 weeks was 95.66±2.86 in Group 1 and 95.84±2.79 ni Group 2 (p=0.82). The mean AOFAS score at 48 weeks was 97.25±3.54 in Group 1 and 96.57±3.07 ni Group 2 (p=0.47). Two cases of complications were observed in the non-locking plate group.
Conclusion
For the treatment of Lauge-Hansen SER type lateral malleolar fracture, internal fixation using locking 1/3 semi-tubular plate and non-locking 1/3 semi-tubular plate are both favorable fixation methods.
Keywords
Lateral malleolar fractures, Locking plate, Posterior anti-glide plating
외복사 골절, 잠김 금속판, 후방 항활주 금속판 고정
서론
족관절 외복사 골절은 정형외과 영역에서 볼 수 있는 흔한 골절 양상으로 전체 골절의 9%를 차지한다고 알려져 있다.1) 불안정한 형태의 외복사 골절은 전위된 골편을 정복하고 해부학적 길이 및 회전 변형 회복을 위해 관혈적 정복과 내고정술이 필요하며2,3) 적절한 정복과 안정적인 고정은 족관절의 조기 운동과 외상 후 관절염을 줄이기 위해 중요하다.4) Lauge-Hansen 분류상5) 회외-외회전 외복사 골절은 특징적으로 골절선이 후상방에서 전하방으로 발생하는데, 수술 방법으로는 대표적으로 외측 금속판을 이용한 내고정과 후방 항활주 금속판6)을 이용한 내고정 방법이 있다. 외측 금속판을 이용한 고정은 삽입물의 돌출로 피부 자극, 동통, 비골건 손상 그리고 나사의 관절 내 관통과 같은 단점이 보고되고 있으며,7,8) 후방 항활주 금속판을 이용한 고정은 비골건염과 같은 합병증9)이 보고되고 있지만 외측 금속판을 이용한 고정보다 생역학적으로 우수한 안정성을 제공한다고 알려져 있다.10) 금속판은 비잠김 금속판 또는 잠김 금속판을 선택해 볼 수 있는데 기존의 비잠김 금속판과 달리 잠김 금속판에서는 fixed angle system을 제공하기 때문에 각과 축 안정성이 높고 골밀도에 덜 영향을 받으며 골절을 안정화시킬 수 있으며, 금속판과 골 사이의 마찰과 압박력을 줄여 삽입물의 안정성을 유지하는 데 유리하다.11) Lauge-Hansen 분류 회외-외회전 외복사 골절에서 후방 항활주 고정 시 잠김 금속판과 비잠김 금속판을 이용한 내고정에 관한 비교에 대한 연구는 거의 없다. 따라서 본 연구에서는 내고정 후 임상적 및 방사선학적 결과에 대해 비교하고자 하였다.
대상 및 방법
2017년 1월부터 2018년 11월까지 조선대학교병원에서 Lauge-Hansen 분류 회외-외회전 외복사 골절 진단하에 1/3 원통 금속판을 이용하여 후방 항활주 금속판 고정술을 시행한 환자 65예를 대상으로 연구를 진행하였다. 포함 기준은 20세 이상의 성인, 외복사 골절, 수술일로부터 최소 48주 이상의 추시가 가능하였던 환자를 대상으로 하였다. 제외 기준은 동측 하지의 동반 손상이 있거나(8예) 금속 삽입물 주변 골절이 있는 경우(3예), 수상 부위의 이전 골절 과거력이 있는 경우(3예), 골절 부위 불유합으로 재수술한 경우(1예)를 제외하고 남은 50예에 대해서 후향적으로 분석하였다. 본 연구는 조선대학교병원 연구윤리위원회(Institutional Review Board, IRB)의 승인하에 진행되었으며(IRB No. 2021-01-005-002), 후향적 의무기록 연구로 환자 서면동의는 IRB에 의해 면제 받았다.
