 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 35(1); 2022 > Article
- Case Report Early Corrective Osteoclasis for Malunited Pediatric Medial Condylar Fracture of the Humerus
- Hong Jun Jung, Ho Youn Park, Yuna Kim
-
Journal of Musculoskeletal Trauma 2022;35(1):21-25.
DOI: https://doi.org/10.12671/jkfs.2022.35.1.21
Published online: January 31, 2022
1Department of Orthopedic Surgery, Sahmyook Medical Center, Seoul, Korea
2Department of Orthopedic Surgery, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
2Department of Orthopedic Surgery, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
- 709 Views
- 0 Download
- 0 Crossref
- 0 Scopus
Abstract
Fractures of the medial condyle of the distal humerus in children are very rare, and the younger the age, the more difficult it is to diagnose. These fractures include an intra-articular fracture and a Salter–Harris type IV growth plate fracture. Therefore, the prognosis is poor if the fracture is neglected or misdiag-nosed because of the high incidence of complications such as nonunion, angular deformity, or joint contracture. This paper reports a case of a four-year-old child who presented with a malunion of the medial condyle of the humerus with good results after an early corrective osteoclasis.
J Korean Fract Soc. 2022 Jan;35(1):21-25. Korean.
Published online Jan 25, 2022.
https://doi.org/10.12671/jkfs.2022.35.1.21
Published online Jan 25, 2022.
https://doi.org/10.12671/jkfs.2022.35.1.21
Copyright © 2022 The Korean Fracture Society.
Case Report
소아 상완골 내과 골절 부정 유합에서 시행한 조기 교정 절골술: 증례 보고

Early Corrective Osteoclasis for Malunited Pediatric Medial Condylar Fracture of the Humerus: A Case Report
초록
소아의 원위부 상완골 내과 골절은 매우 드물며 나이가 어릴수록 진단이 어려울 수 있다. 이는 관절내 골절이며 Salter–Harris IV형의 성장판 골절이므로 골절이 방치되거나 오진이 되면 불유합, 각편형, 관절 구축 등의 합병증 발생률이 매우 높고 예후가 불량하다. 저자들은 상완골 내과 골절 부정 유합으로 내원한 4살 소아 환자에서 조기에 교정 절골술 후 좋은 결과를 얻었기에 문헌 고찰과 함께 증례를 보고하고자 한다.
Abstract
Fractures of the medial condyle of the distal humerus in children are very rare, and the younger the age, the more difficult it is to diagnose. These fractures include an intra-articular fracture and a Salter–Harris type IV growth plate fracture. Therefore, the prognosis is poor if the fracture is neglected or misdiagnosed because of the high incidence of complications such as nonunion, angular deformity, or joint contracture. This paper reports a case of a four-year-old child who presented with a malunion of the medial condyle of the humerus with good results after an early corrective osteoclasis.
Keywords
Humerus, Medial condyle, Malunion, Early corrective osteoclasis
상완골, 내과, 부정 유합, 조기 교정 절골술
소아의 원위부 상완골 내과 골절은 전체 소아 골절의 1%-2% 정도를 차지할 정도로 매우 드물다.1) 골간단부 골편이 매우 얇고 대부분의 골편이 연골로 이루어져 있어 진단이 어려울 수 있고 골절 진단을 놓치는 경우도 종종 있다. 골절이 방치되거나 오진이 되면 불유합, 각편형, 관절 구축 등의 합병증 발생률이 매우 높기 때문에 예후는 불량하다. 이는 관절 내 골절, Salter–Harris IV형 성장판 골절이고 상완골 내과가 취약한 혈액공급을 받기 때문이다.1,2,3) 그러나 골절 초기에 치료가 적절히 이루어진다면 예후는 나쁘지 않은 것으로 알려져 있다. 그러므로 정확한 초기 골절의 진단 및 적절한 치료는 매우 중요하다. 대부분의 급성기 골절은 석고나 경피적 핀 고정술로 치료되며 가끔씩 관혈적 정복술이 요구되기도 한다.2) 지금까지 소아 상완골 내과 급성 골절의 치료에 대한 여러 보고가 있었지만 부정 유합에 대해서 시행한 교정 절골술에 대한 보고는 거의 없다. 저자들은 주관절 구축을 동반한 상완골 내과 골절의 부정 유합이 있는 4살 환자에서 조기에 절골술을 시행하여 치료한 증례를 보고하고자 한다.
