 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(4); 2011 > Article
-
Original Article
- Minimally Invasive Anterior Plating of Humeral Shaft Fractures
- Hyun-Joo Lee, M.D., Chang-Wug Oh, M.D., Do-Hyung Kim, M.D., Kyung-Hyun Park, M.D.
-
Journal of the Korean Fracture Society 2011;24(4):341-346.
DOI: https://doi.org/10.12671/jkfs.2011.24.4.341
Published online: October 30, 2011
Department of Orthopaedic Surgery, Kyungpook National University Hospital, Deagu, Korea.
- Address reprint requests to: Chang-Wug Oh, M.D. Department of Orthopaedic Surgery, Kyungpook National University Hospital, 130, Dongdeok-ro, Jung-gu, Deagu 700-721, Korea. Tel: 82-53-420-5630, Fax: 82-53-422-6605, cwoh@knu.ac.kr
• Received: February 12, 2011 • Revised: July 18, 2011 • Accepted: September 2, 2011
Copyright © 2011 The Korean Fracture Society
- 1,296 Views
- 22 Download
- 3 Crossref
Abstract
-
Purpose
- We evaluated the efficacy and results of minimally invasive anterior plating for humeral shaft fracture.
-
Materials and Methods
- Twenty-two cases of humeral shaft fracture were reviewed, including 8 cases of type A, 8 of type B and 6 of type C (AO/OTA classification). There were three open fractures. The fracture was fixed with MIPO (minimally invasive plate osteosynthesis) technique under C-arm guide. A locking compression plate was located in anterior aspect of the humerus with at least three screws fixed in each fragment. Radiologic and functional results were evaluated.
-
Results
- In 20 of 22 cases, bony union was achieved with the mean period of 17.5 weeks, including 2 cases of delayed union. There were 2 cases of nonunion, which needed the further operative procedure. Except one case of distal 1/3 fracture, all cases showed satisfactory elbow and shoulder function with the mean Mayo elbow score of 17.4 and mean UCLA shoulder score of 97.3. In complication, there was one case of radial nerve palsy due to improper traction, but it was completely improved after 3 months. Otherwise, there was no complication including infection.
-
Conclusion
- Anterior MIPO for humeral shaft fracture may be another option of operative methods with high union and low complication rate.
- 1. Anglen JO, Archdeacon MT, Cannada LK, Herscovici D Jr, Ostrum RF. Avoiding complications in the treatment of humeral fractures. Instr Course Lect, 2009;58:3-11.
- 2. Apivatthakakul T, Arpornchayanon O, Bavornratanavech S. Minimally invasive plate osteosynthesis (MIPO) of the humeral shaft fracture. Is it possible? A cadaveric study and preliminary report. Injury, 2005;36:530-538.Article
- 3. Bell MJ, Beauchamp CG, Kellam JK, McMurtry RY. The results of plating humeral shaft fractures in patients with multiple injuries. The Sunnybrook experience. J Bone Joint Surg Br, 1985;67:293-296.ArticlePDF
- 4. Bhandari M, Devereaux PJ, McKee MD, Schemitsch EH. Compression plating versus intramedullary nailing of humeral shaft fractures--a meta-analysis. Acta Orthop, 2006;77:279-284.Article
- 5. Chapman JR, Henley MB, Agel J, Benca PJ. Randomized prospective study of humeral shaft fracture fixation: intramedullary nails versus plates. J Orthop Trauma, 2000;14:162-166.Article
- 6. Chen AL, Joseph TN, Wolinksy PR, et al. Fixation stability of comminuted humeral shaft fractures: locked intramedullary nailing versus plate fixation. J Trauma, 2002;53:733-737.Article
- 7. Dabezies EJ, Banta CJ 2nd, Murphy CP, d'Ambrosia RD. Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries. J Orthop Trauma, 1992;6:10-13.
- 8. Ekholm R, Ponzer S, Törnkvist H, Adami J, Tidermark J. The Holstein-Lewis humeral shaft fracture: aspects of radial nerve injury, primary treatment, and outcome. J Orthop Trauma, 2008;22:693-697.Article
- 9. Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am, 1986;68:1136-1144.Article
- 10. Fracture and dislocation compendium. Orthopaedic Trauma Association Committee for Coding and Classification. J Orthop Trauma, 1996;10:Suppl 1. v-ix. 1-154.
- 11. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am, 1976;58:453-458.
- 12. Heim D, Herkert F, Hess P, Regazzoni P. Surgical treatment of humeral shaft fractures--the Basel experience. J Trauma, 1993;35:226-232.Article
- 13. Hierholzer C, Sama D, Toro JB, Peterson M, Helfet DL. Plate fixation of ununited humeral shaft fractures: effect of type of bone graft on healing. J Bone Joint Surg Am, 2006;88:1442-1447.