1/3 원통 잠김 금속판을 이용하여 후방 항활주 금속판 고정술을 시행한 경우(1군)와 1/3 원통 비잠김 금속판을 이용하여 후방 항활주 금속판 고정술을 시행한 경우(2군)로 나누어 조사하였고 잠김 금속판 또는 비잠김 금속판 사용은 무작위로 선택되었으며 각각 24예, 26예였다. 모든 수술은 한 명의 술자(J.Y.L.)에 의해 시행되었으며 수술은 전 예에서 1주 이내 시행하였고, 반 측와위(semi-lateral position)에서 비골 원위부 후외연을 따라 골절부를 종 절개한 후 비골건막의 손상과 비골건의 손상에 주의하며 원위 비골 후면을 따라 골절부를 노출시켰다. 골절 정복 후 비골 원위부 후면의 모양에 따라 1/3 원통 금속판을 굴곡시켜 사용하였고 금속판을 통하여 지연나사 고정을 시행하였다(Fig. 1). 금속판은 Synthes 사의 1/3 원통 잠김 금속판(Synthes, West Chester, PA, USA)과 1/3 원통 비잠김 금속판(Synthes, Oberdorf, Switzerland)을 이용하였고 두 금속판의 모양과 용적은 거의 같았으나 비잠김 금속판의 경우 나사 구멍에 나사산이 있었다(Fig. 2). 수술 후 4주간 단하지 석고고정을 하였고 4주째부터 능동 및 수동적 관절 운동을 시작하였으며 보조기를 착용한 채 목발을 이용한 부분 체중부하를 허용하였다.

Fig. 1
Posterior anti-glide plating with pre-contoured 1/3 semi-tubular locking plate.
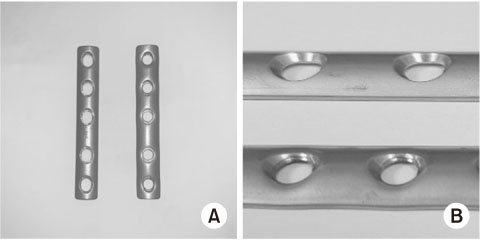
Fig. 2
1/3 semi-tubular non-locking plate (Synthes, Switzerland) (A, left; B, upper), 1/3 semi-tubular locking plate (Synthes, USA) (A, right; B, lower).
본 연구의 방사선학적 평가로는 두 군에서 수술 직후, 1, 6, 12, 24, 48주 후 추시하여 방사선 사진을 확인 및 검토하여 골유합 시기를 확인하였고 골유합 여부를 평가하기 위해 발목 전후면, 격자면, 측면 사진을 촬영하였고, 3-4면의 피질골이 맞닿아 있고 골절선이 사라졌을 때 골이 유합된 것으로 판단하였다.12) 임상적 평가로는 수술 후 24주, 48주 후의 American Orthopaedic Foot and Ankle Society (AOFAS) 족관절-후족부 기능 평가 지수(ankle-hindfoot functional score)의 변화를 두 군 간 비교 분석하였으며, 심부 및 천부 감염, 고정 실패, 불유합, 비골건 자극 증상 등의 합병증에 대해 분석하였다.
통계 분석은 IBM SPSS Statistics 프로그램(ver. 25.0; IBM, Armonk, NY, USA)을 이용했고 각 군의 명목변수 간 상관관계 검정을 위해 카이제곱 검정, 각 군의 연속변수 검정을 위해 독립표본 검정을 이용하였다. 통계적 유의 수준은 p 값이 0.05 미만인 경우로 하였다. 두 군과 하위 집단의 결과 비교 및 분석을 위해 G*Power 프로그램13)을 이용하였으며 효과 크기는 0.5, 알파값은 0.05로 하였다.
