 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 27(2); 2014 > Article
-
Original Article
- Tension Band Wiring for Distal Clavicle Fracture: Radiologic Analysis and Clinical Outcome
- Seong Cheol Moon, M.D., Chul Hee Lee, M.D., Jong Hoon Baek, M.D., Nam Su Cho, M.D., Yong Girl Rhee, M.D.
-
Journal of the Korean Fracture Society 2014;27(2):127-135.
DOI: https://doi.org/10.12671/jkfs.2014.27.2.127
Published online: April 18, 2014
Department of Orthopaedic Surgery, Kyung Hee University Medical Center, Seoul, Korea.
- Address reprint requests to: Yong Girl Rhee, M.D. Department of Orthopaedic Surgery, Kyung Hee University Medical Center, 23 Kyungheedae-ro, Dongdaemun-gu, Seoul 130-872, Korea. Tel: 82-2-958-8360, Fax: 82-2-964-3865, shoulderrhee@hanmail.com
• Received: June 7, 2013 • Revised: September 5, 2013 • Accepted: January 18, 2014
Copyright © 2014 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,481 Views
- 12 Download
- 1 Crossref
Abstract
-
Purpose
- The purpose of this study is to evaluate the radiologic and clinical outcomes after tension band wire fixation of Neer type II distal clavicle fractures.
-
Materials and Methods
- Twenty-six patients with Neer type II distal clavicle fractures who underwent tension band wire fixation from March 2002 to May 2011 were included in the study. Fifteen cases were classified as Neer type IIa and 11 cases as type IIb. The postoperative mean follow-up period was 14.3 months. Clinical and radiologic evaluation was performed at two weeks, six weeks, three months, six months, and 12 months postoperatively.
-
Results
- Bony union on X-rays was observed at an average of 11.7 weeks (range 8-20 weeks) postoperatively. The overall visual analogue scale score for pain was 1.23±2.75 postoperatively. The overall postoperative University of California at Los Angeles score increased to 33.5±2.15 from the preoperative score of 21.6±1.91 (p<0.05).
-
Conclusion
- Among various methods of treatment for Neer type II distal clavicle fracture, K-wire and tension band fixation was used and relatively satisfactory radiological and clinical results were obtained. This surgical method yields excellent clinical results, owing to its relatively easy technique, fewer complications, and allowance of early rehabilitation.
- 1. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am, 2004;86:778-782.ArticlePubMed
- 2. Neer CS 2nd. Nonunion of the clavicle. J Am Med Assoc, 1960;172:1006-1011.ArticlePubMed
- 3. Neer CS 2nd. Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma, 1963;3:99-110.ArticlePubMed
- 4. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res, 1968;58:43-50.PubMed
- 5. Herrmann S, Schmidmaier G, Greiner S. Stabilisation of vertical unstable distal clavicular fractures (Neer 2b) using locking T-plates and suture anchors. Injury, 2009;40:236-239.ArticlePubMed
- 6. Hessmann M, Kirchner R, Baumgaertel F, Gehling H, Gotzen L. Treatment of unstable distal clavicular fractures with and without lesions of the acromioclavicular joint. Injury, 1996;27:47-52.ArticlePubMed
- 7. Lyons FA, Rockwood CA Jr. Migration of pins used in operations on the shoulder. J Bone Joint Surg Am, 1990;72:1262-1267.ArticlePubMed
- 8. Ahn BW, Yoon JH, Kim CK, et al. Internal fixation of clavicle lateral and fracture with mini T-plate. J Korean Fract Soc, 2005;18:410-414.Article
