 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(4); 2011 > Article
-
Review Article
- Sacral Fractures
- Young-Soo Byun, M.D., Se-Ang Chang, M.D.
-
Journal of the Korean Fracture Society 2011;24(4):371-381.
DOI: https://doi.org/10.12671/jkfs.2011.24.4.371
Published online: October 30, 2011
Department of Orthopedic Surgery, Daegu Fatima Hospital, Daegu, Korea.
- Address reprint requests to: Young-Soo Byun, M.D. Department of Orthopedic Surgery, Daegu Fatima Hospital, 576-31, Sinam-dong, Dong-gu, Daegu 701-600, Korea. Tel: 82-53-940-7320, Fax: 82-53-954-7417, fatimaos@unitel.co.kr
Copyright © 2011 The Korean Fracture Society
- 1,753 Views
- 24 Download
- 1 Crossref

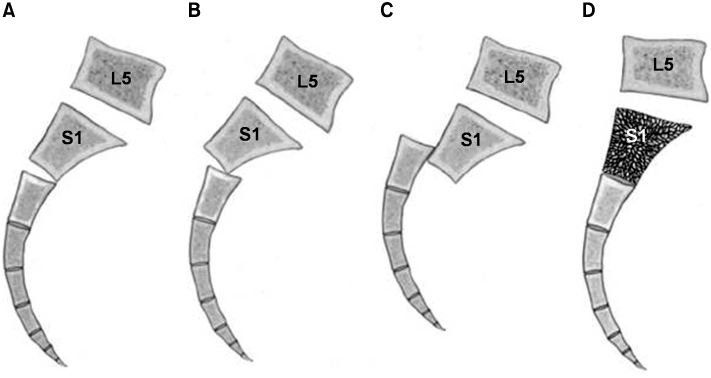
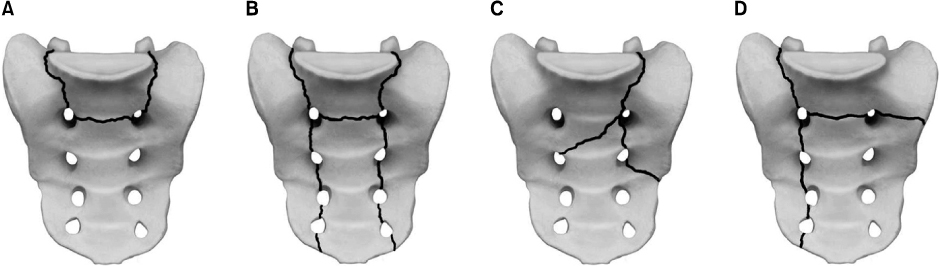
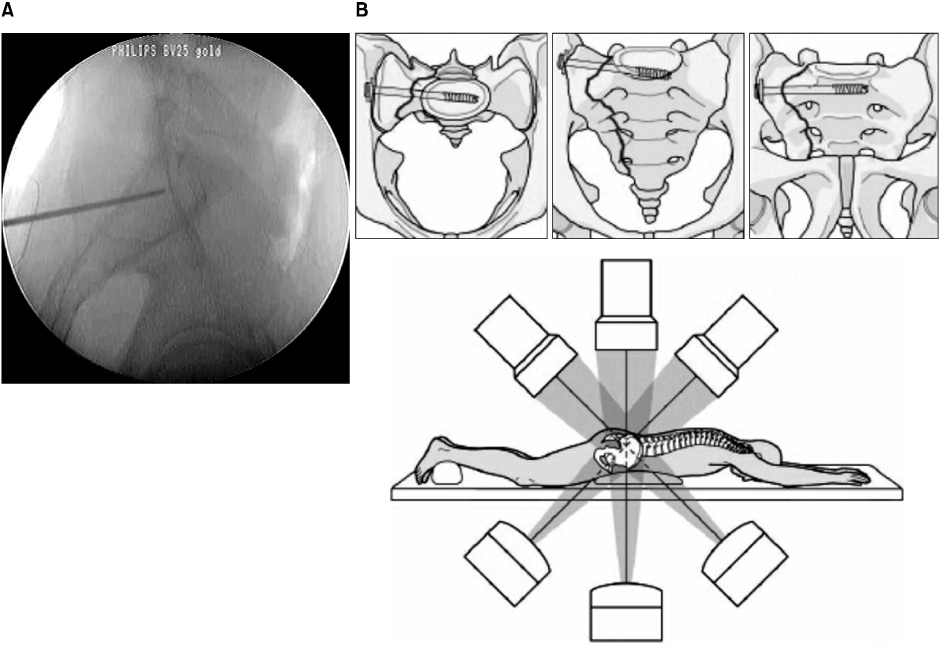
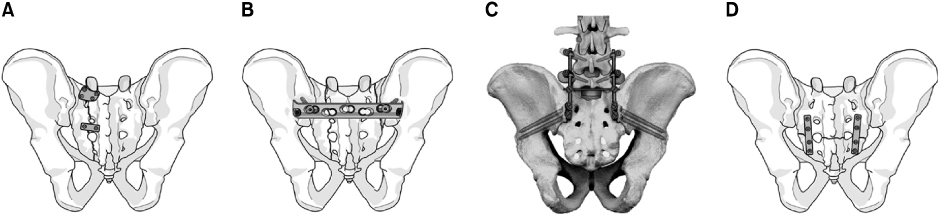
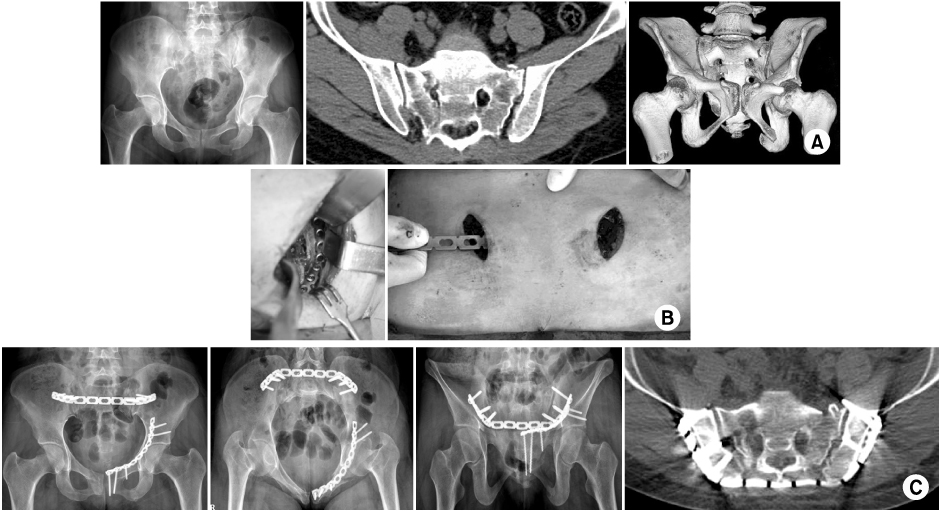
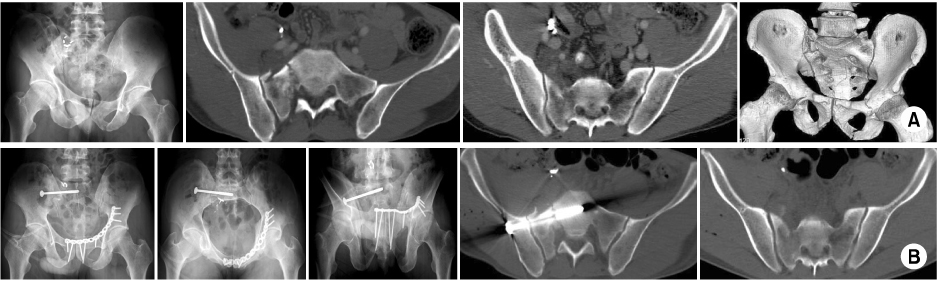
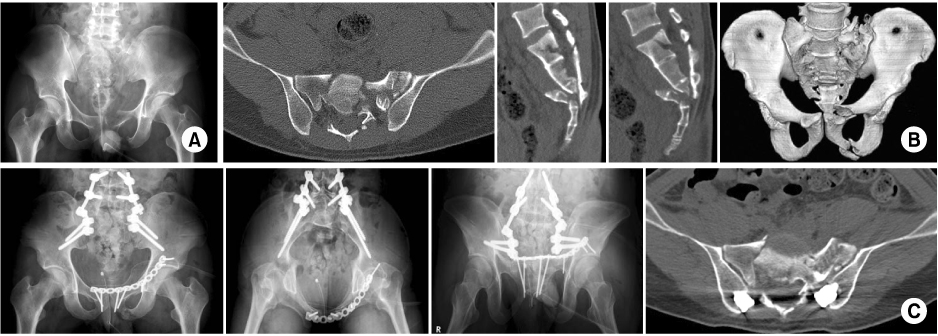
