 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 32(1); 2019 > Article
- Review Article Distal Humerus Fracture: How to Choose the Approach, Implant, Fixation and Rehabilitation
- Min Ho Lee, Young Ho Lee
-
Journal of Musculoskeletal Trauma 2019;32(1):72-81.
DOI: https://doi.org/10.12671/jkfs.2019.32.1.72
Published online: January 31, 2019
Department of Orthopedic Surgery, Seoul National University Hospital, Seoul, Korea. orthoyhl@snu.ac.kr
-
Corresponding author:
Young Ho Lee, Tel: +82-2-2072-0819, Fax: +82-2-740-2718,
Email: orthoyhl@snu.ac.kr
- 4,448 Views
- 248 Download
- 0 Crossref
- 0 Scopus
Abstract
Distal humerus fractures require stable fixation and early joint motion, similar to other intra-articular fractures, but are difficult to treat adequately because of the anatomical complexity, severe comminution, and accompanying osteoporosis. In most cases, surgical treatment is performed using two supporting plates. Plate fixation can be divided into right angle plate fixation and parallel plate fixation. In addition, depending on the type of fracture, surgical procedures can be performed differently, and autologous bone grafting can be required in the case of severe bone loss. The elbow joint is vulnerable to stiffness, so it is important to start joint movement early after surgery. Postoperative complications, such as nonunion, ulnar nerve compression, and heterotopic ossification, can occur. Therefore, accurate and rigid fixation and meticulous manipulation of soft tissues are required during surgery.
J Korean Fract Soc. 2019 Jan;32(1):72-81. Korean.
Published online Jan 25, 2019.
https://doi.org/10.12671/jkfs.2019.32.1.72
Published online Jan 25, 2019.
https://doi.org/10.12671/jkfs.2019.32.1.72
Copyright © 2019 The Korean Fracture Society. All rights reserved.
Review
Distal Humerus Fracture: How to Choose the Approach, Implant, Fixation and Rehabilitation
Min Ho Lee , M.D.
and Young Ho Lee, M.D., Ph.D.
, M.D.
and Young Ho Lee, M.D., Ph.D.
, M.D.
and Young Ho Lee, M.D., Ph.D.
Abstract
Distal humerus fractures require stable fixation and early joint motion, similar to other intra-articular fractures, but are difficult to treat adequately because of the anatomical complexity, severe comminution, and accompanying osteoporosis. In most cases, surgical treatment is performed using two supporting plates. Plate fixation can be divided into right angle plate fixation and parallel plate fixation. In addition, depending on the type of fracture, surgical procedures can be performed differently, and autologous bone grafting can be required in the case of severe bone loss. The elbow joint is vulnerable to stiffness, so it is important to start joint movement early after surgery. Postoperative complications, such as nonunion, ulnar nerve compression, and heterotopic ossification, can occur. Therefore, accurate and rigid fixation and meticulous manipulation of soft tissues are required during surgery.
Keywords
Elbow joint, Ulnar nerve, Heterotopic ossification
Figures
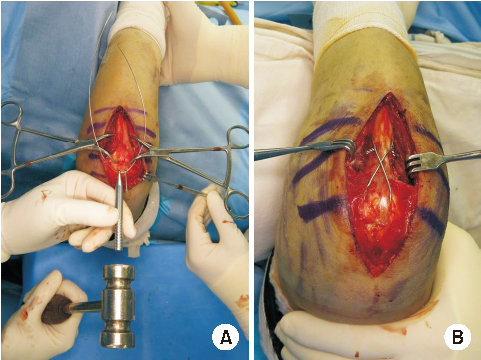
Fig. 1
Tension band wiring with ring pin. (A) Ring pin is inserted to olecranon using snapper. (B) Fracture site is compressed with 8-figure tension band wire.