- 9. Zenni EJ Jr, Krieg JK, Rosen MJ. Open reduction and internal fixation of clavicular fractures. J Bone Joint Surg Am, 1981;63:147-151.ArticlePubMed
- 10. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand, 2002;73:50-53.ArticlePubMed
- 11. Fukuda K, Craig EV, An KN, Cofield RH, Chao EY. Biomechanical study of the ligamentous system of the acromioclavicular joint. J Bone Joint Surg Am, 1986;68:434-440.ArticlePubMed
- 12. Mall JW, Jacobi CA, Philipp AW, Peter FJ. Surgical treatment of fractures of the distal clavicle with polydioxanone suture tension band wiring: an alternative osteosynthesis. J Orthop Sci, 2002;7:535-537.ArticlePubMed
- 13. Renfree KJ, Wright TW. Anatomy and biomechanics of the acromioclavicular and sternoclavicular joints. Clin Sports Med, 2003;22:219-237.ArticlePubMed
- 14. Neviaser RJ. Injuries to the clavicle and acromioclavicular joint. Orthop Clin North Am, 1987;18:433-438.ArticlePubMed
- 15. Renger RJ, Roukema GR, Reurings JC, Raams PM, Font J, Verleisdonk EJ. The clavicle hook plate for Neer type II lateral clavicle fractures. J Orthop Trauma, 2009;23:570-574.ArticlePubMed
- 16. Banerjee R, Waterman B, Padalecki J, Robertson W. Management of distal clavicle fractures. J Am Acad Orthop Surg, 2011;19:392-401.ArticlePubMed
- 17. Chung WY, Lee WS, Jeon TS, Kim DH, Kim KK, Lim JW. Treatment of distal clavicle type II fracture using K-wires and tension band wiring. J Korean Soc Fract, 2003;16:215-221.Article
- 18. Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta Orthop Scand, 1993;64:87-91.ArticlePubMed
- 19. Edwards DJ, Kavanagh TG, Flannery MC. Fractures of the distal clavicle: a case for fixation. Injury, 1992;23:44-46.ArticlePubMed
- 20. Eskola A, Vainionpää S, Pätiälä H, Rokkanen P. Outcome of operative treatment in fresh lateral clavicular fracture. Ann Chir Gynaecol, 1987;76:167-169.PubMed
- 21. Kona J, Bosse MJ, Staeheli JW, Rosseau RL. Type II distal clavicle fractures: a retrospective review of surgical treatment. J Orthop Trauma, 1990;4:115-120.PubMed
- 22. Leppilahti J, Jalovaara P. Migration of Kirschner wires following fixation of the clavicle--a report of 2 cases. Acta Orthop Scand, 1999;70:517-519.ArticlePubMed
- 23. Yamaguchi H, Arakawa H, Kobayashi M. Results of the Bosworth method for unstable fractures of the distal clavicle. Int Orthop, 1998;22:366-368.ArticlePubMedPMCPDF
- 24. Kao FC, Chao EK, Chen CH, Yu SW, Chen CY, Yen CY. Treatment of distal clavicle fracture using Kirschner wires and tension-band wires. J Trauma, 2001;51:522-525.ArticlePubMed
- 25. Chun JM, Kim SY, Lee KW, Shin SJ, Kim EG. Modified tenson band fixation for unstable fracture of the distal clavicle. J Korean Orthop Assoc, 2002;37:416-420.ArticlePDF
REFERENCES
Fig. 1
(A) Neer and Rockwood classification of distal clavicle fracture IIa: both the conoid and the trapezoid ligaments remain attached to the distal fragment. (B) Neer and Rockwood classification of distal clavicle fracture IIb: medial fragment instability is a result of disruption of the conoid ligament.
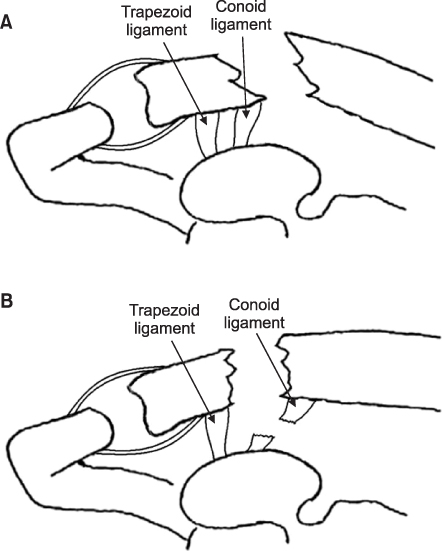
Fig. 2
(A) Preoperative radiologic analysis. a: acromioclavicular distance (ACD), b: coracoclavicular distance (CCD), c: acromioclavicular interval (ACI). (B) Postoperative radiologic analysis. a: ACD, b: CCD, c: ACI after K-wire insertion. ACI is increased. But, CCD is decreased.
