 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(1); 2011 > Article
-
Original Article
- The Surgical Outcomes of Clavicle Lateral End Fractures Fixed with the Oblique T Locking Compession Plate
- Seung-Oh Nam, M.D., Young-Soo Byun, M.D., Dong-Ju Shin, M.D., Jung-Hoon Shin, M.D., Chung-Yeol Lee, M.D., Tae-Gyun Kim, M.D.
-
Journal of the Korean Fracture Society 2011;24(1):41-47.
DOI: https://doi.org/10.12671/jkfs.2011.24.1.41
Published online: January 19, 2011
Department of Orthopedic Surgery, Daegu Fatima Hospital, Daegu, Korea.
- Address reprint requests to: Young-Soo Byun, M.D. Department of Orthopaedic Surgery, Daegu Fatima Hospital, 576-31, Sinam-dong, Dong-gu, Daegu 701-600, Korea. Tel: 82-53-940-7320·Fax: 82-53-940-7417, fatimaos@unitel.co.kr
• Received: September 7, 2010 • Revised: October 26, 2010 • Accepted: December 1, 2010
Copyright © 2011 The Korean Fracture Society
- 1,018 Views
- 1 Download
- 1 Crossref
Abstract
-
Purpose
- The purpose of this study is to evaluate the surgical outcomes of the clavicle lateral end fracture fixed with an oblique T locking compression plate (LCP).
-
Materials and Methods
- Fourteen clavicle lateral end fractures were fixed with the oblique T-LCP and followed up for at least 1 year after the surgery. Thirteen cases were unstable Neer type II fractures and one case was nonunion of the Neer type I fracture. The mean age was 46 years of age (range, 26~70). In ten cases, augmenting sutures with the absorbable suture material were placed in the coraco-clavicular ligament and around the plate and the clavicle to improve the stability of fracture fixation. Autogenous iliac bone graft was done in four cases. The clinical outcomes were evaluated by using UCLA scoring system and KSS (Korean Shoulder Score).
-
Results
- The mean UCLA score was 33.5 and the mean KSS was 94.9. Average time of bone union was 11.9 weeks (range, 6~28), including 1 case with a delayed union. There was no complication such as loss of fixation or nonunion.
-
Conclusion
- Fixation with the oblique T-LCP is a good option providing reliable functional results in clavicle lateral end fractures.
- 1. Ahn BW, Yoon JH, Kim CK, et al. Internal fixation of clavicle lateral and fracture with mini T-plate. J Korean Fract Soc, 2005;18:410-414.Article
- 2. Allman FL Jr. Fractures and ligamentous injuries of the clavicle and its articulation. J Bone Joint Surg Am, 1967;49:774-784.Article
- 3. Chun JM, Kim SY, Lee KW, Shin SJ, Kim EG. Modified tenson band fixation for unstable fracture of the distal clavicle. J Korean Orthop Assoc, 2002;37:416-420.ArticlePDF
- 4. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res, 1987;214:160-164.Article
- 5. Craig EV. Rockwood CA, Green DP, Bucholz RW, Heckman JD. Fracture of the clavicle. In: Fractures in adults, 1996;4th ed. Philadelphia, Lippincott-Raven. 1109-1161.
- 6. Edwards DJ, Kavanagh TG, Flannery MC. Fractures of the distal clavicle: a case for fixation. Injury, 1992;23:44-46.Article
- 7. Flinkkilä T, Ristiniemi J, Hyvönen P, Hämäläinen M. Surgical treatment of unstable fractures of the distal clavicle: a comparative study of Kirschner wire and clavicular hook plate fixation. Acta Orthop Scand, 2002;73:50-53.Article
- 8. Goldberg JA, Bruce WJ, Sonnabend DH, Walsh WR. Type 2 fractures of the distal clavicle: a new surgical technique. J Shoulder Elbow Surg, 1997;6:380-382.Article
- 9. Hessmann M, Kirchner R, Baumgaertel F, Gehling H, Gotzen L. Treatment of unstable distal clavicular fractures with and without lesions of the acromioclavicular joint. Injury, 1996;27:47-52.Article
- 10. Kang HJ, Park KK, Yoon HK, Song HK, Hahn SB. T plate fixation for unstable fracture of distal clavicle. J Korean Fract Soc, 2006;19:329-334.Article
- 11. Kao FC, Chao EK, Chen CH, Yu SW, Chen CY, Yen CY. Treatment of distal clavicle fracture using Kirschner wires and tension-band wires. J Trauma, 2001;51:522-525.Article
- 12. Kona J, Bosse MJ, Staeheli JW, Rosseau RL. Type II distal clavicle fractures: a retrospective review of surgical treatment. J Orthop Trauma, 1990;4:115-120.