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Laminoplasty for Treatment of Transverse Sacral Fracture: A Case Report
Young Soo Jang, Jak Jang, Sung Ju Bae, Chan Il Bae, Sung Bae Park
Journal of the Korean Fracture Society.2014; 27(2): 157. CrossRef
 Cite
CiteSacral Fractures

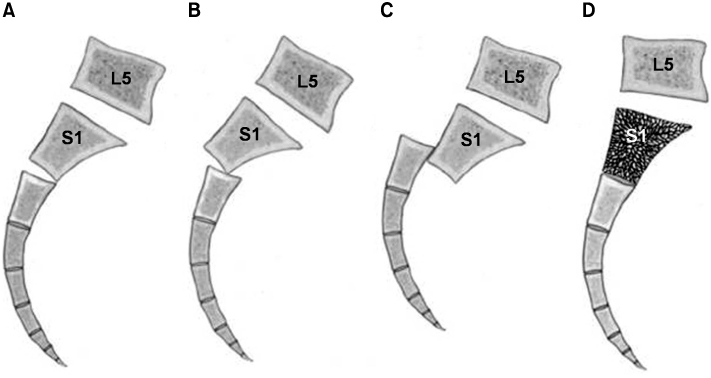
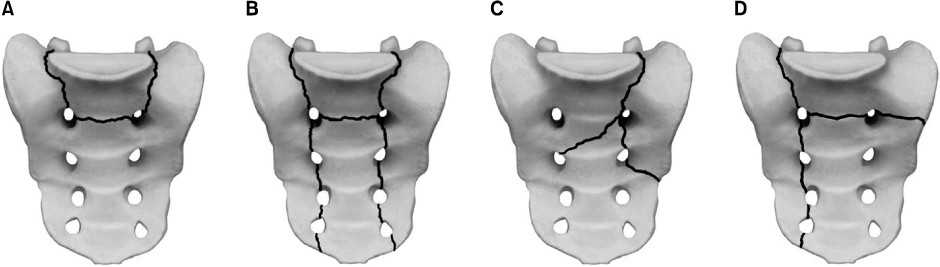
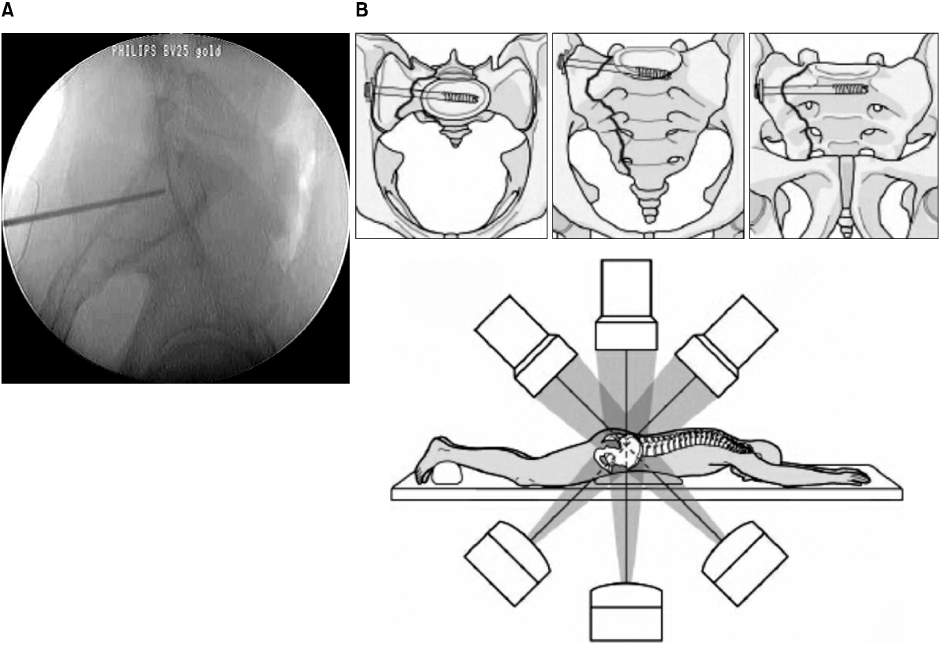
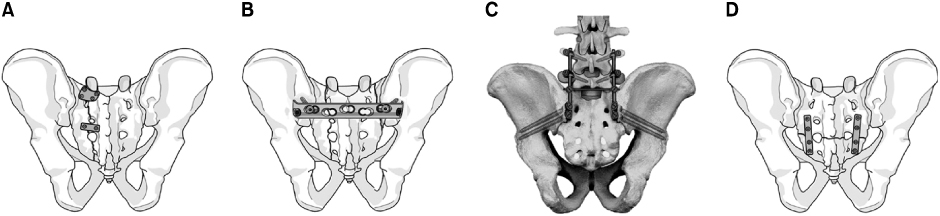
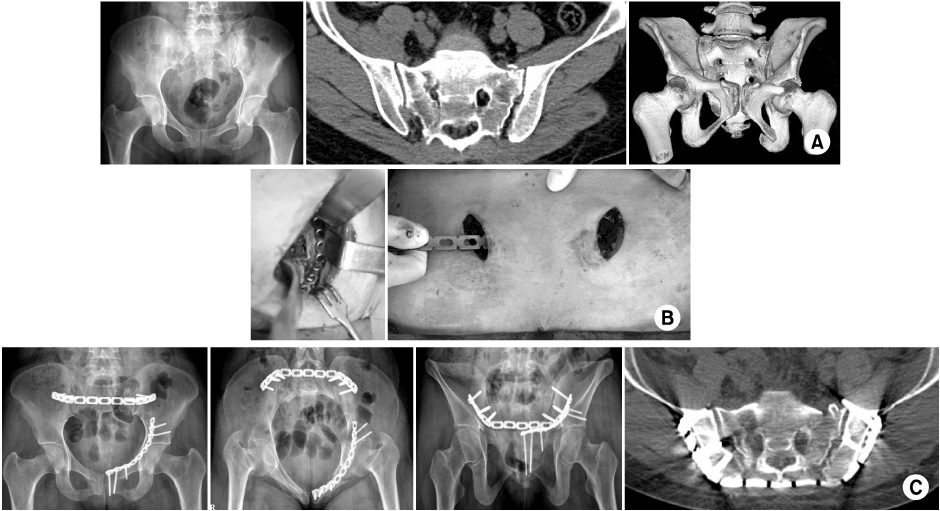
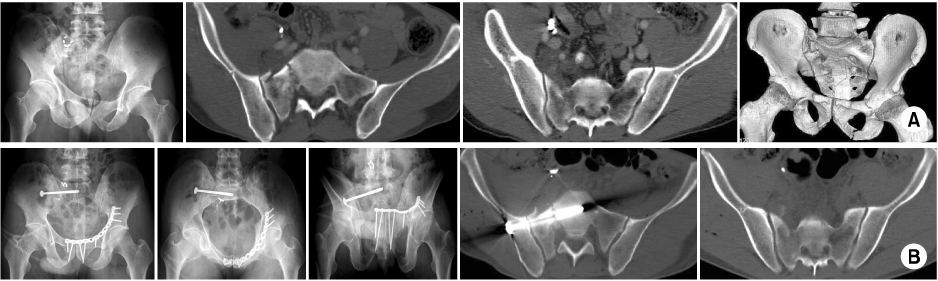
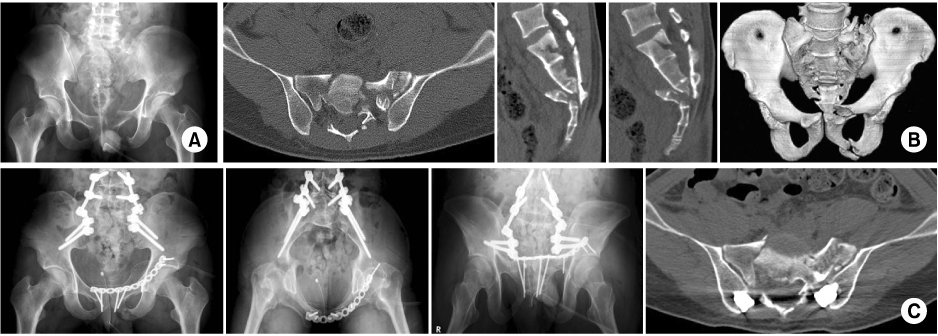
Fig. 1
Classification of sacral fractures according to Denis et al. Zone I is lateral to the neuroforamina (transalar fracture). Zone II involves the neuroforamina, but does not involve the spinal canal (transforaminal fracture). Zone III extends into the spinal canal with primary or associated fracture lines (central fracture).
Fig. 2
Subclassification of Denis zone III sacral fractures, as described by Roy-Camille et al and modified by Strange-Vognsen and Lebech.