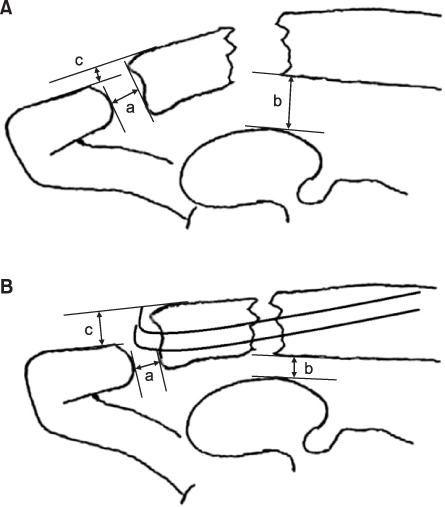
Fig. 3A 47-year-old women injured by traffic accident. Type IIa. (A) The radiograph shows a type IIa distal clavicle fracture of the left shoulder. Coracoclavicular (CC) distance b increased. (B) Postoperative radiograph shows a distal clavicle fracture fixed with tension band wiring. CC distance b was decreased, acromioclavicular (AC) interval c was increased. (C) After removal of wires at postoperative one year, AC interval c was reduced as compared with immediate postoperative radiograph.
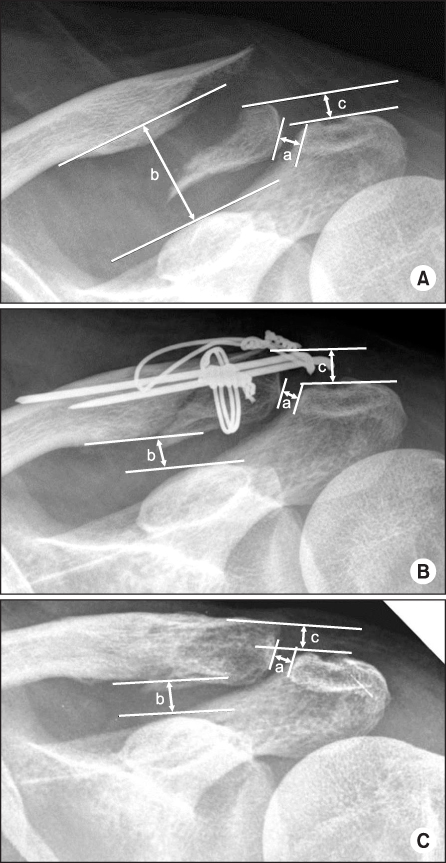
Fig. 4A 24-year-old man injured by falling down. Type IIb. (A) The radiograph shows a type IIb distal clavicle fracture of the left shoulder. Coracoclavicular (CC) distance b