 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(4); 2011 > Article
-
Review Article
- Sacral Fractures
- Young-Soo Byun, M.D., Se-Ang Chang, M.D.
-
Journal of the Korean Fracture Society 2011;24(4):371-381.
DOI: https://doi.org/10.12671/jkfs.2011.24.4.371
Published online: October 30, 2011
Department of Orthopedic Surgery, Daegu Fatima Hospital, Daegu, Korea.
- Address reprint requests to: Young-Soo Byun, M.D. Department of Orthopedic Surgery, Daegu Fatima Hospital, 576-31, Sinam-dong, Dong-gu, Daegu 701-600, Korea. Tel: 82-53-940-7320, Fax: 82-53-954-7417, fatimaos@unitel.co.kr
Copyright © 2011 The Korean Fracture Society
- 1,752 Views
- 24 Download
- 1 Crossref
- 1. Albert MJ, Miller ME, MacNaughton M, Hutton WC. 1) Posterior pelvic fixation using a transiliac 4.5-mm reconstruction plate: a clinical and biomechanical study. J Orthop Trauma, 1993;7:226-232.
- 2. Bents RT, France JC, Glover JM, Kaylor KL. Traumatic spondylopelvic dissociation. A case report and literature review. Spine (Phila Pa 1976), 1996;21:1814-1819.
- 3. Denis F, Davis S, Comfort T. Sacral fractures: an important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res, 1988;227:67-81.
- 4. Ebraheim NA, Coombs R, Hoeflinger MJ, Zeman C, Jackson WT. Anatomical and radiological considerations in compressive bar technique for posterior pelvic disruptions. J Orthop Trauma, 1991;5:434-438.
- 5. Edeiken-Monroe BS, Browner BD, Jackson H. The role of standard roentgenograms in the evaluation of instability of pelvic ring disruption. Clin Orthop Relat Res, 1989;(240):63-76.
- 6. Failinger MS, McGanity PL. Unstable fractures of the pelvic ring. J Bone Joint Surg Am, 1992;74:781-791.
- 7. Fountain SS, Hamilton RD, Jameson RM. Transverse fractures of the sacrum. A report of six cases. J Bone Joint Surg Am, 1977;59:486-489.
- 8. Gibbons KJ, Soloniuk DS, Razack N. Neurological injury and patterns of sacral fractures. J Neurosurg, 1990;72:889-893.
- 9. Gribnau AJ, van Hensbroek PB, Haverlag R, Ponsen KJ, Been HD, Goslings JC. U-shaped sacral and quality of life. Injury, 2009;40:1040-1048.
- 10. Hunt N, Jennings A, Smith M. Current management of U-shaped sacral fractures or spino-pelvic dissociation. Injury, 2002;33:123-126.
- 11. Jackson H, Kam J, Harris JH Jr, Harle TS. The sacral arcuate lines in upper sacral fractures. Radiology, 1982;145:35-39.
- 12. Kellam JF, McMurtry RY, Paley D, Tile M. The unstable pelvic fracture. Operative treatment. Orthop Clin North Am, 1987;18:25-41.
- 13. Kim MY, Reidy DP, Nolan PC, Finkelstein JA. Transverse sacral fractures: case series and literature review. Can J Surg, 2001;44:359-363.
- 14. Krappinger D, Larndorfer R, Struve P, Rosenberger R, Arora R, Blauth M. Minimally invasive transiliac plate osteosynthesis for type C injuries of the pelvic ring: a clinical and radiological follow-up. J Orthop Trauma, 2007;21:595-602.
- 15. Matta JM, Saucedo T. Internal fixation of pelvic ring fractures. Clin Orthop Relat Res, 1989;(242):83-97.
- 16. Mehta S, Auerbach JD, Born CT, Chin KR. Sacral fractures. J Am Acad Orthop Surg, 2006;14:656-665.
- 17. Mosheiff R, Liebergall M. Maneuvering the retrograde medullary screw in pubic ramus fractures. J Orthop Trauma, 2002;16:594-596.
