 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 21(1); 2008 > Article
-
Original Article
- The Factors that Affect the Deformity Correction of Vertebral Body during Kyphoplasty of Osteoporotic Vertebral Compression Fracture
- Young-Do Koh, M.D., Jong-Seok Yoon, M.D., Sung-Il Kim, M.D.
-
Journal of the Korean Fracture Society 2008;21(1):57-61.
DOI: https://doi.org/10.12671/jkfs.2008.21.1.57
Published online: January 31, 2008
Department of Orthopedic Surgery, Ewha Womans University School of Medicine, Seoul, Korea.
- Address reprint requests to: Young-Do Koh, M.D. Department of Orthopedic Surgery, Mokdong Hospital, Ewha Womans University, School of Medicine, 911-1, Mok 6-dong, Yangcheon-gu, Seoul 158-710, Korea. Tel: 82-2-2650-5564, Fax: 82-2-2642-0349, ydkoh@ewha.ac.kr
Copyright © 2008 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 837 Views
- 1 Download
Abstract
-
Purpose
- To study which factors affect the deformity correction of vertebral body during kyphoplasty procedure.
-
Materials and Methods
- 25 osteoporotic vertebral compression fractures were treated with balloon kyphoplasty from October 2006 to May 2007. Lateral radiographs were taken at 5 different stages with preoperative lateral decubitus position, after placing the patient in prone position on an operation table, after inflating balloon, after deflation and removal of the balloon, after inserting the cement. Then we analyzed the compression ratios and kyphotic angles of the vertebral bodies in each stage.
-
Results
- Placing the patient in prone position showed significant postural reduction in kyphotic angle and restorement of the anterior and middle body height. The inflation of the balloon demonstrated significant reduction of kyphotic angle and restorement of the anterior and middle body height. After the deflation, anterior and middle body height has decreased significantly. After the deflation, the kyphotic angle and the anterior and middle body heights were not restored signigicantly compared with those of initial prone position.
-
Conclusion
- Vertebral height and kyphotic angle were partially recovered by inflating the balloon, but the correction was lost after deflating the balloon. Statistically, the body deformity was not restored significantly after deflating the balloon compared with that of intraoperative prone position. Therefore, we concluded that, in kyphoplasty of osteoporotic compression fractures, the postural reduction is the most important factor in deformity correction of fractured vertebral bodies.
- 1. Belkoff SM, Mathis JM, Fenton DC, Scribner RM, Reiley ME, Talmadge K. An ex vivo biomechanical evaluation of an inflatable bone tamp used in the treatment of compression fracture. Spine, 2001;26:151-156.Article
- 2. Cook DJ, Guyatt GH, Adachi JD. Quality of life issues in women with vertebral fractures due to osteoporosis. Arthritis Rheum, 1993;36:750-756.Article
- 3. Faciszewski T, McKiernan F. Calling all vertebral fractures classification of vertebral compression fractures: a consensus for comparison of treatment and outcome. J Bone Miner Res, 2002;17:185-191.ArticlePDF
- 4. Gaitanis IN, Carandang G, Phillips FM, et al. Restoring geometric and loading alignment of the thoracic spine with a vertebral compression fracture: effects of balloon (bone tamp) inflation and spinal extension. Spine J, 2005;5:45-54.Article
- 5. Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR. Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med, 1999;159:1215-1220.Article
- 6. Kayanja MM, Ferrara LA, Lieberman IH. Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J, 2004;4:76-87.Article
- 7. Kim MH, Min SH, Jeon SH. Risk factors of new compression fractures in adjacent vertebrae after percutaneous vertebroplasty. J Korean Fract Soc, 2007;20:260-265.Article
- 8. Kim YS, Chin DK, Cho YE, Jin BH, Kuh SU. Percutaneous vertebroplasty: new technique using a postural reduction for acute osteoporotic vertebral compression fracture. World Spine II Meeting; 2003.08; p. 10-13.