increased. (B) Postoperative radiograph shows a distal clavicle fracture fixed with tension band wiring. CC distance b was decreased, acromioclavicular (AC) interval c was increased. (C) After removal of wires at postoperative one year, AC interval c was reduced as compared with immediate postoperative radiograph.
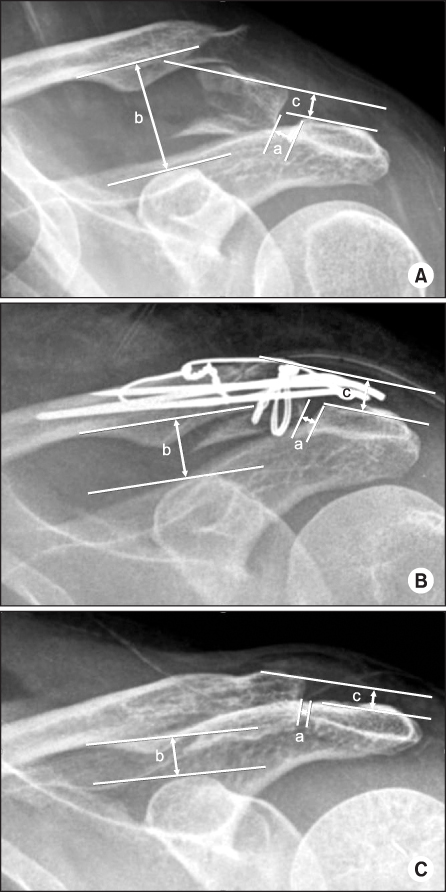
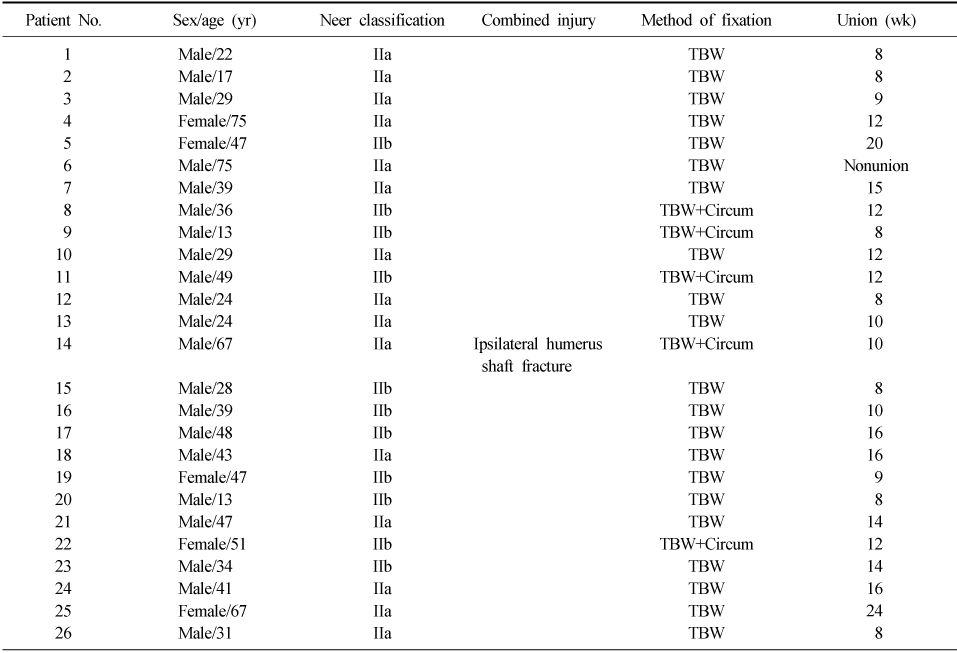
Table 2Radiologic Outcome of Distal Clavicle Fracture Treatment: At Base Line and at the Last Follow-Up
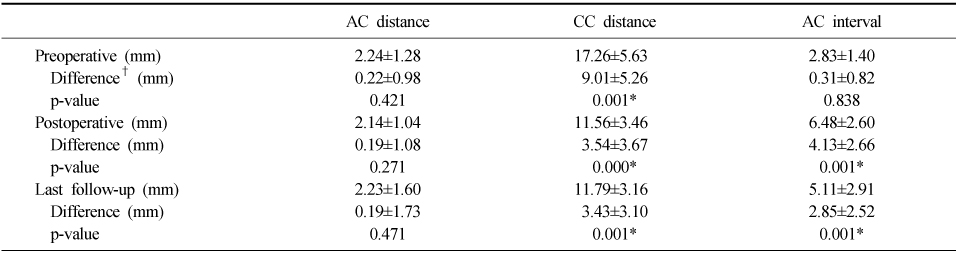

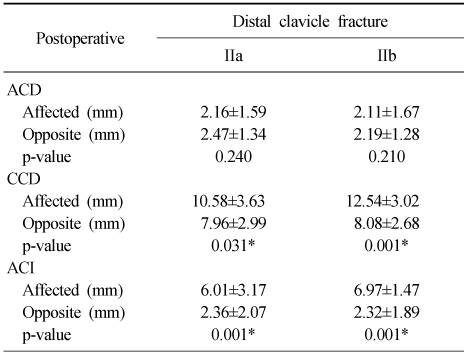
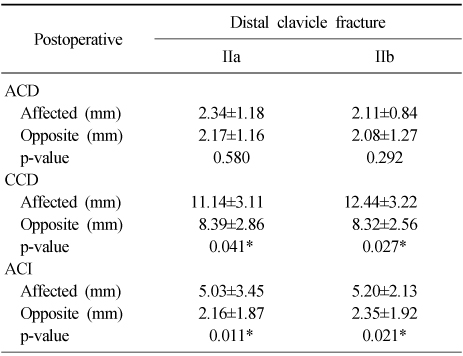
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Clinical and Radiologic Outcomes of Acute Acromioclavicular Joint Dislocation: Comparison of Kirschner's Wire Transfixation and Locking Hook Plate Fixation