- 18. Nork SE, Jones CB, Harding SP, Mirza SK, Routt ML Jr. Percutaneous stabilization of U-shaped sacral fractures using iliosacral screws: technique and early results. J Orthop Trauma, 2001;15:238-246.
- 19. Osterhoff G, Ossendorf C, Wanner GA, Simmen HP, Werner CM. Posterior screw fixation in rotationally unstable pelvic ring injuries. Injury, 2011;42:992-996.
- 20. Pohlemann T, Angst M, Schneider E, Ganz R, Tscherne H. Fixation of transforaminal sacrum fractures: a biomechanical study. J Orthop Trauma, 1993;7:107-117.
- 21. Riemer BL, Butterfield SL, Diamond DL, et al. Acute mortality associated with injuries to the pelvic ring: the role of early patient mobilization and external fixation. J Trauma, 1993;35:671-675.
- 22. Robles LA. Transverse sacral fractures. Spine J, 2009;9:60-69.
- 23. Rommens PM, Hessmann MH. Staged reconstruction of pelvic ring disruption: differences in morbidity, mortality, radiologic results, and functional outcomes between B1, B2/B3, and C-type lesions. J Orthop Trauma, 2002;16:92-98.
- 24. Rommens PM, Vanderschot PM, Broos PL. Conventional radiography and CT examination of pelvic ring fractures. A comparative study of 90 patients. Unfallchirurg, 1992;95:387-392.
- 25. Routt MLC Jr, Meier MC, Kregor PJ, et al. Percutaneous iliosacral screws with the patient supine. Oper Tech Orthop, 1993;7:35-45.
- 26. Routt MLC Jr, Simonian PT, Grujic L. The retrograde medullary superior pubic ramus screw for the treatment of anterior pelvic ring disruptions: a new technique. J Orthop Trauma, 1995;9:35-44.
- 27. Routt MLC Jr, Simonian PT, Mills WJ. Iliosacral screw fixation: early complications of the percutaneous technique. J Orthop Trauma, 1997;11:584-589.
- 28. Routt MLC Jr, Simonian PT, Swiontkowski MF. Stabilization of pelvic ring disruptions. Orthop Clin North Am, 1997;28:369-388.
- 29. Roy-Camille R, Saillant G, Gagna G, Mazel C. Transverse fracture of the upper sacrum. Suicidal jumper's fracture. Spine (Phila Pa 1976), 1985;10:838-845.
- 30. Sagi HC. Technical aspects and recommended treatment algorithms in triangular osteosynthesis and spinopelvic fixation for vertical shear transforaminal sacral fractures. J Orthop Trauma, 2009;23:354-360.
- 31. Sagi HC, Militano U, Caron T, Lindvall E. A comprehensive analysis with minimum 1-year follow-up of vertically unstable transforaminal sacral fractures treated with triangular osteosynthesis. J Orthop Trauma, 2009;23:313-319.
- 32. Schildhauer TA, Bellabarba C, Nork SE, Barei DP, Routt ML Jr, Chapman JR. Decompression and lumbopelvic fixation for sacral fracture-dislocations with spino-pelvic dissociation. J Orthop Trauma, 2006;20:447-457.
- 33. Schildhauer TA, Josten C, Muhr G. Triangular osteosynthesis of vertically unstable sacrum fractures: a new concept allowing early weight-bearing. J Orthop Trauma, 1998;12:307-314.
- 34. Schildhauer TA, Ledoux WR, Chapman JR, Henley MB, Tencer AF, Routt ML Jr. Triangular osteosynthesis and iliosacral screw fixation for unstable sacral fractures: a cadaveric and biomechanical evaluation under cyclic loads. J Orthop Trauma, 2003;17:22-31.
- 35. Schmidek HH, Smith DA, Kristiansen TK. Sacral fractures. Neurosurgery, 1984;15:735-746.
- 36. Shaw JA, Mino DE, Werner FW, Murray DG. Posterior stabilization of pelvic fractures by use of threaded compression rods. Case reports and mechanical testing. Clin Orthop Relat Res, 1985;(192):240-254.
