 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(2); 2011 > Article
-
Case Report
- Thermal Injury Complicating Improperly Reamed Intramedullary Nailing of the Tibia: A Case Report
- Bo-Kun Kim, M.D., Hyun-Dae Shin, M.D., Ph.D., Jung-Mo Hwang, M.D.
-
Journal of the Korean Fracture Society 2011;24(2):178-184.
DOI: https://doi.org/10.12671/jkfs.2011.24.2.178
Published online: April 13, 2011
Department of Orthopaedic Surgery, Dong-A University Medical Center, Busan, Korea.
*Department of Orthopaedic Surgery, Chungnam National University Hospital, Daejeon, Korea.
- Address reprint requests to: Hyun-Dae Shin, M.D., Ph.D. Department of Orthopaedic Surgery, School of Medicine, Chungnam National University, 33, Daesa-ro, Jung-gu, Daejeon 301-721, Korea. Tel: 82-42-280-7349, Fax: 82-42-252-7098, hyunsd@cnu.ac.kr
• Received: October 24, 2010 • Revised: November 9, 2010 • Accepted: December 1, 2010
Copyright © 2011 The Korean Fracture Society
- 970 Views
- 6 Download
Abstract
- Endosteum and bone marrow thermal necrosis caused by reaming during tibial intramedullary nail insertion, and unskilled operation of soft tissue penestration by reamer resulted in chronic osteomyelitis and soft tissue defect. So, several times of free flaps were done but the result was unsuccessful. At last, the authors performed radical necrotic bone resection and internal bone transport using Ilizarov external fixator. The authors report case with literature review.
- 1. Court-Brown CM. Reamed intramedullary tibial nailing: an overview and analysis of 1106 cases. J Orthop Trauma, 2004;18:96-101.
- 2. García OG, Mombiela FL, De La Fuente CJ, Aránguez MG, Escribano DV, Martín JV. The influence of the size and condition of the reamers on bone temperature during intramedullary reaming. J Bone Joint Surg Am, 2004;86-A:994-999.
- 3. Giannoudis PV, Snowden S, Matthews SJ, Smye SW, Smith RM. Friction burns within the tibia during reaming. Are they affected by the use of a tourniquet? J Bone Joint Surg Br, 2002;84:492-496.
- 4. Kocaoglu M, Eralp L, Rashid HU, Sen C, Bilsel K. Reconstruction of segmental bone defects due to chronic osteomyelitis with use of an external fixator and an intramedullary nail. J Bone Joint Surg Am, 2006;88:2137-2145.Article
- 5. Leunig M, Hertel R. Thermal necrosis after tibial reaming for intramedullary nail fixation. A report of three cases. J Bone Joint Surg Br, 1996;78:584-587.
- 6. Riemer BL, Foglesong ME, Burke CJ 3rd, Butterfield SL. Complications of Seidel intramedullary nailing of narrow diameter humeral diaphyseal fractures. Orthopedics, 1994;17:19-29.Article
- 7. Schmidt AH, Finkemeier CG, Tornetta P 3rd. Treatment of closed tibial fractures. Instr Course Lect, 2003;52:607-622.Article
- 8. Yazar S, Lin CH, Wei FC. One-stage reconstruction of composite bone and soft-tissue defects in traumatic lower extremities. Plast Reconstr Surg, 2004;114:1457-1466.Article
REFERENCES
Fig. 1
(A, B) Anteroposterior and lateral radiographs show displaced fracture of tibia and fibula due to rolling over.
(C, D) Closed reduction and internal fixation using interlocking intramedullary nail was performed.