- 9. Kim YW, Chang HG, Lee KB, Ji YN, Lee YB, Ku JM. Vertebroplasty for the treatment of painful osteoporotic compression fractures. J Korean Fract Soc, 2004;17:49-54.Article
- 10. Kuklo TR, Polly DW, Owens BD, et al. Measurement of thoracic and lumbar fracture kyphosis: evaluation of intraobserver, interobserver, and technique variability. Spine, 2001;26:61-65.Article
- 11. Leidig-Bruckner G, Minne HW, Schlaich C. Clinical grading of spinal osteoporosis: quality of life components and spinal deformity in women with chronic low back pain and women with vertebral osteoporosis. J Bone Miner Res, 1997;12:663-675.ArticlePDF
- 12. Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of kyphoplasty in the treatment of painful osteoporotic vertebral compression fractures. Spine, 2001;26:1631-1638.Article
- 13. Lieberman I, Reinhardt MK. Vertebroplasty and kyphoplasty for osteolytic vertebral collapse. Clin Orthop Relat Res, 2003;415 Suppl. S176-S186.Article
- 14. Lindsay R, Silverman SL, Cooper C, et al. Risk of new vertebral fracture in the year following a fracture. JAMA, 2001;285:320-323.Article
- 15. Lyles KW, Gold DT, Shipp KM, Pieper CF, Martinez S, Mulhausen PL. Association of osteoporotic vertebral compression fractures with impaired functional status. Am J Med, 1993;94:595-601.Article
- 16. McKiernan F, Jensen R, Faciszewski T. The dynamic mobility of vertebral compression fractures. J Bone Miner Res, 2003;18:24-29.ArticlePDF
- 17. Myers ER, Wilson S. Biomechanics of osteoporosis and vertebral fracture. Spine (Phila Pa 1976), 1997;22:25S-31S.Article
- 18. Nevitt MC, Ross PD, Palermo L, Musliner T, Genant HK, Thompson DE. Association of prevalent vertebral fractures, bone density, and alendronate treatment with incident vertebral fractures: effect of number and spinal location of fractures. The Fracture Intervention Trial Research Group. Bone, 1999;25:613-619.Article
- 19. Oleksik A, Lips P, Dawson A, et al. Health-related quality of life in post-menopausal women with low BMD with or without prevalent vertebral fractures. J Bone Miner Res, 2000;15:1384-1392.ArticlePDF
- 20. Phillips FM, Todd Wetzel F, Lieberman I, Campbell-Hupp M. An in vivo comparison of the potential for extravertebral cement leak after vertebroplasty and kyphoplasty. Spine, 2002;27:2173-2178.Article
- 21. Pluijim SM, Tromp AM, Smit JH, Deeg DJ, Lips P. Consequences of vertebral deformities in older men and women. J Bone Miner Res, 2000;15:1564-1572.ArticlePDF
- 22. Schlaich C, Minne HW, Bruckner T, et al. Reduced pulmonary function in patients with spinal osteoporotic fractures. Osteoporos Int, 1998;8:261-267.ArticlePDF
- 23. Shindle MK, Gardner MJ, Koob J, Bukata S, Cabin JA, Lane JM. Vertebral height restoration in osteoporotic compression fractures: kyphoplasty balloon tamp is superior to postural correction alone. Osteoporos Int, 2006;17:1815-1819.ArticlePDF
- 24. Silverman SL. The clinical consequences of vertebral compression fracture. Bone, 1992;13:Suppl 2. S27-S31.Article
- 25. Voggenreiter G. Balloon kyphoplasty is effective in deformity correction of osteoporotic vertebral compression fractures. Spine, 2005;30:2806-2812.Article
REFERENCES

Fig. 2
(B) Prone position restored some vertebral height and reduced some kyphotic angle.
(C) Ballooning the bone tamp.
(D) Deflation the bone tamp and loss of restored vertebral height.
(E) Inseting the cement under fluoroscopic guidance.
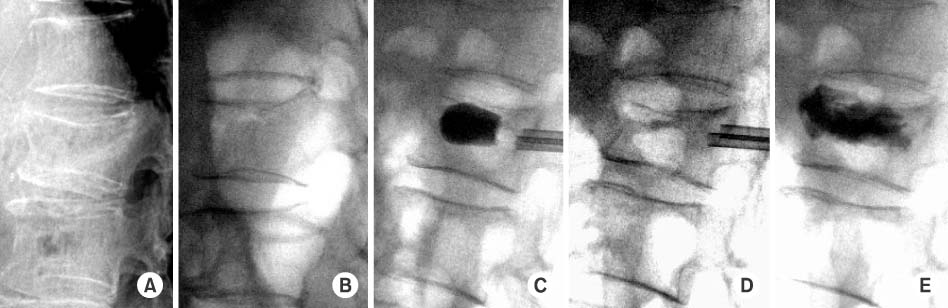
(A) Preoperative lateral radiograph was taken at lateral decubitus position.