- 13. Lee KJ, Choi CH, Kim JM, et al. The Shoulder and elbow, 2007;1st ed. Seoul, Korea, Young-Chang. 290-291.
- 14. Lee KJ, Choi CH, Kim JM, et al. The Shoulder and elbow, 2007;1st ed. Seoul, Korea, Young-Chang. 676-679.
- 15. Neer CS 2nd. Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma, 1963;3:99-110.Article
- 16. Neviaser RJ, Neviaser JS, Neviaser TJ, Neviaser JS. A simple technique for internal fixation of the clavicle. A long term evaluation. Clin Orthop Relat Res, 1975;109:103-107.
- 17. Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta Orthop Scand, 1993;64:87-91.Article
- 18. Robinson CM, Cairns DA. Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am, 2004;86:778-782.Article
- 19. Shin SI, Song KW, Lee JY, et al. Treatment of type 2 distal clavicle fracture using wolter plate. J Korean Shoulder Elbow Soc, 2009;12:14-20.Article
- 20. Sim E, Schwarz N, Höcker K, Berzlanovich A. Repair of complete acromioclavicular separations using the acromioclavicular-hook plate. Clin Orthop Relat Res, 1995;314:134-142.Article
- 21. Yamaguchi H, Arakawa H, Kobayashi M. Results of the bosworth method for unstable fractures of the distal clavicle. Int Orthop, 1998;22:366-368.ArticlePDF
REFERENCES
Fig. 1
(A~C) Oblique T Locking Compression Plate is appropriate for fixation of clavicle lateral end fracture.
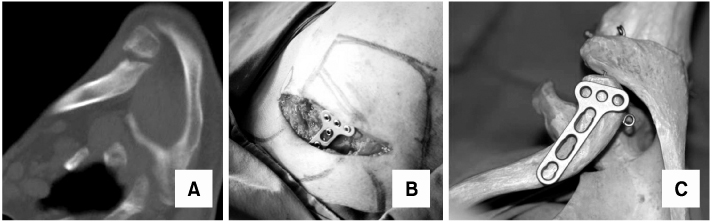
Fig. 2
Intraoperative photographs.
(A) Patient was placed Beach chair position.
(B) The direct approach with Langer's line was used for exposure.
(C) Acromio-clavicular joint was marked with a needle (circle).
(D) The Needle of acromio-clavicular joint was seen on fluoroscopic view (circle).
(E, F) The Needle makes plate positioning easy. Plate was fixed with screws.
(G, H) After screw fixation, unstable fragment that coraco-clavicular ligament was attached was coiled with absorbable suture material through coraco-clavicular ligament.
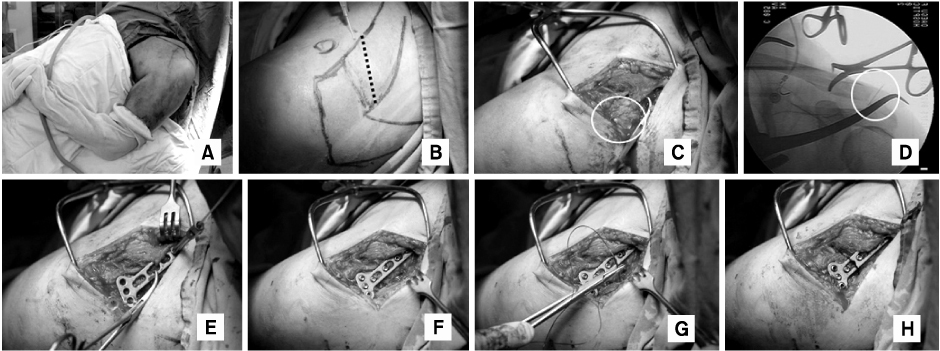
Fig. 3
A 47-year-old man sustained a clavicle lateral end fracture by a traffic accident.
(A, B) Preoperative radiographs show Neer type II, Craig type V unstable clavicle lateral end fracture.
(C, D) Satisfactory reduction and fixation was seen on postoperative radiographs.
(E, F) Radiographs 4 weeks after operation show bone absorption.
(G, H) Final radiographs 57 weeks after operation show solid union without implant loosening and loss of reduction.