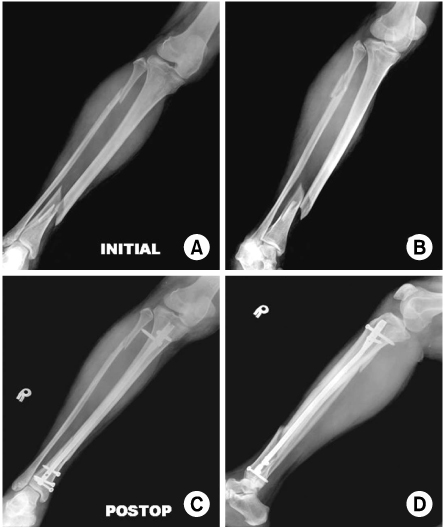
Fig. 2
(A~D) CT angiogram was taken before the anterolateral free flap on right lower leg. No remarkable finding in external iliac artery to popliteal artery but anterior tibial artery, posterior tibial artery and peroneal artery were not preserved on the right side.

Fig. 3
(A, B) 3 phase whole body bone scan with Tc-99m HDP was performed before the anterolateral thigh free flap on right lower leg and shows the perfusion and spatial distribution of tibial sequestration due to thermal necrosis.
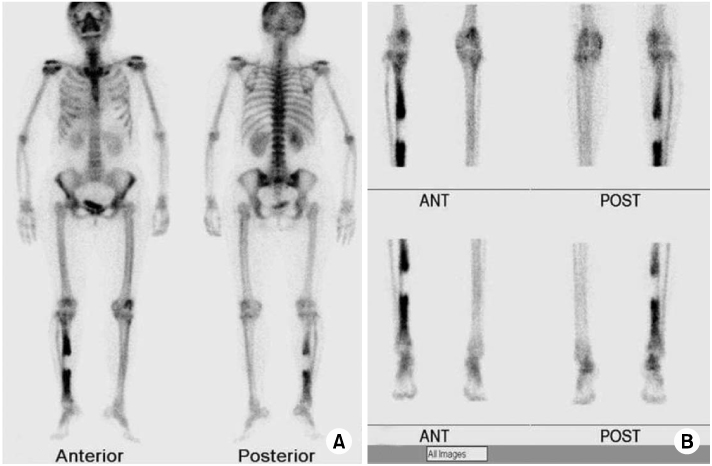
Fig. 4
(A, B) Photographs of the patient's right lower leg after the anterolateral thigh free flap was performed and failed. The tibial shaft was exposured and the soft tissue defection was approximately 7.3×2.5 cm.
(C) Fibular osteocutaneous free flap was performed.
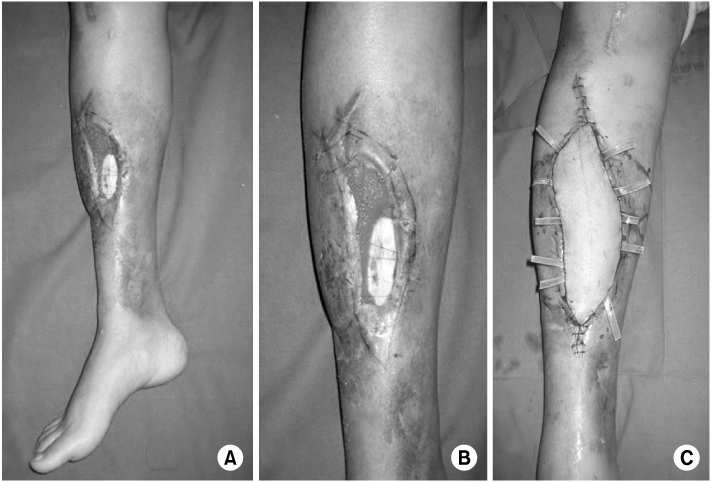
Fig. 5
(A, B) 3 phase whole body bone scan with Tc-99m HDP was performed after the fibular osteocutaneous free flap, and shows chronic osteomyelitis of the right tibia.