증례 보고
4살 환자가 미끄럼틀에서 떨어진 후 발생한 우측 팔꿈치 통증으로 응급실에 내원하였다. 팔꿈치가 부어 있었고 통증이 있는 관절 운동 제한 소견을 보였으며 신경 혈관 검사상 말초신경 이상은 없었다. 초기 팔꿈치 방사선 사진에서 상완골 내과에 골절선을 확인할 수 있었으며 중등도의 연부조직 부종 소견이 있었다(Fig. 1). 응급실에서는 컴퓨터 단층촬영이나 자기공명영상 등의 정밀검사를 하지 않았고 90도 팔꿈치 굴곡, 전완부 중립 위치로 장상지 부목을 적용하였다. 이후 3일 후에 외래 진료를 예약해주었다.

Fig. 1
Simple radiograph of the elbow shows a linear fracture line of the medial condyle (arrowheads) and soft tissue swelling at the medial side of the elbow.
외래에서 방사선 검사 추시를 하였으며 골편의 전위가 거의 없어 장상지 캐스트를 적용하였다. 일주일 후 외래 진료 예약을 해주었지만 환자는 내원하지 않았다. 수상 후 6주 후 환자는 캐스트를 하지 않은 상태로 보호자와 함께 외래를 재방문하였다. 환자 보호자는 이전 외래에서 적용한 캐스트를 환자가 안 아파하여 일주일 후 풀렀다고 하였다. 재방문 환자의 팔꿈치는 90도로 굴곡 구축되어 있었고 수동적 관절 운동을 시행하려 했을 때 심한 통증을 호소하였다. 시행한 단순방사선 영상에서 내측 상과 부분에 가골 형성 등 부정 유합 소견을 시사하는 소견이 보였다(Fig. 2). 자기공명영상 검사를 두 차례 시도하였지만 환자의 낮은 순응도로 검사를 실패하였고 환자 나이가 4세였고 대부분 연골로 이루어져 있어 컴퓨터 단층촬영 검사에서는 주관절 4면 단순방사선 검사(전후, 측면, 내외측 사면)에서 보이는 소견 외에 추가로 얻을 수 있는 정보가 거의 없을 것으로 생각되어 촬영하지 않았다. 관절 상태 확인을 위하여 전신마취하에서 관절조영술과 필요하면 교정 절골술을 시행하기로 결정하였다.
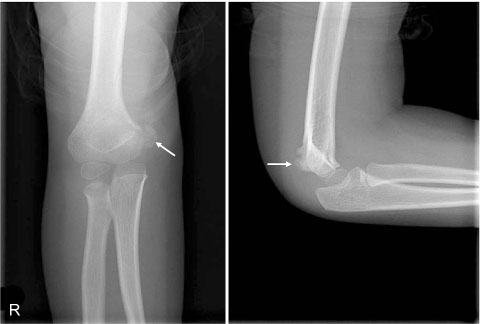
Fig. 2
Simple radiographs taken six weeks after the injury showed callus formation at the superomedial side of the medial epicondyle (arrows). They suggest malunion of medial condylar fracture of the distal humerus.
전신마취하에 21 gauge spinal needle을 요소두(radiocapitellar) 관절에 삽입한 후 멸균 증류수와 혼합한 3-5 ml 정도의 Iodine (IOBRIX INJ 350®; Taejoon Pham, Seoul, Korea)을 관절 내에 주입하였다. C-arm을 이용하여 관절 상태를 확인하였고 척상완(ulnohumeral) 관절의 불규칙한 관절면과 가골이 형성되면서 부정 유합이 진행되고 있는 소견을 확인할 수 있었다(Fig. 3). 관절 조영술 후 내측 피부절개를 가한 후 먼저 척골 신경을 확인한 후 나일론 테이프로 보호하였다. 내측 상과 부분의 가골을 제거한 후 이전 골절 부위를 통한 절골술을 시행하였다. 골유합이 완전하지 않아 관절 내 골절면까지 쉽게 분리가 가능하였다. 골편을 해부학적으로 정복하여 3개의 1.5 mm K-강선을 이용하여 고정하였다(Fig. 4). K-강선 끝은 잘라서 피부 밑에 묻었으며 창상 봉합 후 장상지 부목을 적용하였다. 술 후 2주째 실밥을 제거하고 장상지 캐스트를 적용하여 2주간 추가 고정을 하였다. 술 후 4주 후에 캐스트를 제거한 후 탈부착 가능한 장상지 요깁스를 적용하여 관절 운동을 시작하였다. 술 후 3개월째 골유합 소견이 보여 전신마취하에 K-강선을 제거하였다(Fig. 5). 술 후 6개월째 환자 주관절은 30도 신전에서 95도 굴곡이 가능하였으며 단순방사선상 골유합이 잘 유지되는 소견을 보였다(Fig. 6). 술 후 1년째 촬영한 단순방사선상 각변형이나 성장 정지된 소견은 보이지 않았으며 통증 없이 신전 10도에서 130도 굴곡 가능한 소견을 보였다(Fig. 7). 술 후 2년째 촬영한 단순방사선 소견에서도 내측 골극 형성 외에 다른 소견은 보이지 않았으며 통증 없이 전범위 관절 운동 가능한 소견을 보였다(Fig. 8).