Yong Girl Rhee, Jung Gwan Park, Nam Su Cho, Wook Jae Song
Clinics in Shoulder and Elbow.2014; 17(4): 159. CrossRef
 Cite
CiteTension Band Wiring for Distal Clavicle Fracture: Radiologic Analysis and Clinical Outcome
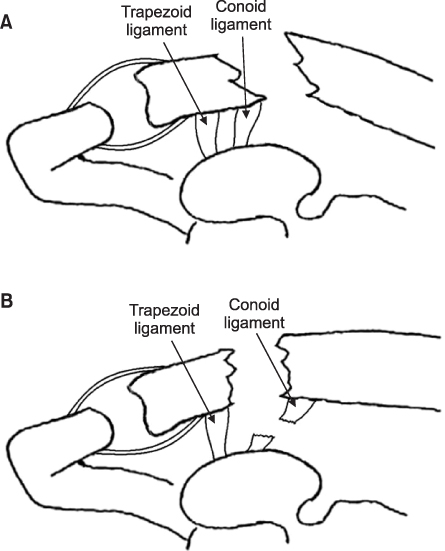
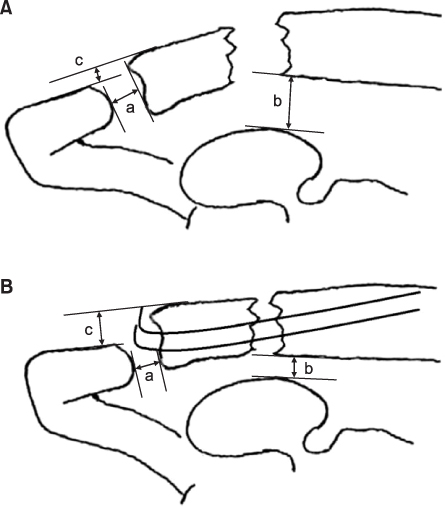
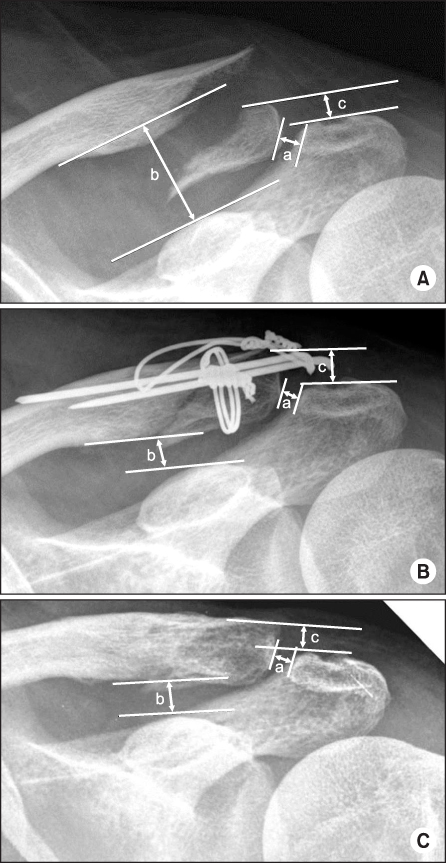
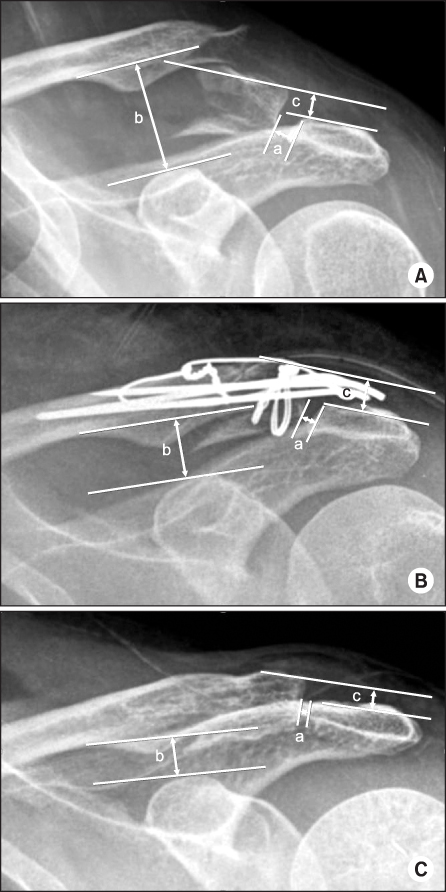
Fig. 1
(A) Neer and Rockwood classification of distal clavicle fracture IIa: both the conoid and the trapezoid ligaments remain attached to the distal fragment. (B) Neer and Rockwood classification of distal clavicle fracture IIb: medial fragment instability is a result of disruption of the conoid ligament.