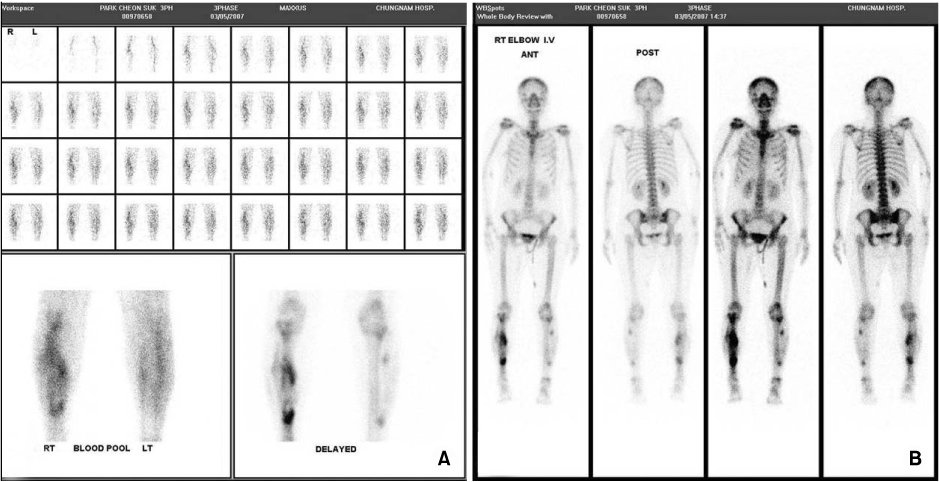
Fig. 6
(A, B) Postoperative anteroposterior and lateral radiographs. Radical necrotic bone resection (100 mm) and bifocal Ilizarov frame was inserted.
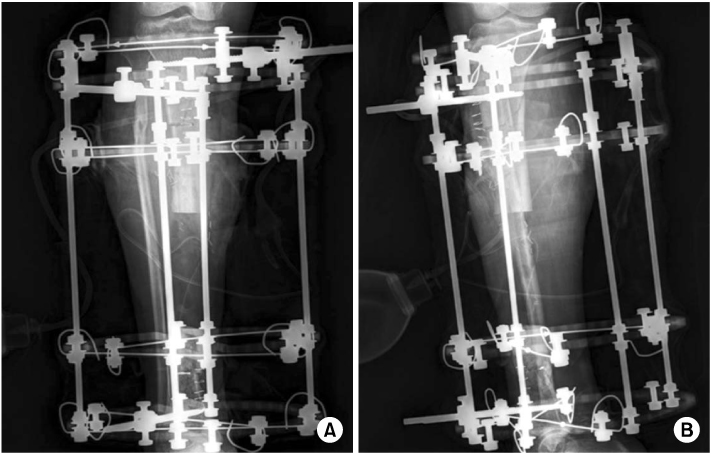
Fig. 7
(A, B) Follow up study at three months after operation. Internal transport was finished and consolidation of regenerates was visible, and bone graft and bone marrow injection was performed at the docking site.
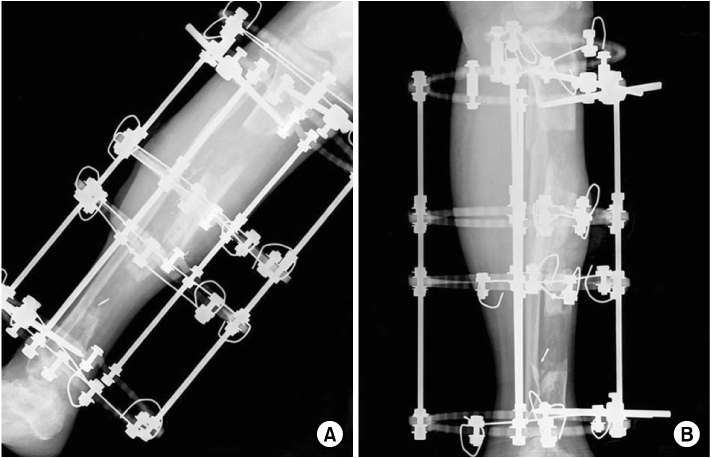
Fig. 8
(A, B) Follow up study at one years after operation. The quality of bone was excellent and union was successful.
