 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 27(3); 2014 > Article
-
Case Report
- Granulation Tissue Formed by Stimulating K-Wire Mimicking Tuberculous Cervical Lymphadenopathy: A Case Report
- Gu-Hee Jung, M.D., Tae-Hun Kim, M.D., Hyun-Ik Cho, M.D.
-
Journal of the Korean Fracture Society 2014;27(3):227-231.
DOI: https://doi.org/10.12671/jkfs.2014.27.3.227
Published online: July 16, 2014
Department of Orthopedic Surgery, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea.
- Address reprint requests to: Gu-Hee Jung, M.D. Department of Orthopedic Surgery, Kosin University Gospel Hospital, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan 602-702, Korea. Tel: 82-51-990-6229, Fax: 82-51-243-0181, jyujin2001@kosin.ac.kr
• Received: September 16, 2013 • Revised: June 12, 2014 • Accepted: June 12, 2014
Copyright © 2014 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 995 Views
- 0 Download
- 1 Crossref
Abstract
- Pins and wires are still used frequently in surgeries of the shoulder; however, these can cause breakage or migration to surrounding tissues, leading to complications. We report on case of a patient with a neck mass who had a past history of pulmonary tuberculosis and distal clavicle fracture with internally fixated state. She was misdiagnosed as tuberculous cervical lymphadenopathy and treated for approximately one year, but was finally revealed as granulation tissue around the internally fixated distal clavicle fracture site, thus, mass excision and metal removal was performed. This case shows the importance of a proper selection device, internal fixation technique, duration, and close follow-up after the operation.
- 1. Lyons FA, Rockwood CA Jr. Migration of pins used in operations on the shoulder. J Bone Joint Surg Am, 1990;72:1262-1267.ArticlePubMed
- 2. Sharma H, Taylor GR, Clarke NM. A review of K-wire related complications in the emergency management of paediatric upper extremity trauma. Ann R Coll Surg Engl, 2007;89:252-258.Article
- 3. Cheon SJ, Lee JM. Early intrathoracic migration of K-wire used for fixation of proximal humerus fracture. J Korean Orthop Assoc, 2011;46:167-171.Article
- 4. Lee BI, Kim YB, Choi HS, Kim CH, Ji JW. Spinal canal migration of a K-wire used for fixation of a distal clavicular fracture. J Korean Orthop Assoc, 2013;48:231-235.Article
- 5. Jean JL, Lee CH, Chu CM, Hsieh SP, Tang HL. Pseudocyst formation after intertrochanteric fracture fixation: a case report. J Formos Med Assoc, 2001;100:285-288.
- 6. Bisbinas I, Mikalef P, Gigis I, Beslikas T, Panou N, Christoforidis I. Management of distal clavicle fractures. Acta Orthop Belg, 2010;76:145-149.
- 7. Meda PV, Machani B, Sinopidis C, Braithwaite I, Brownson P, Frostick SP. Clavicular hook plate for lateral end fractures: a prospective study. Injury, 2006;37:277-283.Article
- 8. Wu K, Chang CH, Yang RS. Comparing hook plates and Kirschner tension band wiring for unstable lateral clavicle fractures. Orthopedics, 2011;34:e718-e723.ArticlePubMed
- 9. Lee YS, Lau MJ, Tseng YC, Chen WC, Kao HY, Wei JD. Comparison of the efficacy of hook plate versus tension band wire in the treatment of unstable fractures of the distal clavicle. Int Orthop, 2009;33:1401-1405.ArticlePubMed
- 10. Wang SG. Differential diagnosis and treatment of neck masses. J Korean Med Assoc, 2007;50:613-625.Article
REFERENCES

Fig. 2Axial cervical computed tomography scans. About 2.5 cm sized rim enhancing low density mass was seen at supraclavicular area. The tip of K-wire was in the mass. Black arrow: rim enchanced mass. White arrow: K-wire. (A) Lung setting, (B) bone setting.

Fig. 3Coronal cervical computed tomography scans confirmed migration of the K-wire into the mass, showing irritation of the mass by tip of the K-wire.



Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Kirschner Wire Migration into SpinaL Canal after Acromioclavicular Joint Fixation (Literature Review and Clinical Case)
D. A. Gulyaev, D. S. Godanyuk, T. A. Kaurova, P. V. Krasnoshlyk, S. V. Maikov
Traumatology and Orthopedics of Russia.2018; 24(4): 121. CrossRef
 Cite
CiteGranulation Tissue Formed by Stimulating K-Wire Mimicking Tuberculous Cervical Lymphadenopathy: A Case Report

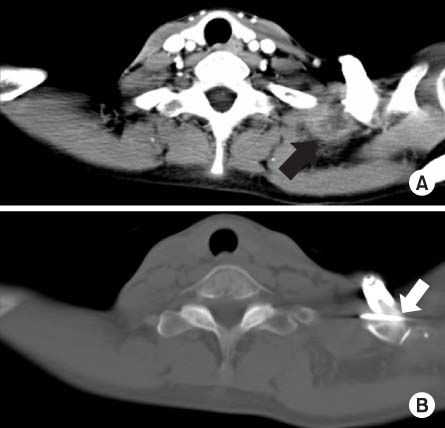
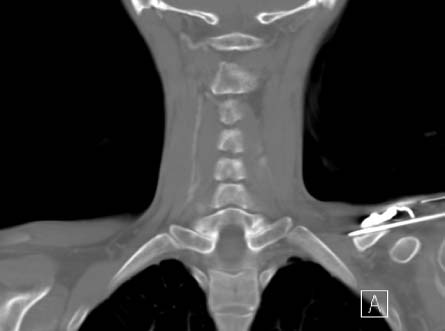
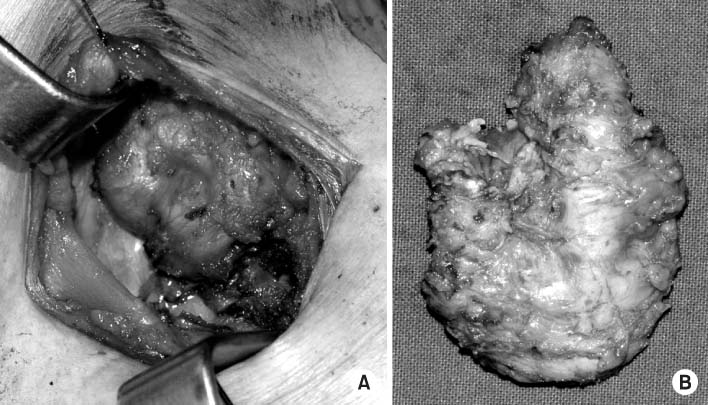
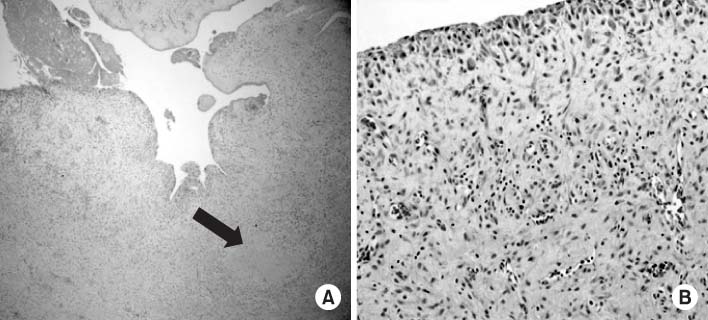
Fig. 1
Preoperative plane radiograph showed mild medial migration of K-wire.
Fig. 2
Axial cervical computed tomography scans. About 2.5 cm sized rim enhancing low density mass was seen at supraclavicular area. The tip of K-wire was in the mass. Black arrow: rim enchanced mass. White arrow: K-wire. (A) Lung setting, (B) bone setting.
Fig. 3
Coronal cervical computed tomography scans confirmed migration of the K-wire into the mass, showing irritation of the mass by tip of the K-wire.
Fig. 4
(A) Intraoperative finding of soft tissue mass during excional biopsy. (B) After excisional biopsy about 5.0×3.0×1.5 cm sized mass was removed.
Fig. 5
At the pathologic study nonspecific granulation tissue was seen (A, B), and local fibrosis was seen (black arrow) (H&E; A: ×40, B: ×100).
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Granulation Tissue Formed by Stimulating K-Wire Mimicking Tuberculous Cervical Lymphadenopathy: A Case Report

