 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 22(3); 2009 > Article
-
Original Article
- Retrograde Intramedullary Nailing or the Treatment of Segmental Femoral Shaft Fracture Including Distal Part
- Jong-Ho Yoon, M.D., Byung-Woo Ahn, M.D., Chong-Kwan Kim, M.D., Jin-Woo Jin, M.D., Ji-Hoon Lee, M.D., Hyun-Ku Cho, M.D., Joo-Hyun Lee, M.D.
-
Journal of the Korean Fracture Society 2009;22(3):145-151.
DOI: https://doi.org/10.12671/jkfs.2009.22.3.145
Published online: July 31, 2009
Department of Orthopedic Surgery, Masan Samsung Hospital, Sungkyunkwan University School of Medicine, Masan, Korea.
- Address reprint requests to: Jin-Woo Jin, M.D. Department of Orthopedic Surgery, Masan Samsung Hospital, Sungkyunkwan University School of Medicine, 50, Hapsung 2-dong, Hoewon-gu, Masan 630-520, Korea. Tel: 82-55-290-6030, Fax: 82-55-290-6888, ortho_ss@yahoo.co.kr
• Received: November 7, 2008 • Revised: January 1, 2009 • Accepted: April 22, 2009
Copyright © 2009 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 999 Views
- 6 Download
- 1 Crossref
Abstract
-
Purpose
- To evaluate the usefulness of the retrograde intramedullary nailing for the treatment of segmental femoral shaft fracture including distal part.
-
Materials and Methods
- We reviewed 15 patients of segmental femoral fracture, who had treated with retrograde intramedullary nailing and followed-up more than 1 year from January 2003 to October 2007. There were 10 men, 5 women, and the mean age was 45 years old. There were associated fracture in 10 cases. We evaluate the time for union, non-union and malunion by radiologic finding and functional assessment by Sanders' criteria.
-
Results
- The mean time of union was 21 weeks. There was one delayed union in proximal fracture site. There was no shortening more than 1.5 cm, no angular deformity more than 10 degrees, no postoperative infection or instability. According to Sanders' criteria, there were excellent clinical results in 9 cases, good results in 5 cases and fair result in 1 case.
-
Conclusion
- The retrograde intramedullary nailing can be a useful method for treatment of segmental femoral shaft fracture including distal part.
- 1. Acharaya KN, Rao MR. Retrograde nailing for distal third femoral shaft fractures: a prospective study. J Orthop Surg (Hong Kong), 2006;14:253-258.ArticlePDF
- 2. Anastopoulos G, Asimakopolous A, Exarchou E, Pantazopoulos T. Closed interlocked nailing in comminuted and segmental femoral shaft fractures. J Trauma, 1993;35:772-775.Article
- 3. Anup K, Mehra MM. Retrograde femoral interlocking nail in complex fractures. J Orthop Surg (Hong Kong), 2002;10:17-21.ArticlePDF
- 4. Browner BD, Levine AM, Jupiter JB, Trafton PG. Skeletal trauma. 2nd ed. Philadelphia: WB Saunders Co; 1998. p. 2033-2079.
- 5. Cavallo RJ, Strauss E. Functional outcome after operative management of supracondylar femur fractures above or below orthopaedics implants, In: Proceeding of 62nd. Annual Meeting of American Academy of Orthopaedics Surgeons; 1995. p. 154.
- 6. Chung PH, Hwang CS, Kang S, Kim JP, Jeon YJ. Treatment of suprachondylar-intercondylar femoral fractures with a retrograde intramedullary nailing. J Korean Fract Soc, 2004;17:110-116.Article
- 7. Danziger MB, Caucci D, Zecher SB, Segal D, Covall DJ. Treatment of intercondylar and supracondylar distal femur fractures using the GSH supracondylar nail. Am J Orthop, 1995;24:684-690.
- 8. Kregor PJ, Templeman D. Associated injuries complicating the management of acetabular fractures. Orthop Clin North Am, 2002;33:73-95.Article
- 9. Leung KS, Shen WY, Mui LT, Grosse A. Interlocking intramedullary nailing for supracondylar & intercondylar fracture of the distal part of the femur. J Bone Joint Surg Am, 1991;73:332-340.