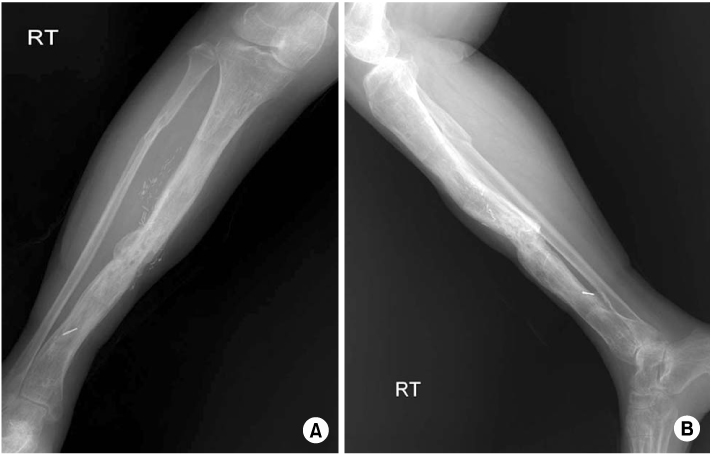
Fig. 9
Follow up photos at 2 years after operation.
(A) She hasn't felt both limb length discrepancy and angulations despite there were multiple scars.
(B) The dorsiflexion of ankle was possible as 95 degrees.
(C) The patient's knee flexion was as possible as 100 degrees in standing position, and (D) full extension was available.
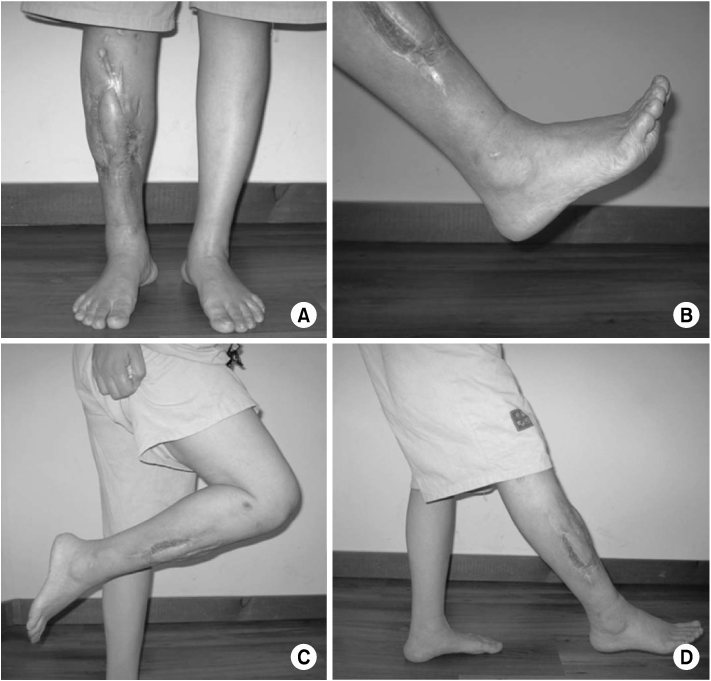
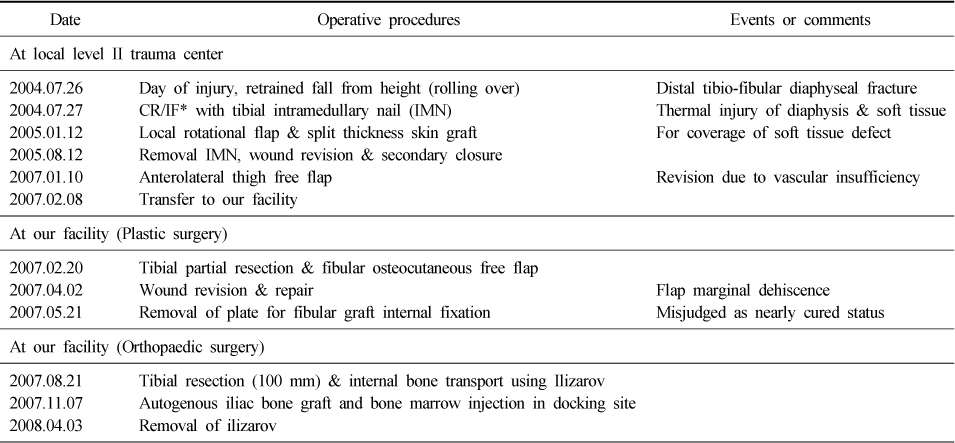
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteThermal Injury Complicating Improperly Reamed Intramedullary Nailing of the Tibia: A Case Report
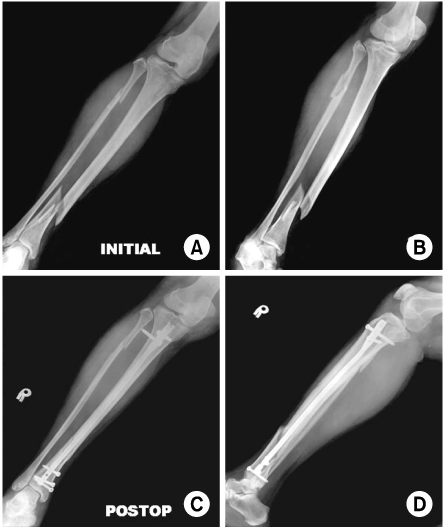

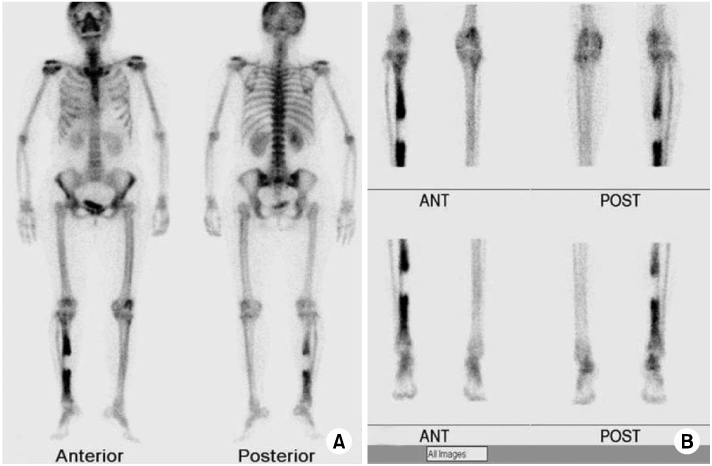
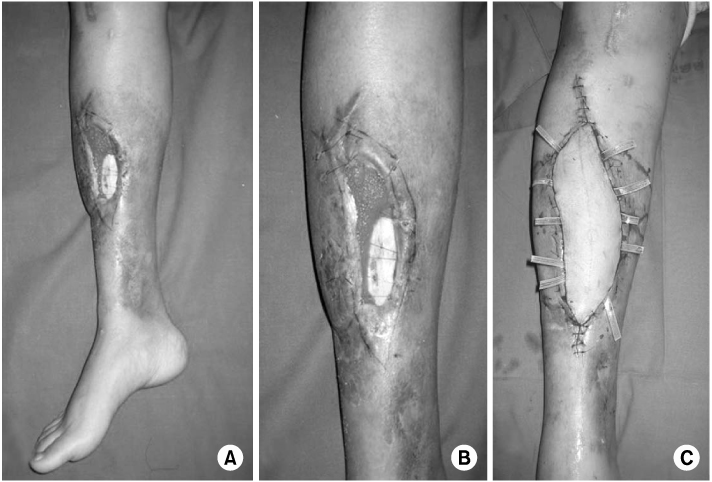
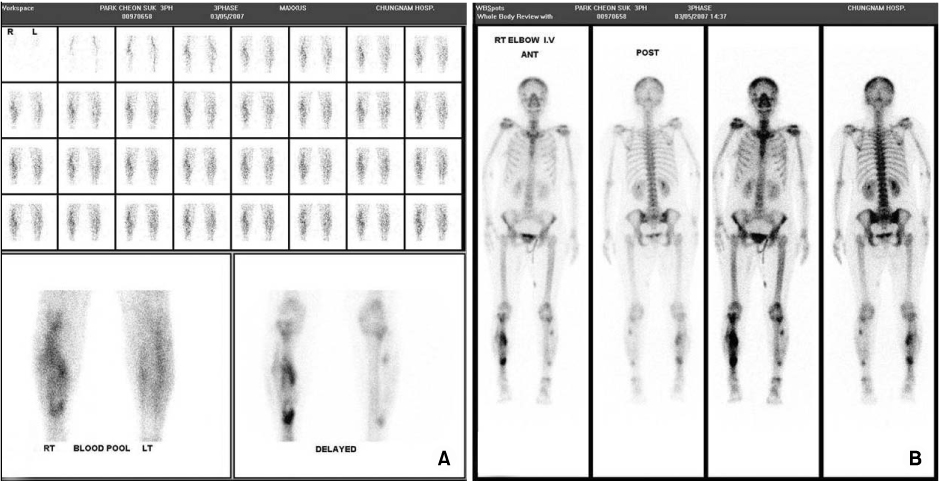
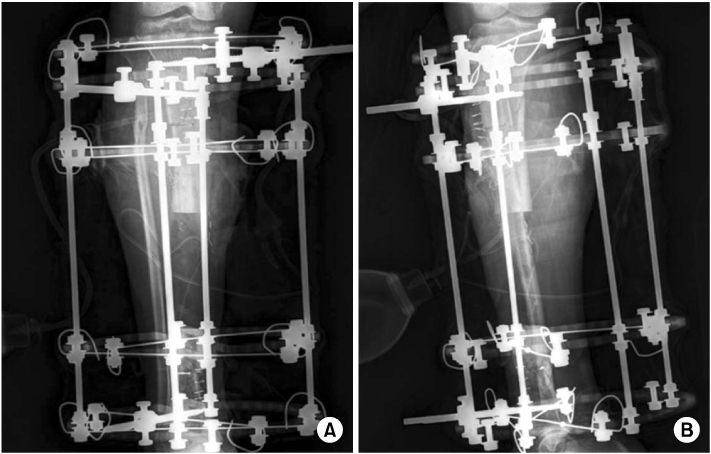