Fig. 3
(A) Intra-operative fluoroscopic findings showed a 21 gauge spinal needle was inserted into the radiocapitellar joint. (B) Images after dye injection showed incongruent ulnohumeral joint (arrowhead). The medial condylar fragment was uniting with callus formation at the superomedial aspect of the original fracture site (arrow).
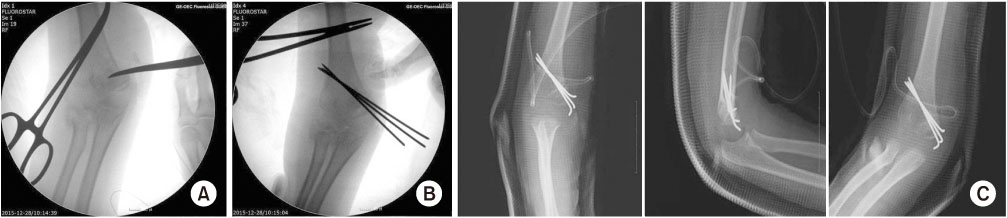
Fig. 4
(A) Osteoclasis was performed using a small osteotome at the fracture level, and (B) after reduction of the articular surface, the fragments were fixed with three 1.5 mm K-wires. (C) Postoperative anteroposterior, lateral, and medial oblique simple radiographs showed good reduction and firm fixation.

Fig. 5
Postoperative three-month radiographs after pin removal showed bony union.

Fig. 6
(A) Postoperative six-month radiographs showed bony union and no growth arrest, and (B) clinical photos showed the elbow motion was possible from 30° extension to 95° further flexion.

Fig. 7
(A) Postoperative one-year radiographs showed growth arrest and no angular deformity, and (B) clinical photos showed that the elbow motion was possible from 10° extension to 130° further flexion without difficulty and pain.
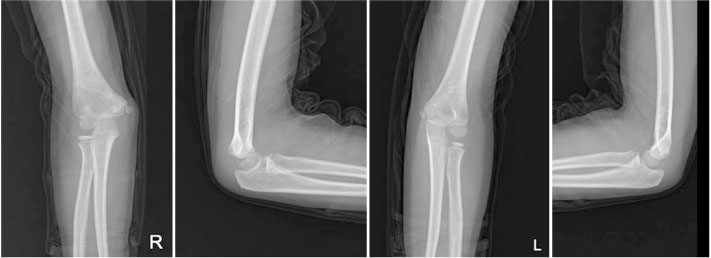
Fig. 8
Postoperative two-year radiographs showed no growth arrest and no angular deformity compared to the contralateral normal elbow but medial side spur formation.
고찰
저자들은 소아 환자에서 상완골 내과 골절의 부정 유합 발생 시 조기 교정 절골술로 적극적인 개입을 하는 것이 좋은 치료 방법 중 하나가 될 수 있다고 생각한다. 상완골 내과 골절은 관절내 골절이고 Salter–Harris IV형 손상으로 해부학적 정복이 매우 중요하다.4) 만일 이에 실패하면 성장판 손상으로 인한 성장 정지로 각 변형이 올 수 있으며 심지어는 단축(longitudinal shortening)이 발생할 수도 있다.4,5) 이 증례에서 환아가 보이는 수상 후 6주째 굴곡 구축은 심한 통증을 동반한 90도 주관절 완전 굴곡 구축으로 단순한 고정으로 인한 구축과는 양상이 매우 달랐다. 저자들은 이것을 관절면의 불규칙성으로 인한 부정 유합 때문이라고 생각하였다. 소아에서 골절 후에 고정으로 통증을 동반하는 관절 구축이 심하게 발생하는 경우는 드물기 때문이다.6) 심지어 이 환자는 첫 외래 진료 후 부목을 충분히 적용하지 않았으며 절골술 후 4주 후부터 통증이 많이 감소하였고 관절 운동이 회복되는 양상을 보였기 때문이다.