- 10. Lucas SE, Seligon D, Henry SL. Intramedullary supracondular nailing of femoral fractures. Clin Orthop Relat Res, 1993;296:200-206.
- 11. Mize R. Treatment options for fractures of the dista femur. AAOS. Instr Course Lect, 1994;43:109-117.
- 12. Moed B, Watson T, Cramer K, Karges DE, Teefey JS. Unreamed retrograde intramedullary nailing of fractures of the femoral shaft. J Orthop Trauma, 1998;12:334-342.Article
- 13. Morgan E, Ostrum R, DiCicco J, McElroy J, Poka A. Effects of retraograde femoral intramedullary nailing of the patellofemoral articulation. J Orthop Trauma, 1999;13:13-16.
- 14. Oh CW, Oh JK, Min WK, et al. Comparison of operative methods between retragrade and antegrade nailing for ipsilateral femoral shaft and neck fracture. J Korean Fract Soc, 2007;20:135-140.Article
- 15. Ostrum RF. Treatment of floating knee injuries through a single percutaneous approach. Clin Orthop Relat Res, 2000;375:43-50.Article
- 16. Ostrum R, Agarwal A, Lakatos R, Poka A. Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma, 2000;14:496-501.
- 17. Papadokostakis G, Papakostidis C, Dimitriou R, Giannoudis PV. The role and efficacy of retrograding nailing for the treatment of diaphyseal and distal femoral fractures: a systematic review of the literature. Injury, 2005;36:813-822.Article
- 18. Patterson BM, Routt ML Jr, Benirschke SK, Hansen ST Jr. Retrograde nailing of femoral shaft fractures. J Trauma, 1995;38:38-43.Article
- 19. Ricci W, Bellabara C, Evanoff B, Herscovici D, DiPasquale T, Sanders R. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma, 2001;15:161-169.Article
- 20. Ruedi TP, Luscher JN. Results after internal fixations of comminuted fractures of the femoral shaft with DC plates. Clin Orthop Relat Res, 1979;138:74-76.
- 21. Sanders R, Regazzoni P, Ruedi TP. Treatment of suprachondylar - intercondylar fractures of femur using the dynamic condylar screw. J Orthop Trauma, 1989;3:214-222.
- 22. Stewart MJ, Sisk TD, Wallace SL Jr. Fractures of the distal third of the femur: a comparison of methods of treatment. J Bone Joint Surg Am, 1966;48:784-807.
- 23. Tornetta P III, Tiburzi D. Antegrade or retrograde reamed femoral nailing. J Bone Joint Surg Br, 2000;82:652-654.ArticlePDF
- 24. Wolinsky P, Tejwani N, Richmond JH, et al. Controveries in intramedullary nailing of femoral shaft fractures. J Bone Joint Surg Am, 2001;83:1404-1415.
REFERENCES
Fig. 1
(A) Initial anteroposterior and lateral radiographs of a 59-year-old female with segmented femoral shaft fracture and ipsilateral patellar fracture.
(B) Femoral shaft was fixed with retrograde intramedullary nailing and patellar fracture was fixed with Tension Bend Wiring.
(C) Follow-up radiographs, made at 17-month after operation, showed that well united femoral shaft fracture and patellar fracture.
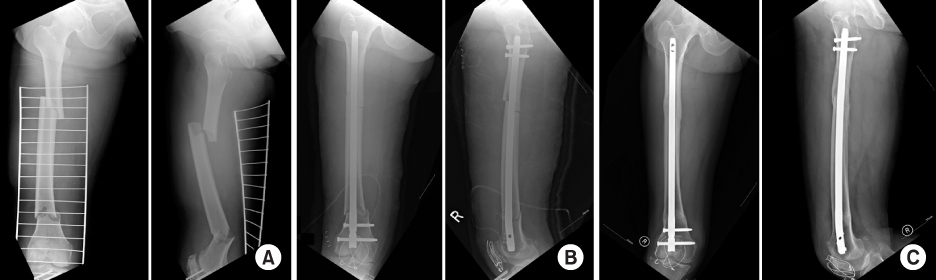
Fig. 2
(A) Initial anteroposterior and lateral radiographs of a 62-year-old male with segmented femoral shaft fracture, ipsilateral femoral neck fracture and ipsilateral patellar fracture.