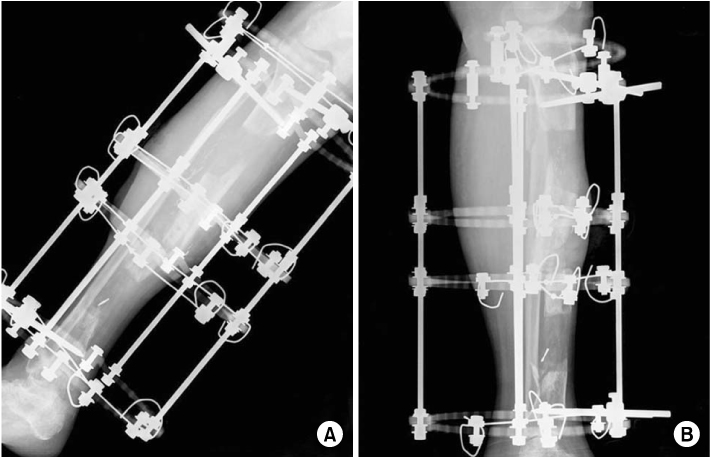
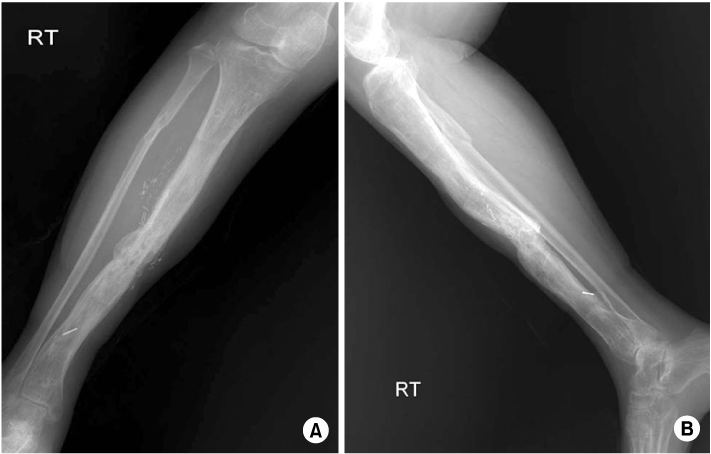
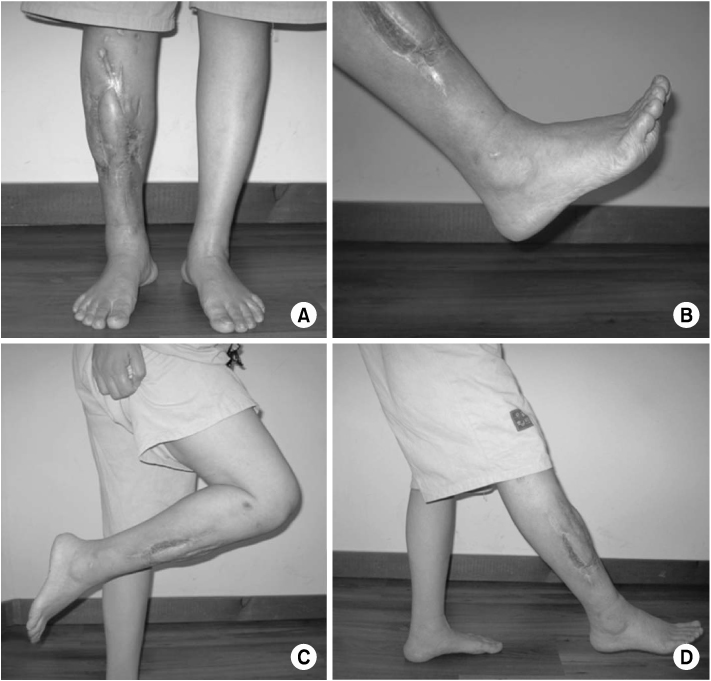
Fig. 1
(A, B) Anteroposterior and lateral radiographs show displaced fracture of tibia and fibula due to rolling over.
(C, D) Closed reduction and internal fixation using interlocking intramedullary nail was performed.
Fig. 2
(A~D) CT angiogram was taken before the anterolateral free flap on right lower leg. No remarkable finding in external iliac artery to popliteal artery but anterior tibial artery, posterior tibial artery and peroneal artery were not preserved on the right side.
Fig. 3
(A, B) 3 phase whole body bone scan with Tc-99m HDP was performed before the anterolateral thigh free flap on right lower leg and shows the perfusion and spatial distribution of tibial sequestration due to thermal necrosis.