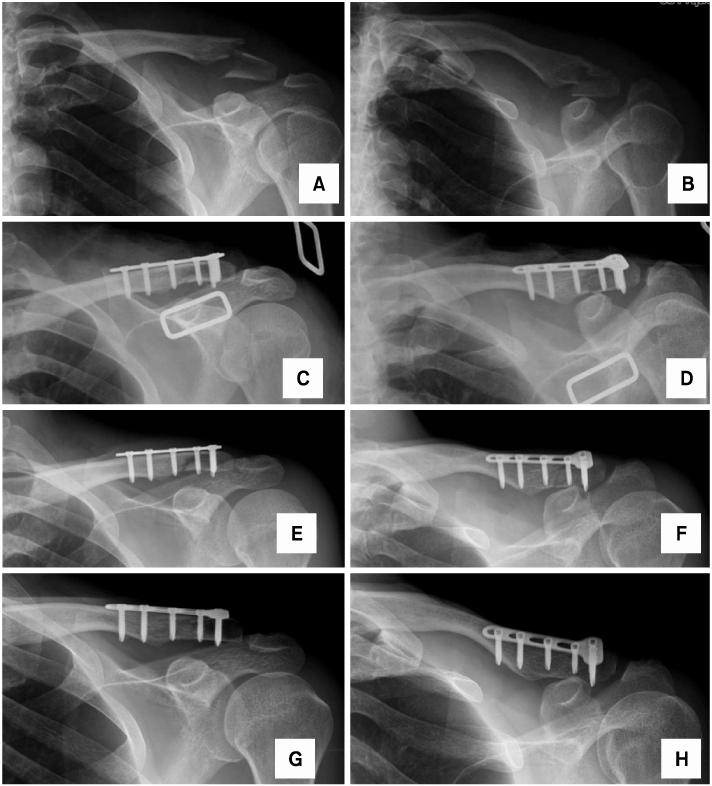
Fig. 4
A 39-year-old man sustained a clavicle lateral end fracture by a traffic accident.
(A~C) Reconstructed three-dimensional CT scans show a comminuted, unstable fracture of clavicle lateral end.
(D, E) Preoperative radiographs show Neer type II, Craig type V clavicle lateral end fracture
(F, G) Final radiographs 2 years after operation show solid union without implant loosening and loss of reduction.
(H~L) The photographs show a good functional result with full forward flexion and internal and external rotation of shoulders at final follow-up (postoperative 2 years).
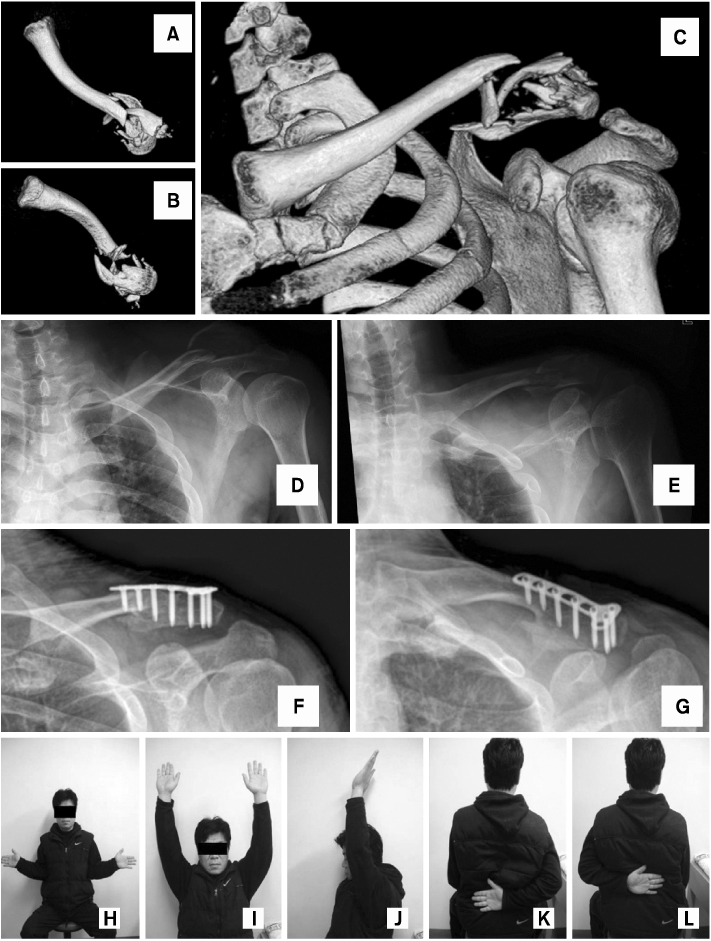
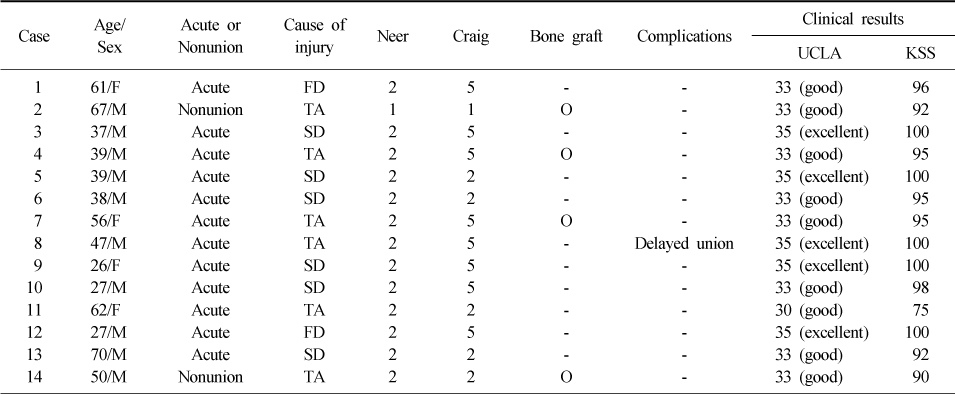
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Results of Hook Plate Fixation of Unstable Distal Clavicle Fractures
Hoon-Sang Sohn, Byung Chul Jo
Journal of the Korean Fracture Society.2011; 24(4): 335. CrossRef
 Cite
CiteThe Surgical Outcomes of Clavicle Lateral End Fractures Fixed with the Oblique T Locking Compession Plate
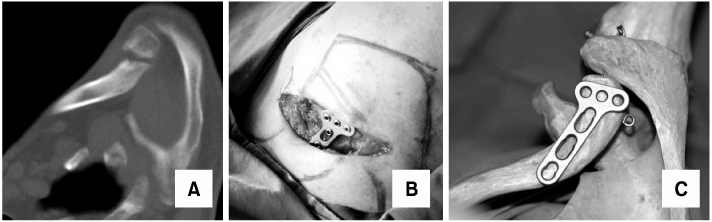