결과
각 군 간의 적절한 비교를 위하여 각 군 간 특성을 비교하였고, 1군 및 2군의 평균 연령은 46.41±20.31세 및 43.92±20.08세였다(p=0.92). 1군과 2군에서 성비(남:여)는 각각 13:11과 12:14였으며(p=0.78), 수술 부위(우측:좌측)는 각각 12:12와 14:12였다(p=0.57). 평균 신장은 각각 163.08±6.15 cm 및 169.69±8.36 cm였고(p=0.06), 체질량지수(body mass index)는 각각 24.23±2.27 kg/m2 및 24.25±2.46 kg/m2였으며(p=0.43), 평균 체중은 64.5±7.31 kg 및 70.19±11.05 kg (p=0.01)으로 통계적으로 유의미한 차이를 보였다. 또한 골절 양상은 Lauge-Hansen supination external rotation (SER) type II, type III, type IV 골절 각각 9:9:6 (37.5%:37.5%:25%), 12:9:5 (46.1%:34.6%:19.2%)로 보였으며(p=0.80), 경비인대결합을 고정한 경우는 각각 2예(8.3%)와 2예(7.7%)였다(p=0.93) (Table 1) (G*Power=0.4).
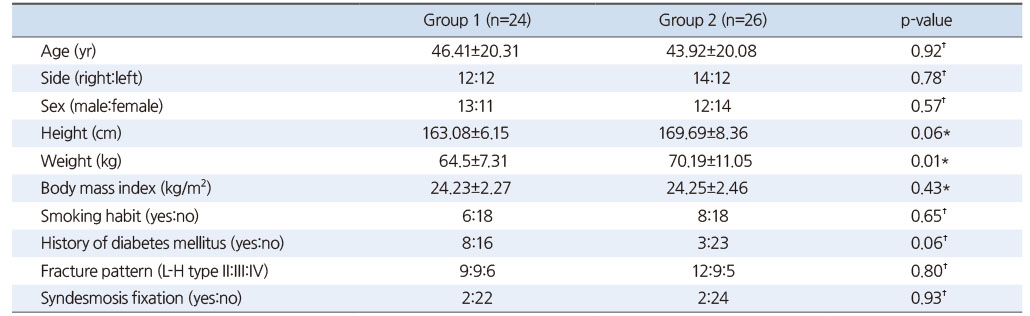
Table 1
Patient’s Demographics and Characteristics
방사선학적 결과를 보았을 때 전 예에서 골유합을 얻을 수 있었고(Fig. 3), 1군과 2군에서 평균 골유합까지 기간은 각각 13.00±3.38주, 12.92±3.26주로 유의한 차이가 없었다(p=0.87). 임상적 결과를 보았을 때 AOFAS 족관절-후족부 기능 평가 지수는 술 후 24주에 1군과 2군에서 각각 95.66±2.86점, 95.84±2.79점이었으며(p=0.82), 48주에 각각 97.25±3.54점, 96.57±3.07점으로 유의한 차이가 없었다(p=0.47). 술 후 합병증은 잠김 금속판군에서는 관찰되지 않았고 비잠김 금속판군에서 비골건 자극 증상 1예와 창상 천부 감염 소견 1예로 총 2예가 관찰되었다. 2예 모두에서 수술적 처치는 시행하지 않았고 약물 치료 및 항생제 치료로 호전 소견을 보였다(Table 2) (G*Power=0.4).

Fig. 3
Preoperative and postoperative anterior-posterior radiograph following open reduction and internal fixation with a 1/3 semi-tubular locking plate (A) and 1/3 semi-tubular non-locking plate (B).