Fig. 4
(A, B) Photographs of the patient's right lower leg after the anterolateral thigh free flap was performed and failed. The tibial shaft was exposured and the soft tissue defection was approximately 7.3×2.5 cm.
(C) Fibular osteocutaneous free flap was performed.
Fig. 5
(A, B) 3 phase whole body bone scan with Tc-99m HDP was performed after the fibular osteocutaneous free flap, and shows chronic osteomyelitis of the right tibia.
Fig. 6
(A, B) Postoperative anteroposterior and lateral radiographs. Radical necrotic bone resection (100 mm) and bifocal Ilizarov frame was inserted.
Fig. 7
(A, B) Follow up study at three months after operation. Internal transport was finished and consolidation of regenerates was visible, and bone graft and bone marrow injection was performed at the docking site.
Fig. 8
(A, B) Follow up study at one years after operation. The quality of bone was excellent and union was successful.
Fig. 9
Follow up photos at 2 years after operation.
(A) She hasn't felt both limb length discrepancy and angulations despite there were multiple scars.
(B) The dorsiflexion of ankle was possible as 95 degrees.
(C) The patient's knee flexion was as possible as 100 degrees in standing position, and (D) full extension was available.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Thermal Injury Complicating Improperly Reamed Intramedullary Nailing of the Tibia: A Case Report
A schematic summary of the patient's management
*CR/IF: Closed reduction/Internal fixaion.
Table 1
A schematic summary of the patient's management
*CR/IF: Closed reduction/Internal fixaion.