- 14. Jawa A, McCarty P, Doornberg J, Harris M, Ring D. Extra-articular distal-third diaphyseal fractures of the humerus. A comparison of functional bracing and plate fixation. J Bone Joint Surg Am, 2006;88:2343-2347.
- 15. Ji F, Tong D, Tang H, et al. Minimally invasive percutaneous plate osteosynthesis (MIPPO) technique applied in the treatment of humeral shaft distal fractures through a lateral approach. Int Orthop, 2009;33:543-547.ArticlePDF
- 16. Jiang R, Luo CF, Zeng BF, Mei GH. Minimally invasive plating for complex humeral shaft fractures. Arch Orthop Trauma Surg, 2007;127:531-535.ArticlePDF
- 17. Lin J, Hou SM. Locked nailing of severely comminuted or segmental humeral fractures. Clin Orthop Relat Res, 2003;406:195-204.Article
- 18. Lin J, Shen PW, Hou SM. Complications of locked nailing in humeral shaft fractures. J Trauma, 2003;54:943-949.Article
- 19. Livani B, Belangero WD. Bridging plate osteosynthesis of humeral shaft fractures. Injury, 2004;35:587-595.Article
- 20. Livani B, Belangero WD, Castro de Medeiros R. Fractures of the distal third of the humerus with palsy of the radial nerve: management using minimally-invasive percutaneous plate osteosynthesis. J Bone Joint Surg Br, 2006;88:1625-1628.
- 21. McCormack RG, Brien D, Buckley RE, McKee MD, Powell J, Schemitsch EH. Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail. A prospective, randomised trialr. J Bone Joint Surg Br, 2000;82:336-339.
- 22. Morrey BF, Adams RA. Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Joint Surg Am, 1992;74:479-490.Article
- 23. Olarte CM, Darowish M, Ziran BH. Radial nerve transposition with humeral fracture fixation: preliminary results. Clin Orthop Relat Res, 2003;413:170-174.
- 24. Park JY, Oh JH, Kho DH, Jung JK. Intramedullary nail on the humeral fracture. J Korean Fract Soc, 2008;21:244-254.Article
- 25. Shao YC, Harwood P, Grotz MR, Limb D, Giannoudis PV. Radial nerve palsy associated with fractures of the shaft of the humerus: a systematic review. J Bone Joint Surg Br, 2005;87:1647-1652.
- 26. Shin HD, Rhee KJ, Kim KC, Song HS. Operative treatment of traumatic humeral shaft fracture: comparision of interlocking IM nailing and plate fixation by posterior approach. J Korean Fract Soc, 2005;18:93-99.Article
- 27. Volgas DA, Stannard JP, Alonso JE. Nonunions of the humerus. Clin Orthop Relat Res, 2004;419:46-50.Article
REFERENCES
Fig. 1
(A) A 47-year-old female sustained a spiral fracture of the left humerus diaphysis due to in-car accident.
(B, C) Through the submuscular tunnel, a locking compression plate was inserted and fixed with an acceptable alignment.
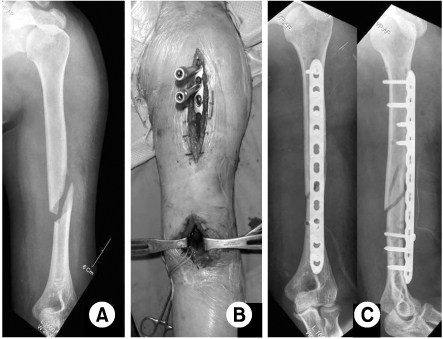
Fig. 2
(A) Ten months after the surgery, radiographs demonstrated a complete osseous union.
(B) Note the skin scars of proximal and distal incision without involving the fracture site.
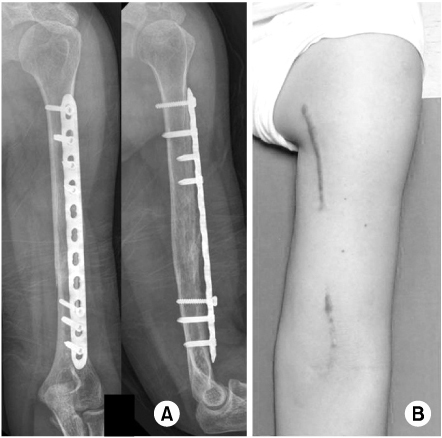
Fig. 3
(A) A 34-year-old female sustained a comminuted fracture of the humeral shaft after traffic accident.
(B) After making the submuscular tunnel using Kelly clamps, a locking compression plate was fixed with the MIPO procedure.
(C) Note an acceptable alignment without reducing the comminuted fragment.