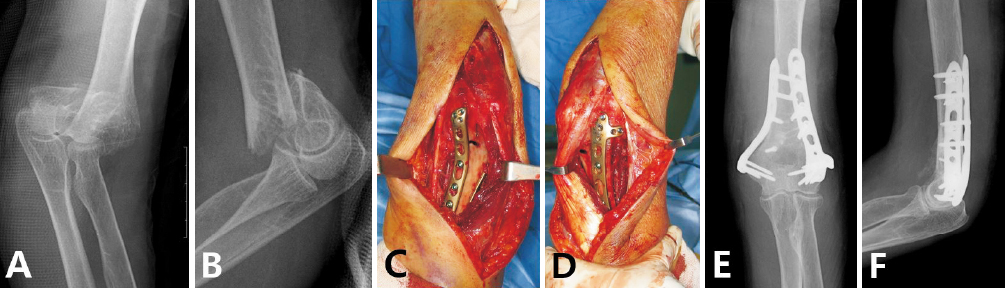
Fig. 2
Double plating of distal humerus fracture. (A, B) Preoperative X-ray. (C, D) Double plating at medial and lateral column. (E, F) Postoperative X-ray.
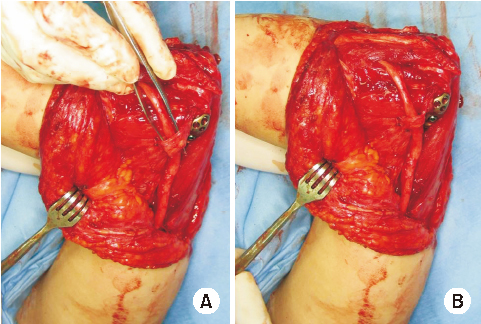
Fig. 3
Ulnar nerve anterior transposition. (A, B) Transposed ulnar nerve is stabilized with new tunnel made of medial intermuscular septum.
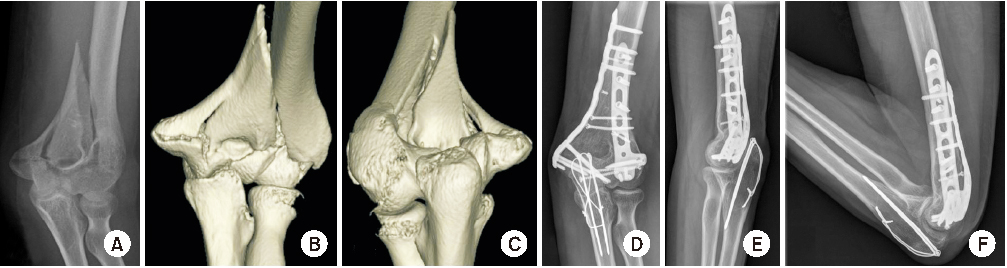
Fig. 4
Type 1 fracture. (A) Preoperative X-ray showed medial side large fracture fragment. (B, C) Three-dimensional computed tomography. (D) Large fragment was fixed with interfragmentary screw. (E, F) Three years after operation, range of motion is nearly normal.
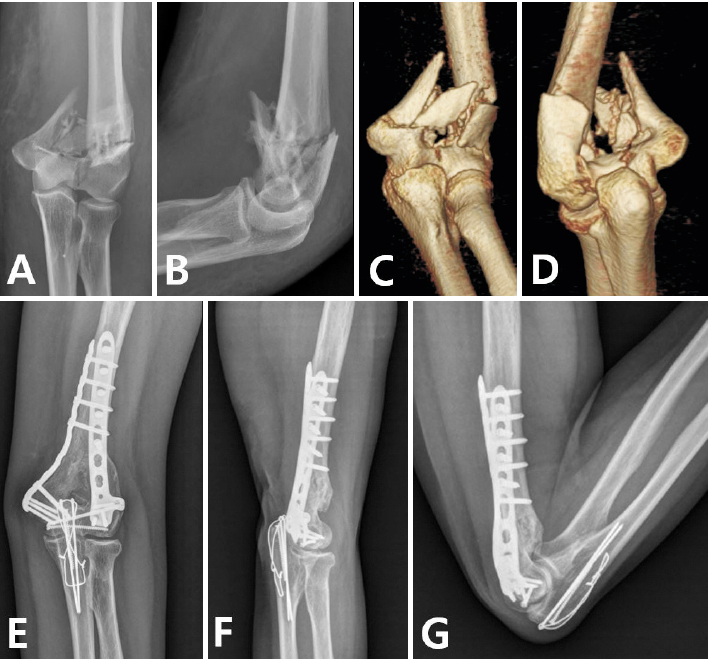
Fig. 5
Type 2 fracture. (A, B) Preoperative X-ray showed severe metaphyseal comminution. (C, D) Three-dimensional computed tomography. (E) Fracture was fixed by bridging plate. (F, G) Two years after operation, range of motion is nearly normal.