(B) Femoral shaft was fixed with retrograde intramedullary nailing, neck was fixed with 3 cannulated cancellous screws and the patella was fixed with tension bend wirings.
(C) Follow-up radiographs, made at 16-month after operation, showed that well united femoral shaft, neck & patellar fracture and removed hardwares.
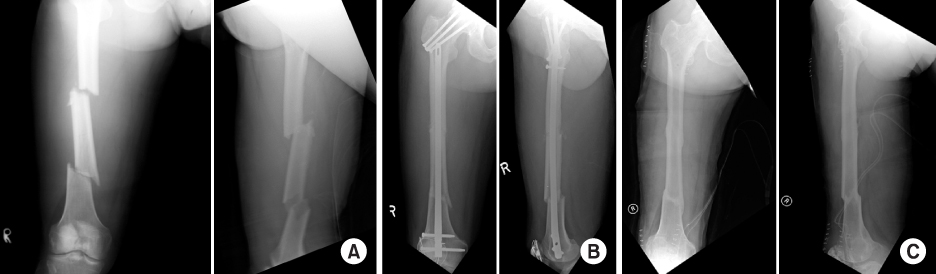
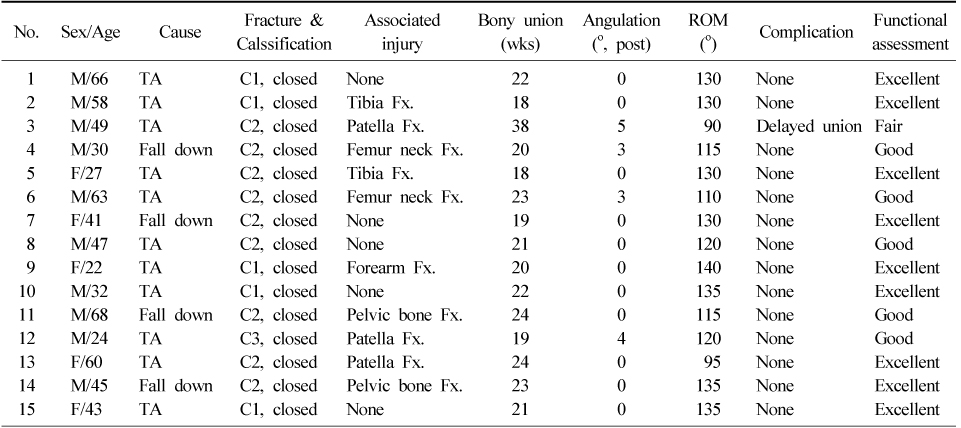
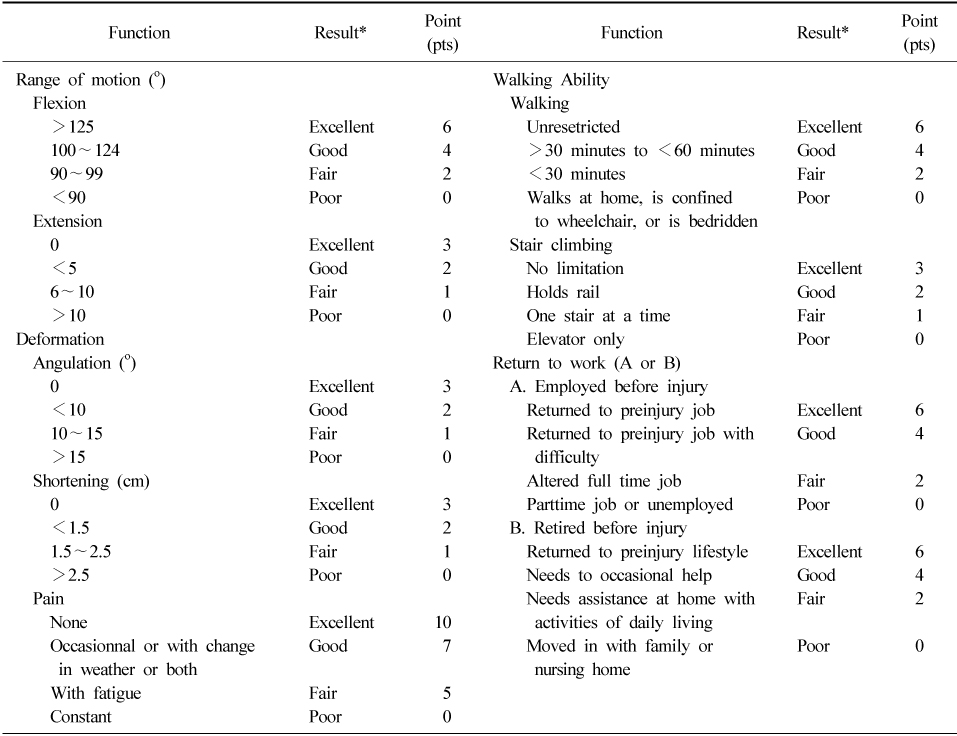
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Analysis of Risk Factors for Nonunion after Intramedullary Nailing of Femoral Shaft Fracture in Adult
Yong-Woon Shin, Yerl-Bo Sung, Jeong Yoon Choi, Minkyu Kim
Journal of the Korean Fracture Society.2011; 24(4): 313. CrossRef
 Cite
CiteRetrograde Intramedullary Nailing or the Treatment of Segmental Femoral Shaft Fracture Including Distal Part
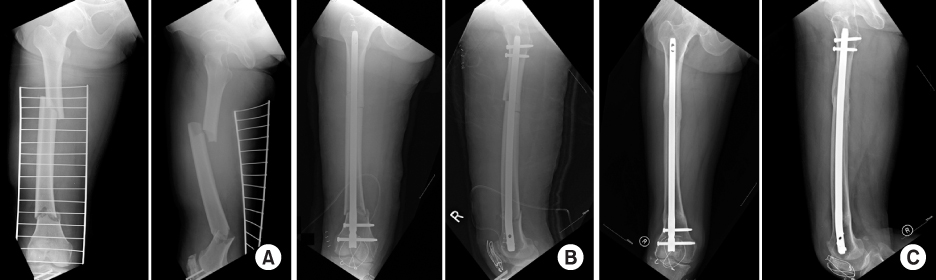
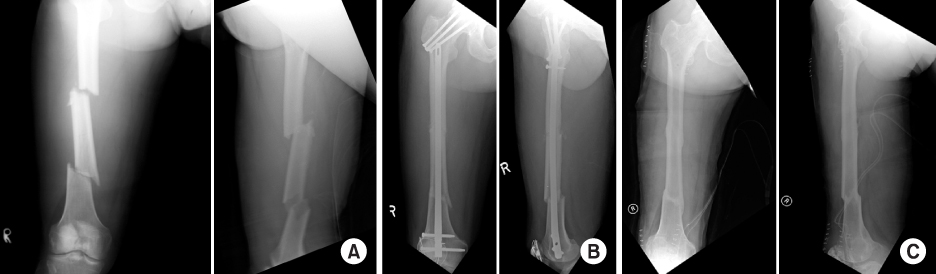
Fig. 1
(A) Initial anteroposterior and lateral radiographs of a 59-year-old female with segmented femoral shaft fracture and ipsilateral patellar fracture.