- 37. Siebler JC, Hasley BP, Mormino MA. Functional outcomes of Denis zone III sacral fractures treated nonoperatively. J Orthop Trauma, 2010;24:297-302.
- 38. Simonian PT, Routt ML Jr. Biomechanics of pelvic fixation. Orthop Clin North Am, 1997;28:351-367.
- 39. Starr AJ, Malekzadeh AS. Bucholz RW, Heckman JD, Court-Brown C. Fractures of the pelvic ring. In: Rockwood and Green's Fractures in adults, 2006;6th ed. Philadelphia, Lippincott Williams & Wilkins. 1585-1664.
- 40. Stocks GW, Gabel GT, Noble PC, Hanson GW, Tullos HS. Anterior and posterior internal fixation of vertical shear fractures of the pelvis. J Orthop Res, 1991;9:237-245.
- 41. Strange-Vognsen HH, Lebech A. An unusual type of fracture in the upper sacrum. J Orthop Trauma, 1991;5:200-203.
- 42. Suzuki T, Hak DJ, Ziran BH, et al. Outcome and complications of posterior transiliac plating for vertically unstable sacral fractures. Injury, 2009;40:405-409.
- 43. Tile M, Helfet DL, Kellam JF. Fractures of the pelvis and acetabulum, 2003;3rd ed. Philadelphia, USA, Lippincott Williams and Wilkins. 203-322.
- 44. Vaccaro AR, Kim DH, Brodke DS, et al. Diagnosis and management of sacral spine fractures. Instr Course Lect, 2004;53:375-385.
- 45. Vresilovic EJ, Mehta S, Placide R, Milam RA 4th. Traumatic spondylopelvic dissociation. A report of two cases. J Bone Joint Surg Am, 2005;87:1098-1103.
- 46. Ward EF, Tomasin J, Vander Griend RA. Open reduction and internal fixation of vertical shear pelvic fractures. J Trauma, 1987;27:291-295.
- 47. White JH, Hague C, Nicolaou S, Gee R, Marchinkow LO, Munk PL. Imaging of sacral fractures. Clin Radiol, 2003;58:914-921.
- 48. Yi C, Hak DJ. Traumatic spinopelvic dissociation or U-shaped sacral fracture: a review of the literature. Injury, 2011;In press.
REFERENCES
Fig. 1Classification of sacral fractures according to Denis et al. Zone I is lateral to the neuroforamina (transalar fracture). Zone II involves the neuroforamina, but does not involve the spinal canal (transforaminal fracture). Zone III extends into the spinal canal with primary or associated fracture lines (central fracture).

Fig. 2
Subclassification of Denis zone III sacral fractures, as described by Roy-Camille et al and modified by Strange-Vognsen and Lebech.
(A) Type 1, flexion fracture with an anterior simple bending of the upper fragment.
(B) Type 2, flexion fracture with a posterior displacement of the upper fragment.
(C) Type 3, extension fracture with an anterior displacement of the upper fragment more and less vertical.
(D) Type 4, neutral position fracture with marked comminution and nondisplacement of the upper fragment.
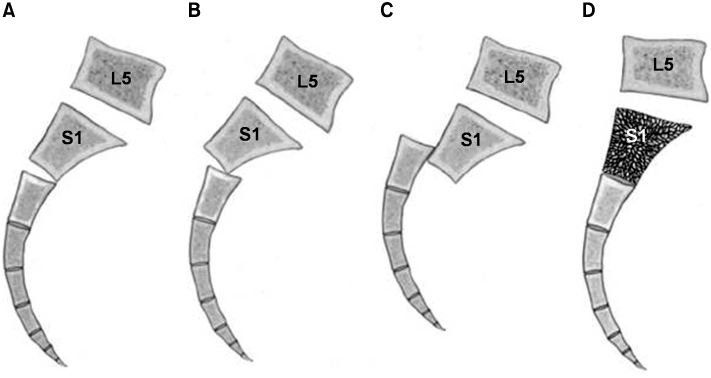
Fig. 3
Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet.