(A) Type 1, flexion fracture with an anterior simple bending of the upper fragment.
(B) Type 2, flexion fracture with a posterior displacement of the upper fragment.
(C) Type 3, extension fracture with an anterior displacement of the upper fragment more and less vertical.
(D) Type 4, neutral position fracture with marked comminution and nondisplacement of the upper fragment.
Fig. 3
Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet.
(A) U-type fracture.
(B) H-type fracture.
(C) λ-type (or Y-type) fracture.
(D) T-type fracture.
Fig. 4
Percutaneous fixation of the iliosacral screw.
(A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop).
(B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet, A-P and outlet views of the pelvis.
Fig. 5
Methods of surgical stabilization.
(A) Local plate osteosynthesis.
(B) Posterior transiliac plate fixation.
(C) Spino-pelvic fixation.
(D) Plate stabilization for the low transverse fracture.
Fig. 6
This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident.
(A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum.
(B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma.
(C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures.
Fig. 7
This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb.
(A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type).
(B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a reconstruction plate anteriorly and an iliosacral screw posteriorly. Note: The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw.
Fig. 8
This 23-year-old male patient sustained polytrauma including a suicidal jumper's fracture by a fall from the 5th story.
(A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture.
(B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures.
(C) Definitive treatment was performed 11 days after trauma. Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Sacral Fractures