Table 2
Radiographic Union, Functional Results and Complications
고찰
비골 원위부 골절에서 Lauge-Hansen 분류법에 따른 회외-외회전 외복사 골절은 가장 흔한 유형의 골절이고 주로 수술적 처치를 시행하는데, 해부학적 정복 후 골유합 시까지 안정된 고정을 시켜 조기에 관절 운동을 통해 수상 전 상태의 관절로 회복시키는 것과14) 외측 구조물의 지지대 역할을 하는 삽입물로 고정을 함으로써 골절로 인해 발생할 수 있는 외측 구조물의 단축을 일으키지 않는 것이 중요하다.9,15)
Brunner와 Weber6)는 외복사 골절에서 후방 항활주 방법을 이용한 고정을 소개하였으며 Schaffer와 Manoli16)는 항활주 고정 방법과 외측 금속판과의 생역학적인 비교 연구에서 중등도 이하 강도의 골질에서 특히 항활주 고정술이 유의하게 우수하다고 보고하였고, Minihane 등10)은 특히 골다공증성 골질에서 후방 항활주 고정술이 생역학적으로 유의하게 우수하다고 보고한 바 있다. 또한 Kilian 등17)은 원위 비골 Dannis-Weber type B형의 골절에서 외측 금속판을 이용한 고정과 후방 항활주 금속판을 이용한 고정을 후향적으로 비교하였는데, 후방 항활주 금속판 사용군(15%)이 외측 금속판 사용군(29.3%)보다 합병증이 더 적었으며 구체적으로는 창상 관련 합병증, 삽입물로 인한 자극 증상, 심부 정맥 혈전증이 있었으나 두 군 간 통계적 유의함은 없다고 보고하였다(p=0.31). 이에 본 연구에서는 후방 항활주 고정술을 이용하여 회외-외회전 외복사 골절을 안정화하였으며, 모든 예(50예)에서 골유합을 얻을 수 있었고 1예에서 비골건 자극 증상, 1예에서 천부 창상 감염을 관찰할 수 있었다.
몇몇 연구들에서는 비골 원위부 골절에서 잠김 금속판을 이용한 고정과 비잠김 금속판을 이용한 고정을 비교하였는데, White 등18)은 분쇄가 심하고 불안정한 비골 원위부 골절에 대한 사체 연구에서 잠김 금속판과 일반적인 가교 금속판 고정 간의 생역학적으로 유의미한 차이는 없었다고 보고하였다. Tsukada 등19)은 외복사 골절 환자에서 시행한 잠김 금속판 고정군과 비잠김 금속판 고정군 간의 무작위 대조 연구를 시행하였고 골유합과 임상적 점수, 합병증 발생 측면에서 유의미한 차이는 없다고 보고하였다. 하지만 이 연구들은 외측 금속판을 이용한 술식이었고 후방 항활주 고정 방법을 이용한 비교 연구는 거의 보고된 바가 없다. 본 연구에서는 Lauge-Hansen 분류 회외-외회전 외복사 골절에서 후방 항활주 고정 방법을 이용한 술식에서 잠김 금속판 및 비잠김 금속판 사용에 대한 임상적 결과를 비교하였고 두 군 간 방사선학적, 임상적, 합병증 발생 여부 측면에서 유의한 차이를 보이지 않았다.
본 연구는 후향적으로 진행된 연구이며 비교적 적은 사례로 인한 통계적 제한점이 있다. 실제 G*Power를 측정하였을 때 적은 표본으로 인해 그 값이 0.4 이하로 저조하였다. 또한 표본의 편중이 있을 수 있고 한 명의 술자에 의해 수술이 시행되었다는 제한점이 있다. 본 연구에서는 모든 예에서 지연 나사 고정을 시행하였는데, 잠김 및 비잠김 금속판 사이의 순수한 후방 항활주 금속판의 차이 비교에 대한 추가적인 연구가 필요할 것으로 생각된다. 구체적으로는 지연나사 고정 방법을 사용하지 않은 두 군에서의 골유합 정도 비교나 추시 기간 중 지연나사 못의 해리 여부 등에 대한 추가적인 비교 연구가 필요할 것이다. 다만 본 연구는 이전의 연구들과 달리 회외-외회전 외복사 골절에서 후방 항활주 금속판 고정 중 1/3 원통 잠김 금속판과 비잠김 금속판을 이용한 방법에 대한 임상적 결과에 대해 비교하였다는 것에 의의가 있으며, 최근 고령의 당뇨, 골다공증 등 다양한 기저력을 가진 환자에서의 외복사 골절의 유병률이 증가함에 따라 다양한 수술적 방법에 따른 전향적 또는 무작위 대조 연구 등 추가적인 연구가 필요할 것으로 생각된다.