Fig. 3
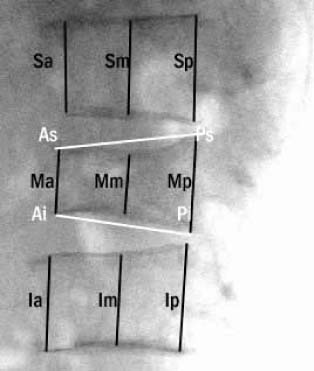
Measurement of kyphotic angle, anterior VB height, middle VB height, Posterior VB height Kyphotic angle is the angle between the line As-Ps and Ai-Pi. To minimize possible magnification effects, vertebral height were reported as fractions of referent height. Anterior body height (%)=2Ma/Sa+Ia, Middle body height (%)=2Mm/Sm+Im, Posterior body height (%)=2Mp/Sp+Ip.

Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteThe Factors that Affect the Deformity Correction of Vertebral Body during Kyphoplasty of Osteoporotic Vertebral Compression Fracture

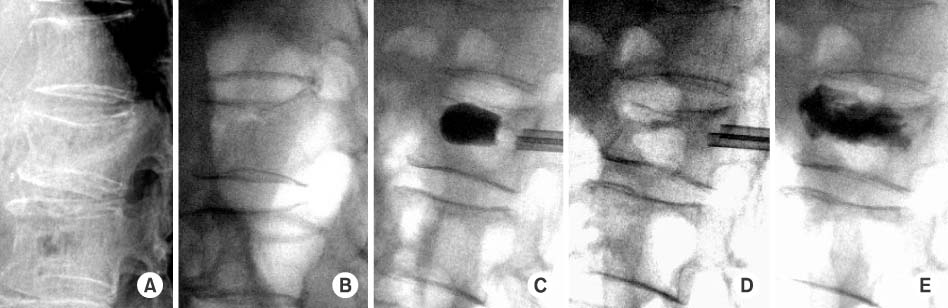
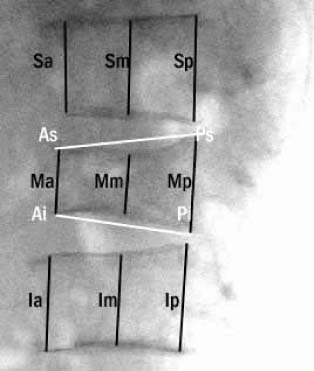
Fig. 1
Positioning of the patient on the operating table throughout the operative procedure.
Fig. 2
(A) Preoperative lateral radiograph was taken at lateral decubitus position.
(B) Prone position restored some vertebral height and reduced some kyphotic angle.
(C) Ballooning the bone tamp.
(D) Deflation the bone tamp and loss of restored vertebral height.
(E) Inseting the cement under fluoroscopic guidance.
Fig. 3
Measurement of kyphotic angle, anterior VB height, middle VB height, Posterior VB height Kyphotic angle is the angle between the line As-Ps and Ai-Pi. To minimize possible magnification effects, vertebral height were reported as fractions of referent height. Anterior body height (%)=2Ma/Sa+Ia, Middle body height (%)=2Mm/Sm+Im, Posterior body height (%)=2Mp/Sp+Ip.
Fig. 1
Fig. 2
Fig. 3
The Factors that Affect the Deformity Correction of Vertebral Body during Kyphoplasty of Osteoporotic Vertebral Compression Fracture
Summary of results
Values are given as mean: comparisons by T-test. IBT: Inflatable bone tamp, VB: Vertebral body. *p<0.001, †0.001<p<0.01, ‡0.01<p<0.05, §p>0.05, ∥p>0.05 for prone position vs. deflation of IBT, ¶p<0.005 for preoperative vs. cementing, **p>0.05 for preoperative vs. cementing.
Table 1
Summary of results
Values are given as mean: comparisons by T-test. IBT: Inflatable bone tamp, VB: Vertebral body. *p<0.001, †0.001<p<0.01, ‡0.01<p<0.05, §p>0.05, ∥p>0.05 for prone position vs. deflation of IBT, ¶p<0.005 for preoperative vs. cementing, **p>0.05 for preoperative vs. cementing.