(A) U-type fracture.
(B) H-type fracture.
(C) λ-type (or Y-type) fracture.
(D) T-type fracture.
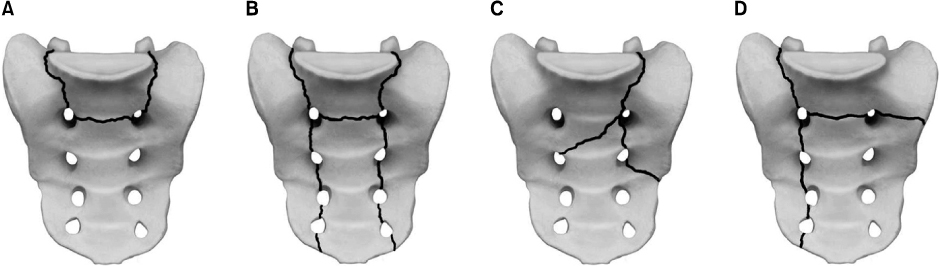
Fig. 4
Percutaneous fixation of the iliosacral screw.
(A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop).
(B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet, A-P and outlet views of the pelvis.
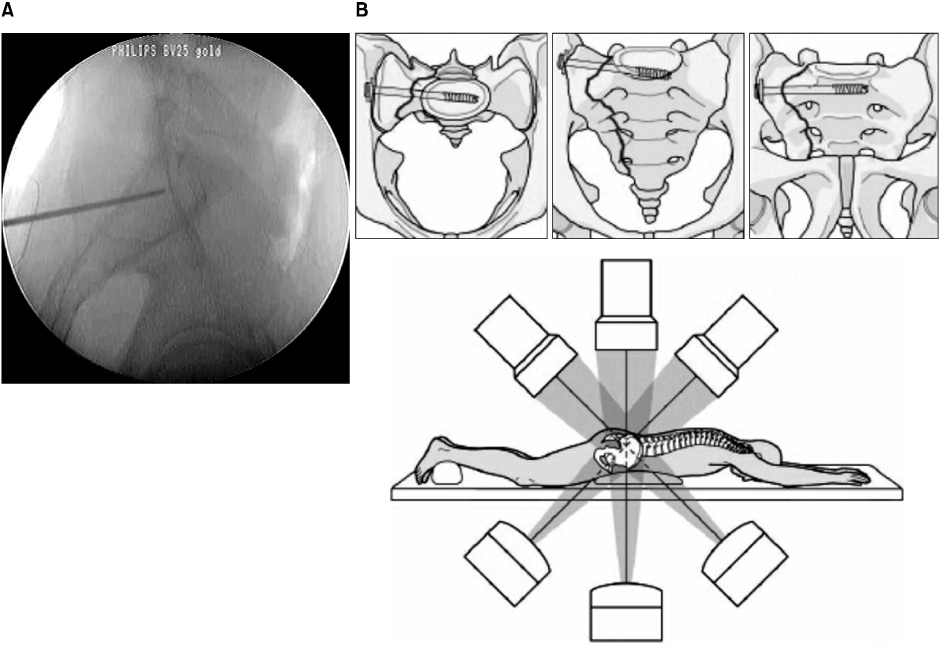
Fig. 5
Methods of surgical stabilization.
(A) Local plate osteosynthesis.
(B) Posterior transiliac plate fixation.
(C) Spino-pelvic fixation.
(D) Plate stabilization for the low transverse fracture.
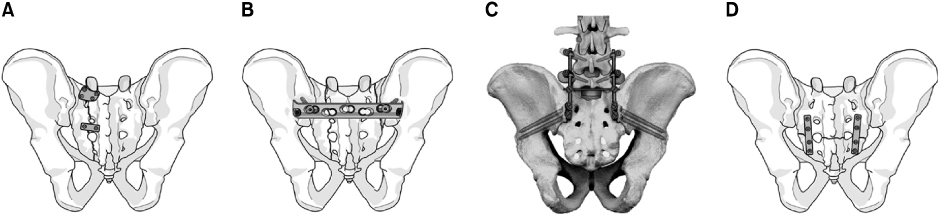
Fig. 6
This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident.