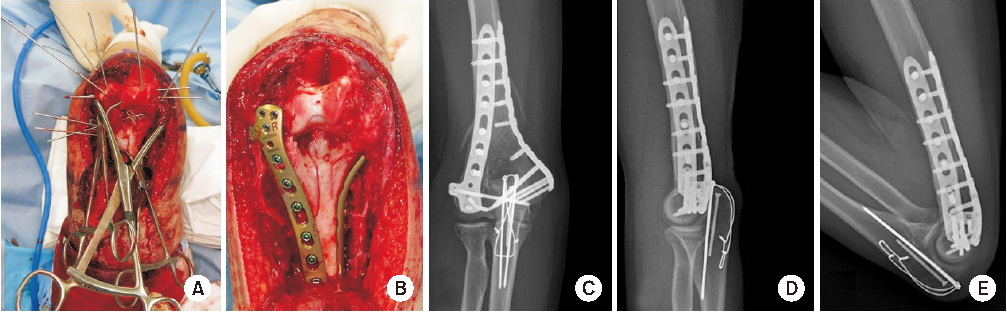
Fig. 6
Type 3 fracture. (A) Multiple comminuted articular bony fragment was reduced and fixed with K-wire. (B) Plate and screw was substituted by K-wire. (C–E) Postoperative X-ray showed stable reduction and normal range of motion.
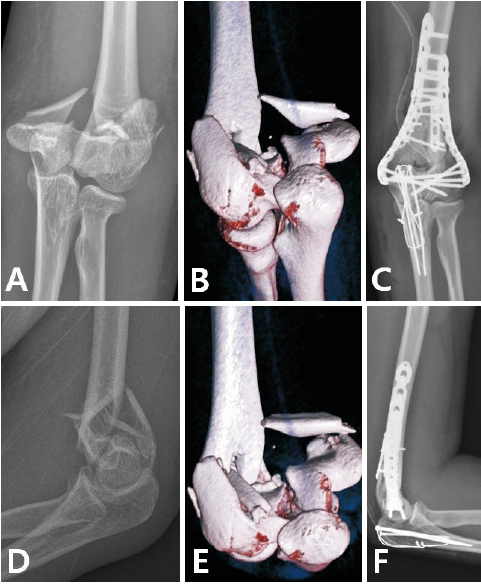
Fig. 7
Type 4 fracture. (A, B) Preoperative X-ray showed small metaphyseal bony fragment. (C, D) Three-dimensional computed tomography. (E, F) Small bony fragment was fixed with miniplate for simplifying fracture pattern, then reduced other fragment.