Fig. 2
(A) Preoperative radiologic analysis. a: acromioclavicular distance (ACD), b: coracoclavicular distance (CCD), c: acromioclavicular interval (ACI). (B) Postoperative radiologic analysis. a: ACD, b: CCD, c: ACI after K-wire insertion. ACI is increased. But, CCD is decreased.
Fig. 3
A 47-year-old women injured by traffic accident. Type IIa. (A) The radiograph shows a type IIa distal clavicle fracture of the left shoulder. Coracoclavicular (CC) distance b increased. (B) Postoperative radiograph shows a distal clavicle fracture fixed with tension band wiring. CC distance b was decreased, acromioclavicular (AC) interval c was increased. (C) After removal of wires at postoperative one year, AC interval c was reduced as compared with immediate postoperative radiograph.
Fig. 4
A 24-year-old man injured by falling down. Type IIb. (A) The radiograph shows a type IIb distal clavicle fracture of the left shoulder. Coracoclavicular (CC) distance b increased. (B) Postoperative radiograph shows a distal clavicle fracture fixed with tension band wiring. CC distance b was decreased, acromioclavicular (AC) interval c was increased. (C) After removal of wires at postoperative one year, AC interval c was reduced as compared with immediate postoperative radiograph.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Tension Band Wiring for Distal Clavicle Fracture: Radiologic Analysis and Clinical Outcome
Summary of Cases
TBW: Tension band wiring, Circum: Circumferential additional wiring.
Radiologic Outcome of Distal Clavicle Fracture Treatment: At Base Line and at the Last Follow-Up
Values are presented as mean±standard deviation. AC: Acromioclavicular, CC: Coracoclavicular. *Statistically significant (p<0.05). †Difference between affected side and normal side.
Preoperative Radiologic Outcome of Distal Clavicle Fracture IIa and IIb
Values are presented as mean±standard deviation. ACD: Acromioclavicular distance, CCD: Coracoclavicular distance, ACI: Acromioclavicular interval. *Statistically significant (p<0.05).
Immediate Postoperative Radiologic Outcome of Distal Clavicle Fracture IIa and IIb
Values are presented as mean±standard deviation. ACD: Acromioclavicular distance, CCD: Coracoclavicular distance, ACI: Acromioclavicular interval. *Statistically significant (p<0.05).
Last Follow-Up Radiologic Outcome of Distal Clavicle Fracture IIa and IIb
Values are presented as mean±standard deviation. ACD: Acromioclavicular distance, CCD: Coracoclavicular distance, ACI: Acromioclavicular interval. *Statistically significant (p<0.05).
Table 1
Summary of Cases
TBW: Tension band wiring, Circum: Circumferential additional wiring.
Table 2
Radiologic Outcome of Distal Clavicle Fracture Treatment: At Base Line and at the Last Follow-Up
Values are presented as mean±standard deviation. AC: Acromioclavicular, CC: Coracoclavicular. *Statistically significant (p<0.05). †Difference between affected side and normal side.
Table 3
Preoperative Radiologic Outcome of Distal Clavicle Fracture IIa and IIb
Values are presented as mean±standard deviation. ACD: Acromioclavicular distance, CCD: Coracoclavicular distance, ACI: Acromioclavicular interval. *Statistically significant (p<0.05).
Table 4
Immediate Postoperative Radiologic Outcome of Distal Clavicle Fracture IIa and IIb
Values are presented as mean±standard deviation. ACD: Acromioclavicular distance, CCD: Coracoclavicular distance, ACI: Acromioclavicular interval. *Statistically significant (p<0.05).
Table 5
Last Follow-Up Radiologic Outcome of Distal Clavicle Fracture IIa and IIb
Values are presented as mean±standard deviation. ACD: Acromioclavicular distance, CCD: Coracoclavicular distance, ACI: Acromioclavicular interval. *Statistically significant (p<0.05).