(A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum.
(B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma.
(C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures.
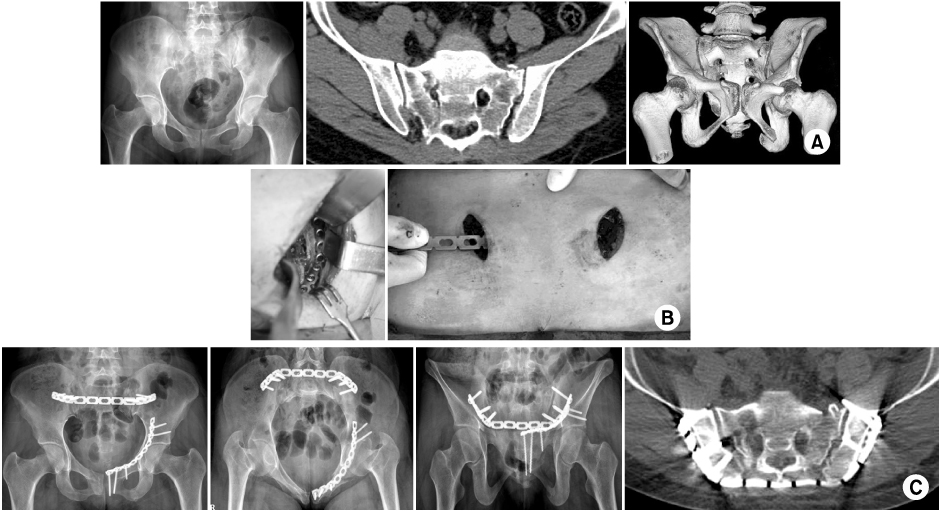
Fig. 7
This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb.
(A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type).
(B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a reconstruction plate anteriorly and an iliosacral screw posteriorly. Note: The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw.
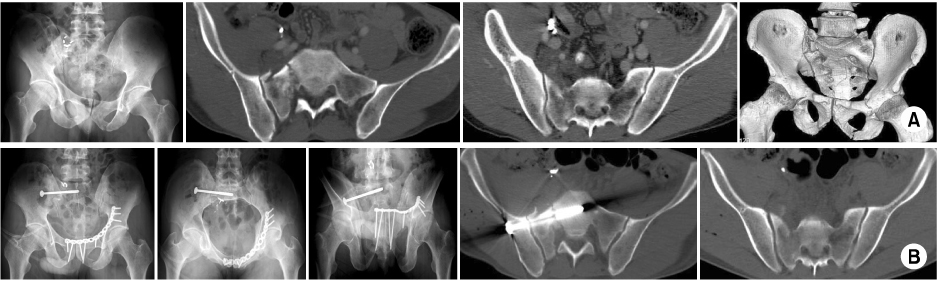
Fig. 8
This 23-year-old male patient sustained polytrauma including a suicidal jumper's fracture by a fall from the 5th story.
(A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture.
(B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures.
(C) Definitive treatment was performed 11 days after trauma. Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation.