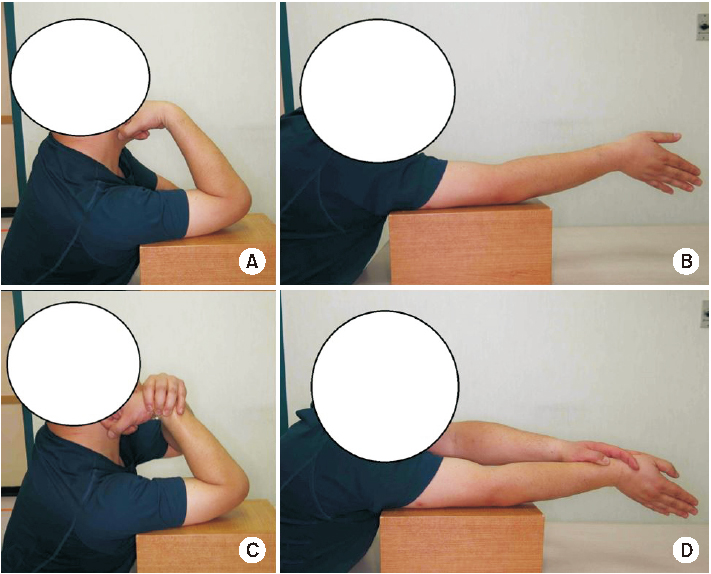
Fig. 8
Rehabilitation after operation. (A) Active elbow flexion. (B) Active assisted elbow flexion. (C) Active elbow extension. (D) Active assisted elbow extension.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Mighell MA, Stephens B, Stone GP, Cottrell BJ. Distal humerus fractures: open reduction internal fixation. Hand Clin 2015;31:591–604.
-
-
Nauth A, McKee MD, Ristevski B, Hall J, Schemitsch EH. Distal humeral fractures in adults. J Bone Joint Surg Am 2011;93:686–700.
-
-
Robinson CM, Hill RM, Jacobs N, Dall G, Court-Brown CM. Adult distal humeral metaphyseal fractures: epidemiology and results of treatment. J Orthop Trauma 2003;17:38–47.
-
-
Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium - 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21:S1–S133.
-
-
Jupiter JB, Mehne DK. Fractures of the distal humerus. Orthopedics 1992;15:825–833.
-
-
Srinivasan K, Agarwal M, Matthews SJ, Giannoudis PV. Fractures of the distal humerus in the elderly: is internal fixation the treatment of choice? Clin Orthop Relat Res 2005;(434):222–230.
-
-
Desloges W, Faber KJ, King GJ, Athwal GS. Functional outcomes of distal humeral fractures managed nonoperatively in medically unwell and lower-demand elderly patients. J Shoulder Elbow Surg 2015;24:1187–1196.
-
-
Rajaee SS, Lin CA, Moon CN. Primary total elbow arthroplasty for distal humeral fractures in elderly patients: a nationwide analysis. J Shoulder Elbow Surg 2016;25:1854–1860.
-
-
Prasad N, Ali A, Stanley D. Total elbow arthroplasty for non-rheumatoid patients with a fracture of the distal humerus: a minimum ten-year follow-up. Bone Joint J 2016;98-B:381–386.
-
-
Ring D, Gulotta L, Chin K, Jupiter JB. Olecranon osteotomy for exposure of fractures and nonunions of the distal humerus. J Orthop Trauma 2004;18:446–449.
-
-
Coles CP, Barei DP, Nork SE, Taitsman LA, Hanel DP, Bradford Henley M. The olecranon osteotomy: a six-year experience in the treatment of intraarticular fractures of the distal humerus. J Orthop Trauma 2006;20:164–171.
-
-
Elmadag M, Erdil M, Bilsel K, Acar MA, Tuncer N, Tuncay I. The olecranon osteotomy provides better outcome than the triceps-lifting approach for the treatment of distal humerus fractures. Eur J Orthop Surg Traumatol 2014;24:43–50.
-
-
Zhang C, Zhong B, Luo CF. Comparing approaches to expose type C fractures of the distal humerus for ORIF in elderly patients: six years clinical experience with both the triceps-sparing approach and olecranon osteotomy. Arch Orthop Trauma Surg 2014;134:803–811.
-
-
Kim JY, Lee YH, Gong HS, Lee SL, Lee SK, Baek GH. Use of Kirschner wires with eyelets for tension band wiring of olecranon fractures. J Hand Surg Am 2013;38:1762–1767.