결론
Lauge-Hansen 분류 회외-외회전 외복사 골절의 수술적 처치 시 후방 항활주 1/3 반원형 잠김 금속판과 비잠김 금속판을 이용한 고정술의 방사선학적 결과에서 골유합 시기, 합병증의 발생 여부에 차이가 없었으며 임상적 기능 평가 항목에서 족관절-후족부 기능 평가 지수 또한 유의미한 차이를 보이지 않았다. 따라서 원통 잠김 금속판과 비잠김 금속판을 이용한 후방 항활주 고정 술식은 모두 적절한 선택이 될 수 있을 것으로 생각된다.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury 2006;37:691–697.
-
-
Ali MS, McLaren CA, Rouholamin E, O’Connor BT. Ankle fractures in the elderly: nonoperative or operative treatment. J Orthop Trauma 1987;1:275–280.
-
-
Hughes JL, Weber H, Willenegger H, Kuner EH. Evaluation of ankle fractures: non-operative and operative treatment. Clin Orthop Relat Res 1979;(138):111–119.
-
-
Michelson JD. Fractures about the ankle. J Bone Joint Surg Am 1995;77:142–152.
-
-
Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg 1950;60:957–985.
-
-
Brunner CF, Weber BG. In: Special techniques in internal fixation. Berlin: Springer Science & Business Media; 2013.
-
-
Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma 2001;15:271–274.
-
-
Redfern DJ, Sauvé PS, Sakellariou A. Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771–774.
-
-
Weber M, Krause F. Peroneal tendon lesions caused by antiglide plates used for fixation of lateral malleolar fractures: the effect of plate and screw position. Foot Ankle Int 2005;26:281–285.
-
-
Minihane KP, Lee C, Ahn C, Zhang LQ, Merk BR. Comparison of lateral locking plate and antiglide plate for fixation of distal fibular fractures in osteoporotic bone: a biomechanical study. J Orthop Trauma 2006;20:562–566.
-
-
Miranda MA. Locking plate technology and its role in osteoporotic fractures. Injury 2007;38 Suppl 3:S35–S39.
-
-
Corrales LA, Morshed S, Bhandari M, Miclau T 3rd. Variability in the assessment of fracture-healing in orthopaedic trauma studies. J Bone Joint Surg Am 2008;90:1862–1868.
-
-
Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods 2009;41:1149–1160.
-
-
Segal D, Wiss DA, Whitelaw GP. Functional bracing and rehabilitation of ankle fractures. Clin Orthop Relat Res 1985;(199):39–45.
-
-
Belcher GL, Radomisli TE, Abate JA, Stabile LA, Trafton PG. Functional outcome analysis of operatively treated malleolar fractures. J Orthop Trauma 1997;11:106–109.
-
-
Schaffer JJ, Manoli A 2nd. The antiglide plate for distal fibular fixation. A biomechanical comparison with fixation with a lateral plate. J Bone Joint Surg Am 1987;69:596–604.
-
-
Kilian M, Csörgö P, Vajczikova S, Luha J, Zamborsky R. Antiglide versus lateral plate fixation for Danis-Weber type B malleolar fractures caused by supination-external rotation injury. J Clin Orthop Trauma 2017;8:327–331.
-
-
White NJ, Corr DT, Wagg JP, Lorincz C, Buckley RE. Locked plate fixation of the comminuted distal fibula: a biomechanical study. Can J Surg 2013;56:35–40.
-
-
Tsukada S, Otsuji M, Shiozaki A, et al. Locking versus non-locking neutralization plates for treatment of lateral malleolar fractures: a randomized controlled trial. Int Orthop 2013;37:2451–2456.
-
 Cite
Cite