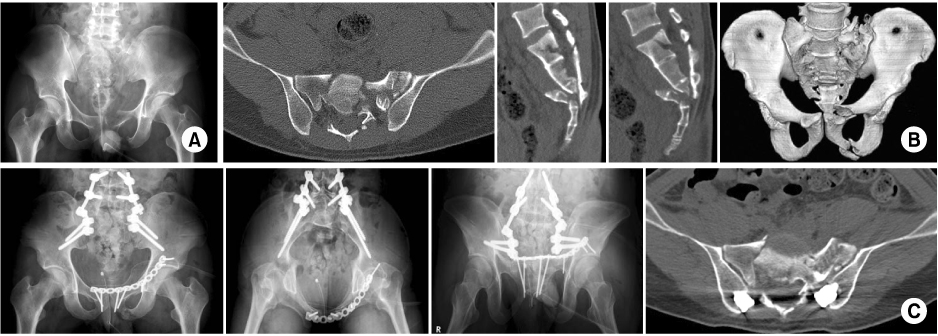
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Laminoplasty for Treatment of Transverse Sacral Fracture: A Case Report
Young Soo Jang, Jak Jang, Sung Ju Bae, Chan Il Bae, Sung Bae Park
Journal of the Korean Fracture Society.2014; 27(2): 157. CrossRef
 Cite
CiteSacral Fractures

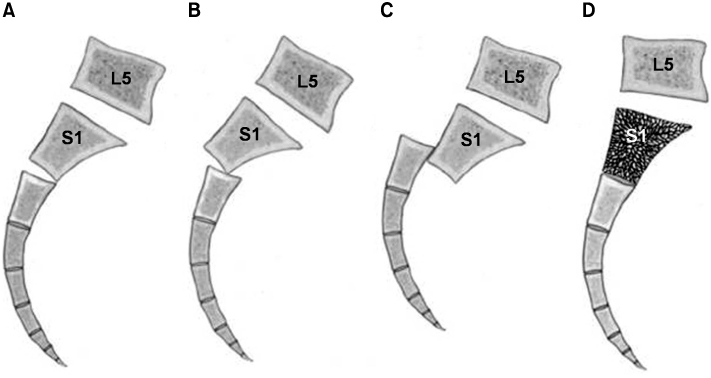
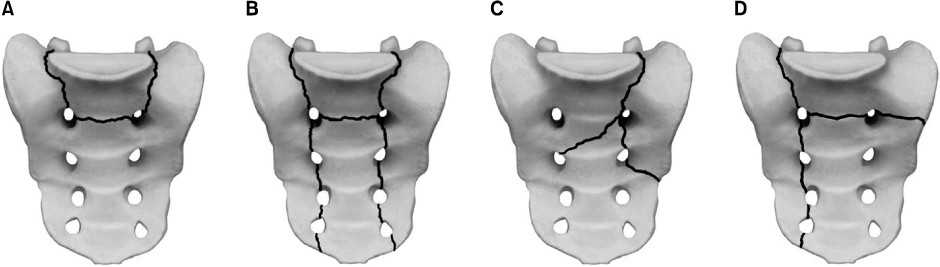
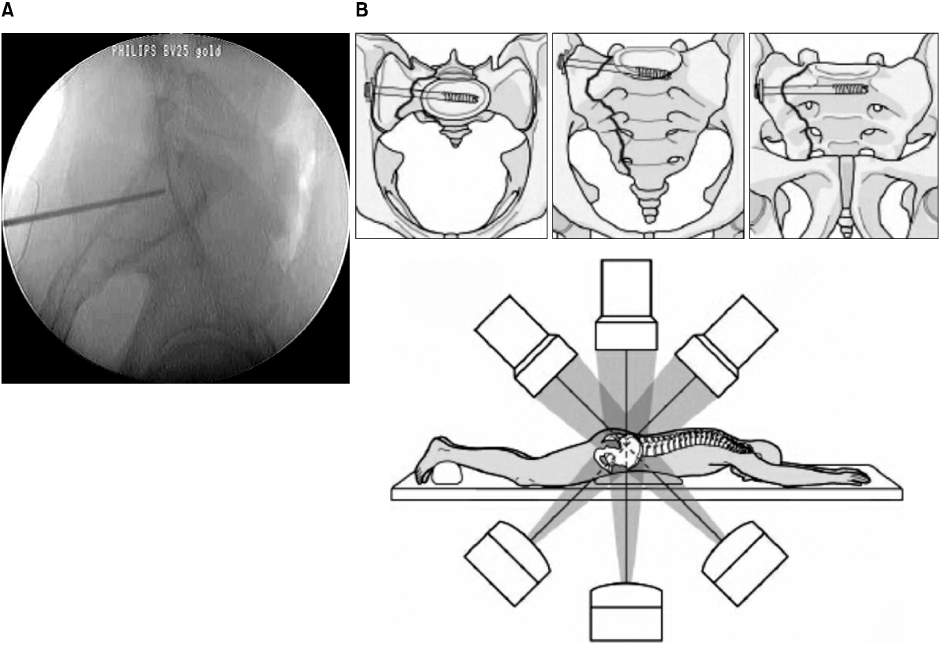
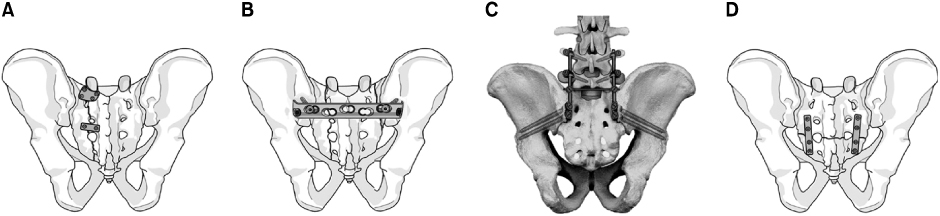