-
-
Chen G, Liao Q, Luo W, Li K, Zhao Y, Zhong D. Tricepssparing versus olecranon osteotomy for ORIF: analysis of 67 cases of intercondylar fractures of the distal humerus. Injury 2011;42:366–370.
-
-
Campbell WC. Incision for exposure of the elbow joint. Am J Surg 1932;15:65–67.
-
-
McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR. Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82-A:1701–1707.
-
-
O'Driscoll SW. The triceps-reflecting anconeus pedicle (TRAP) approach for distal humeral fractures and nonunions. Orthop Clin North Am 2000;31:91–101.
-
-
Schildhauer TA, Nork SE, Mills WJ, Henley MB. Extensor mechanism-sparing paratricipital posterior approach to the distal humerus. J Orthop Trauma 2003;17:374–378.
-
-
Worden A, Ilyas AM. Ulnar neuropathy following distal humerus fracture fixation. Orthop Clin North Am 2012;43:509–514.
-
-
Chen RC, Harris DJ, Leduc S, Borrelli JJ Jr, Tornetta P 3rd, Ricci WM. Is ulnar nerve transposition beneficial during open reduction internal fixation of distal humerus fractures? J Orthop Trauma 2010;24:391–394.
-
-
Wiggers JK, Brouwer KM, Helmerhorst GT, Ring D. Predictors of diagnosis of ulnar neuropathy after surgically treated distal humerus fractures. J Hand Surg Am 2012;37:1168–1172.
-
-
Vazquez O, Rutgers M, Ring DC, Walsh M, Egol KA. Fate of the ulnar nerve after operative fixation of distal humerus fractures. J Orthop Trauma 2010;24:395–399.
-
-
Helfet DL, Hotchkiss RN. Internal fixation of the distal humerus: a biomechanical comparison of methods. J Orthop Trauma 1990;4:260–264.
-
-
Schuster I, Korner J, Arzdorf M, Schwieger K, Diederichs G, Linke B. Mechanical comparison in cadaver specimens of three different 90-degree double-plate osteosyntheses for simulated C2-type distal humerus fractures with varying bone densities. J Orthop Trauma 2008;22:113–120.
-
-
Hungerer S, Wipf F, von Oldenburg G, Augat P, Penzkofer R. Complex distal humerus fractures-comparison of polyaxial locking and nonlocking screw configurations: a preliminary biomechanical study. J Orthop Trauma 2014;28:130–136.
-
-
Jupiter JB, Neff U, Holzach P, Allgöwer M. Intercondylar fractures of the humerus. An operative approach. J Bone Joint Surg Am 1985;67:226–239.
-
-
Helfet DL, Schmeling GJ. Bicondylar intraarticular fractures of the distal humerus in adults. Clin Orthop Relat Res 1993;(292):26–36.
-
-
O'Driscoll SW. Optimizing stability in distal humeral fracture fixation. J Shoulder Elbow Surg 2005;14:186S–194S.
-
-
Sanchez-Sotelo J, Torchia ME, O'Driscoll SW. Complex distal humeral fractures: internal fixation with a principle-based parallel-plate technique. J Bone Joint Surg Am 2007;89:961–969.
-
-
Stoffel K, Cunneen S, Morgan R, Nicholls R, Stachowiak G. Comparative stability of perpendicular versus parallel double-locking plating systems in osteoporotic comminuted distal humerus fractures. J Orthop Res 2008;26:778–784.
-
-
Zalavras CG, Vercillo MT, Jun BJ, Otarodifard K, Itamura JM, Lee TQ. Biomechanical evaluation of parallel versus orthogonal plate fixation of intra-articular distal humerus fractures. J Shoulder Elbow Surg 2011;20:12–20.
-
-
Zalavras CG, McAllister ET, Singh A, Itamura JM. Operative treatment of intra-articular distal humerus fractures. Am J Orthop (Belle Mead NJ) 2007;36 12 Suppl 2:8–12.
-
 PubReader
PubReader Cite
Cite