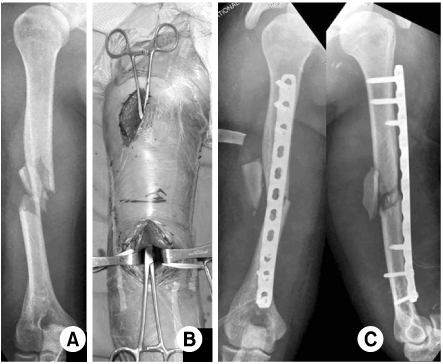
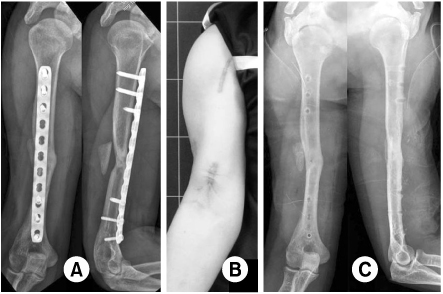
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Minimal Invasive Plate Osteosynthesis versus Conventional Open Plating in Simple Humeral Shaft Fracture (AO Type A, B1, B2)
Boseon Kim, GwangChul Lee, Hyunwoong Jang
Journal of the Korean Fracture Society.2017; 30(3): 124. CrossRef - Clinical and Radiographical Follow-up for Residual Displacement of Fracture Fragments after Interlocking Intramedullary Nailing in Humeral Shaft Fractures
Jae-Kwang Yum, Dong-Ju Lim, Eui-Yub Jung, Su-Een Sohn
The Journal of the Korean Shoulder and Elbow Society.2013; 16(2): 107. CrossRef - Operative Treatment of Humerus Shaft Fracture: Conventional Open Plating or Minimally Invasive Plate Osteosynthesis
Hyun-Joo Lee, Chang-Wug Oh
Journal of the Korean Fracture Society.2012; 25(2): 155. CrossRef
 Cite
CiteMinimally Invasive Anterior Plating of Humeral Shaft Fractures
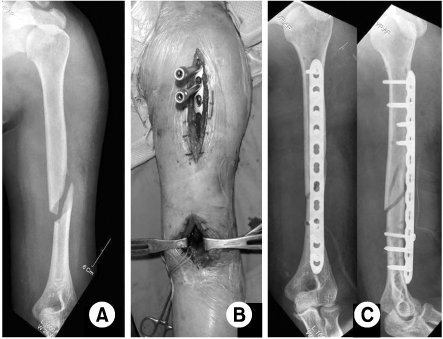
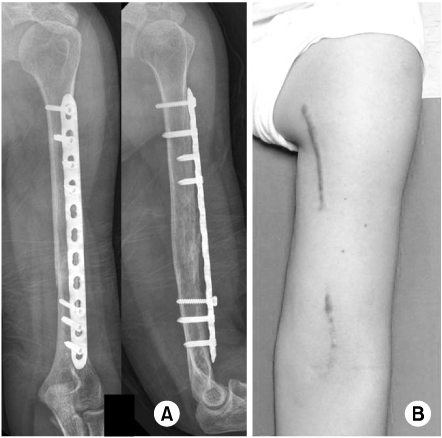
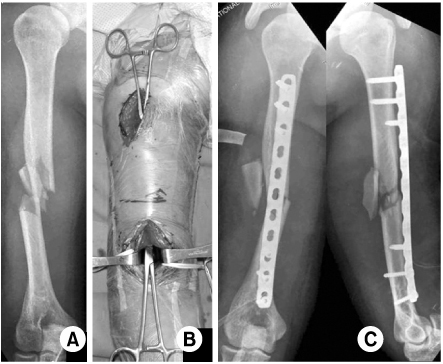
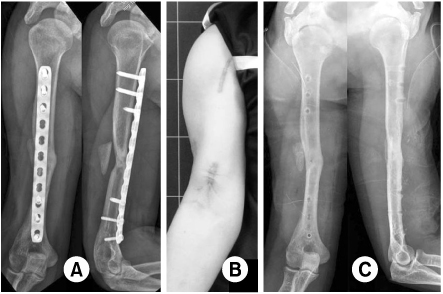
Fig. 1
(A) A 47-year-old female sustained a spiral fracture of the left humerus diaphysis due to in-car accident.
(B, C) Through the submuscular tunnel, a locking compression plate was inserted and fixed with an acceptable alignment.
Fig. 2
(A) Ten months after the surgery, radiographs demonstrated a complete osseous union.
(B) Note the skin scars of proximal and distal incision without involving the fracture site.
Fig. 3
(A) A 34-year-old female sustained a comminuted fracture of the humeral shaft after traffic accident.
(B) After making the submuscular tunnel using Kelly clamps, a locking compression plate was fixed with the MIPO procedure.
(C) Note an acceptable alignment without reducing the comminuted fragment.
Fig. 4
(A) Six months after the surgery, the osseous union was achieved.
(B) Note the small incision scars of proximal and distal incision.
(C) Note the firm union after the removal of plate.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Minimally Invasive Anterior Plating of Humeral Shaft Fractures