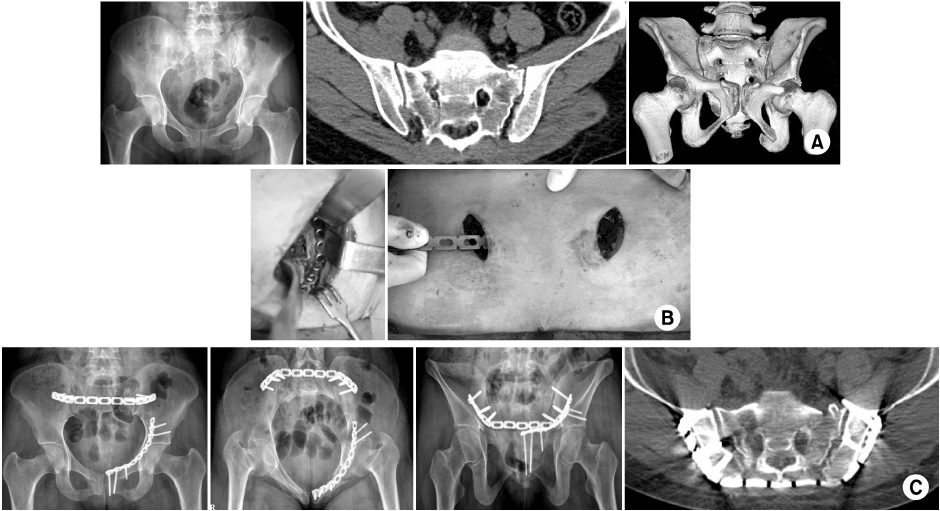
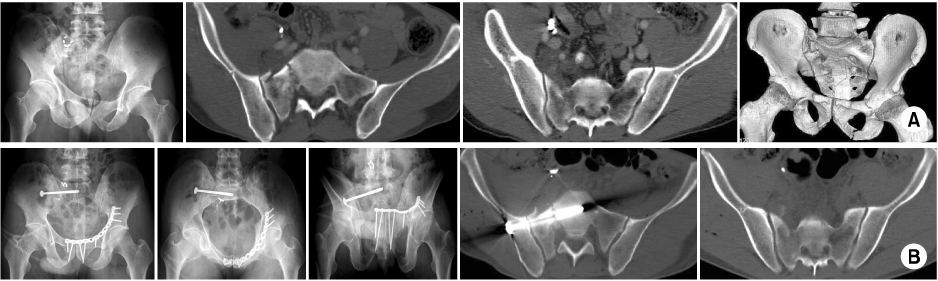
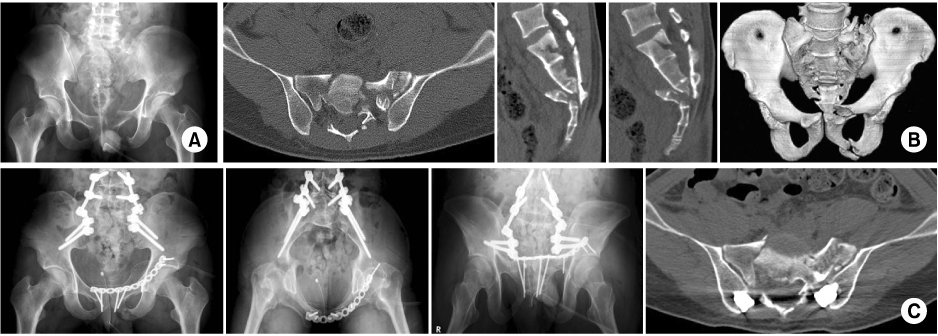
Fig. 1
Classification of sacral fractures according to Denis et al. Zone I is lateral to the neuroforamina (transalar fracture). Zone II involves the neuroforamina, but does not involve the spinal canal (transforaminal fracture). Zone III extends into the spinal canal with primary or associated fracture lines (central fracture).