(B) Femoral shaft was fixed with retrograde intramedullary nailing and patellar fracture was fixed with Tension Bend Wiring.
(C) Follow-up radiographs, made at 17-month after operation, showed that well united femoral shaft fracture and patellar fracture.
Fig. 2
(A) Initial anteroposterior and lateral radiographs of a 62-year-old male with segmented femoral shaft fracture, ipsilateral femoral neck fracture and ipsilateral patellar fracture.
(B) Femoral shaft was fixed with retrograde intramedullary nailing, neck was fixed with 3 cannulated cancellous screws and the patella was fixed with tension bend wirings.
(C) Follow-up radiographs, made at 16-month after operation, showed that well united femoral shaft, neck & patellar fracture and removed hardwares.
Fig. 1
Fig. 2
Retrograde Intramedullary Nailing or the Treatment of Segmental Femoral Shaft Fracture Including Distal Part
Summary of patient data
Functional evaluation scale (by Sanders et al, 1991)
*Excellent=36~40 pts, Good=26~35 pts, Fair=16~25 pts, Poor=0~15 pts.
Table 1
Summary of patient data
Table 2
Functional evaluation scale (by Sanders et al, 1991)
*Excellent=36~40 pts, Good=26~35 pts, Fair=16~25 pts, Poor=0~15 pts.