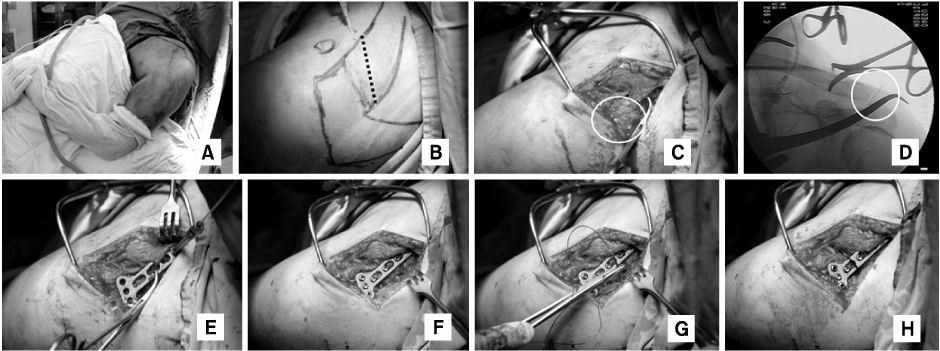
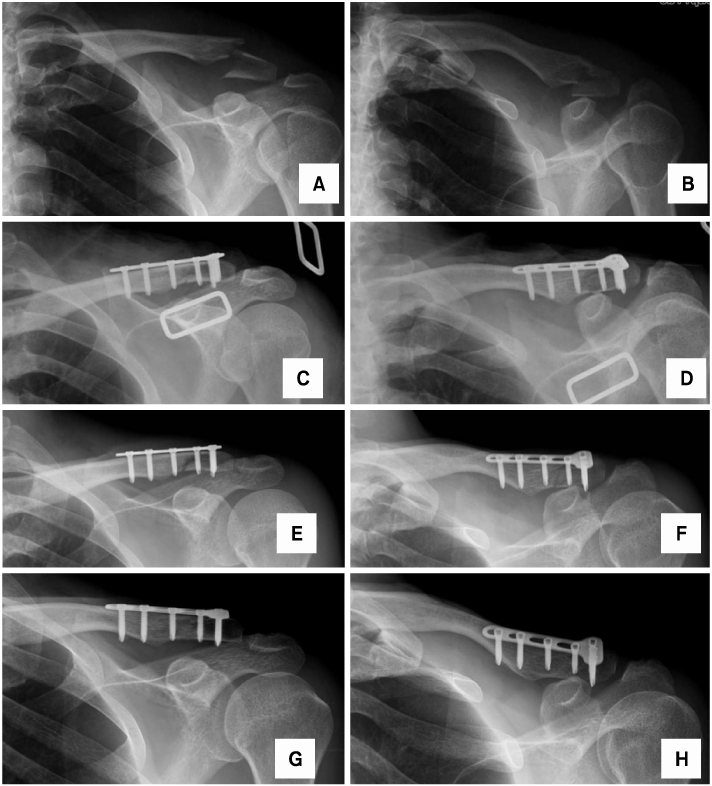
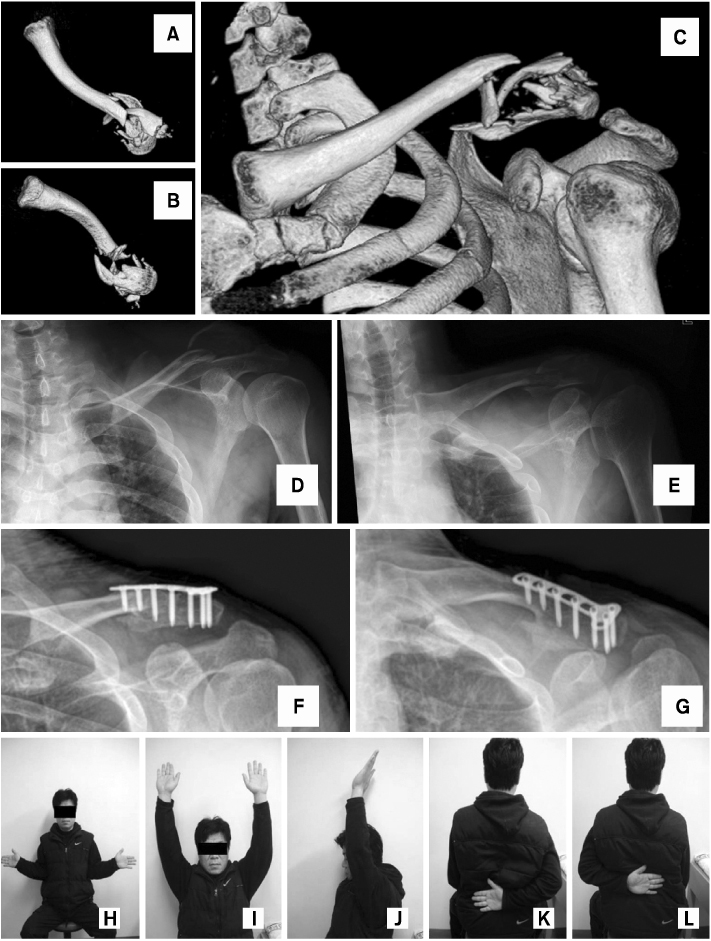
Fig. 1
(A~C) Oblique T Locking Compression Plate is appropriate for fixation of clavicle lateral end fracture.
Fig. 2
Intraoperative photographs.
(A) Patient was placed Beach chair position.
(B) The direct approach with Langer's line was used for exposure.
(C) Acromio-clavicular joint was marked with a needle (circle).
(D) The Needle of acromio-clavicular joint was seen on fluoroscopic view (circle).
(E, F) The Needle makes plate positioning easy. Plate was fixed with screws.
(G, H) After screw fixation, unstable fragment that coraco-clavicular ligament was attached was coiled with absorbable suture material through coraco-clavicular ligament.
Fig. 3
A 47-year-old man sustained a clavicle lateral end fracture by a traffic accident.
(A, B) Preoperative radiographs show Neer type II, Craig type V unstable clavicle lateral end fracture.
(C, D) Satisfactory reduction and fixation was seen on postoperative radiographs.
(E, F) Radiographs 4 weeks after operation show bone absorption.
(G, H) Final radiographs 57 weeks after operation show solid union without implant loosening and loss of reduction.
Fig. 4
A 39-year-old man sustained a clavicle lateral end fracture by a traffic accident.
(A~C) Reconstructed three-dimensional CT scans show a comminuted, unstable fracture of clavicle lateral end.
(D, E) Preoperative radiographs show Neer type II, Craig type V clavicle lateral end fracture
(F, G) Final radiographs 2 years after operation show solid union without implant loosening and loss of reduction.
(H~L) The photographs show a good functional result with full forward flexion and internal and external rotation of shoulders at final follow-up (postoperative 2 years).
Fig. 1
Fig. 2
Fig. 3
Fig. 4
The Surgical Outcomes of Clavicle Lateral End Fractures Fixed with the Oblique T Locking Compession Plate
Patient demographics
M: Male, F: Female, TA: Traffic accident, SD: Slip down, FD: Fall down.
Table 1
Patient demographics
M: Male, F: Female, TA: Traffic accident, SD: Slip down, FD: Fall down.