Fig. 2
Subclassification of Denis zone III sacral fractures, as described by Roy-Camille et al and modified by Strange-Vognsen and Lebech.
(A) Type 1, flexion fracture with an anterior simple bending of the upper fragment.
(B) Type 2, flexion fracture with a posterior displacement of the upper fragment.
(C) Type 3, extension fracture with an anterior displacement of the upper fragment more and less vertical.
(D) Type 4, neutral position fracture with marked comminution and nondisplacement of the upper fragment.
Fig. 3
Complex Denis zone III sacral fractures can be classified descriptively by the letter of the alphabet.
(A) U-type fracture.
(B) H-type fracture.
(C) λ-type (or Y-type) fracture.
(D) T-type fracture.
Fig. 4
Percutaneous fixation of the iliosacral screw.
(A) The tip of the guidewire should be placed distal to the iliac cortical density (the sacral alar slop).
(B) The C-arm must be positioned to allow standard fluoroscopic views such as inlet, A-P and outlet views of the pelvis.
Fig. 5
Methods of surgical stabilization.
(A) Local plate osteosynthesis.
(B) Posterior transiliac plate fixation.
(C) Spino-pelvic fixation.
(D) Plate stabilization for the low transverse fracture.
Fig. 6
This 29-year-old female patient sustained pelvic ring injury with incomplete neurologic deficit by a motor vehicle accident.
(A) The initial x-ray and CT scan show the left pubic rami fractures and bilateral transforaminal fractures of the sacrum with dysmorphism of the upper sacrum.
(B) The left pubic rami fractures were reduced and stabilized with a plate through a modified Stoppa approach and the sacral fracture was stabilized with a transiliac plate through two short incisions 4 days after trauma.
(C) Postoperative x-rays and CT scan show good reduction and stable fixation of the fractures.
Fig. 7
This 49-year-old male patient sustained pelvic ring injury by lateral compression force with minimal neurologic deficit of the right lower limb.
(A) Initial x-ray and CT scan show the left pubic rami fractures and the right vertical sacral fracture (Bucket-handle type).
(B) Postoperative x-rays and CT scan show reduction of the pelvic deformity and stabilization of the pelvis with a reconstruction plate anteriorly and an iliosacral screw posteriorly. Note: The sacral fracture was reduced indirectly by reduction of the anterior pubic rami fractures and stabilized by a percutaneous iliosacral screw.
Fig. 8
This 23-year-old male patient sustained polytrauma including a suicidal jumper's fracture by a fall from the 5th story.
(A) The initial A-P view shows displaced fractures of the left pubic rami and suspicious complex sacral fracture.
(B) Preoperative CT scan shows complex transverse and longitudinal sacral fractures.
(C) Definitive treatment was performed 11 days after trauma. Postoperative x-rays and CT scan show fracture reduction and lumbo-pelvic fixation.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Sacral Fractures