상완골 활차의 골화 시기는 약 9세이다.7) 대부분의 상완골 내과 골절은 8-12세 사이에 발생한다.3,8) 하지만 6개월, 4.7년에서 발생한 상완골 내과 골절에 대한 보고도 있다.2,9) 이 증례의 환자는 4세였으며 나이가 어릴수록 골편의 크기가 작고 연골이 차치하는 부분이 많기 때문에 진단이 어려울 수 있다. 조기에 골절 진단이 잘 이루어졌다면 전위가 심하지 않은 경우 보존적 치료, 전위가 있다면 수술적 치료(경피적 핀고정술 혹은 관혈적 정복술 및 핀고정술)를 시행한다.1,2) 진단이 잘못되어 치료가 지연되면 예후가 좋지 않기 때문에 수술을 시행할지 경과를 관찰할 것인지는 정밀 검사 후 결정을 해야 한다. 진단을 위해 자기공명영상 검사나 관절조영술 같은 추가 검사가 필요할 수 있다. 자기공명영상 검사는 어린 환아에게 있어서 낮은 순응도로 실패할 수 있으며 진정제 투여로 인하여 위험할 수 있는데 이때는 전신마취하 관절조영술이 도움이 된다.2) 관절조영술로 부정 유합된 위치를 확인할 수 있으며 조기에 교정 절골술로 관절면의 해부학적 정복을 얻을 수 있다.
수술 중에는 골편의 무혈성 괴사를 막기 위해서 주변의 연부조직 박리 시 주의해야 한다. 활차의 무혈성 괴사의 위험이 높기 때문에 오히려 불유합을 받아들이는 것이 더 좋은 기능적 결과를 보였다라고 발표한 문헌도 있다.2,3) 저자들은 최대한 연부조직을 보호하고 연부조직 조작을 최소화하여 수술을 시행하였다. 또한 팔꿈치 내측 접근법을 이용하므로 척골 신경을 주의해야 한다. 상완골 내측 상과 합병증에 대해서 상과 절골술(supracondylar osteotomy)에 대한 보고가 있는데 저자들은 관절외 절골술을 시행하였고 좋은 기능적 결과를 얻었다라고 발표하였다.3) 하지만 관절면의 해부학적 정복은 교정하지 않았다. 이 증례에서의 환자는 수상 후 6주 경에 다시 병원에 내원하였고 저자들은 당시 부정 유합된 골절면이 완전히 정상골의 강도를 갖지는 않는다고 생각하였다. 그러므로 골절면에서 시행한 절골술을 어렵지 않게 시행할 수 있었다. 더 장기적인 추시가 요구되지만 저자들은 부정 유합이 진행되고 있는 소아 상완골 내과 골절 환자가 내원했을 때 골절면을 통한 조기 교정 절골술이 도움이 될 것으로 생각한다.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Bensahel H, Csukonyi Z, Badelon O, Badaoui S. Fractures of the medial condyle of the humerus in children. J Pediatr Orthop 1986;6:430–433.
-
-
Leet AI, Young C, Hoffer MM. Medial condyle fractures of the humerus in children. J Pediatr Orthop 2002;22:2–7.
-
-
Papavasiliou V, Nenopoulos S, Venturis T. Fractures of the medial condyle of the humerus in childhood. J Pediatr Orthop 1987;7:421–423.
-
-
Flynn JM, Skaggs DL, Waters PM. In: Rockwood and Wilkins’ fractures in children. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2015. pp. 734-742.
-
-
Cass JR, Peterson HA. Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059–1070.
-
-
Bogdan M, Mikov A. The role of physical therapy in the treatment of post-traumatic contracture of the elbow in children. Med Pregl 2017;70:58–61.
-
-
Cheng JC, Wing-Man K, Shen WY, et al. A new look at the sequential development of elbow-ossification centers in children. J Pediatr Orthop 1998;18:161–167.
-
-
Varma BP, Srivastava TP. Fracture of the medial condyle of the humerus in children: a report of 4 cases including the late sequelae. Injury 1972;4:171–174.
-
-
De Boeck H, Casteleyn PP, Opdecam P. Fracture of the medial humeral condyle. Report of a case in an infant. J Bone Joint Surg Am 1987;69:1442–1444.
-
 Cite
Cite
