 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > > Ahead-of print articles > Article
-
Case Report
- Fixation with two headless compression screws and a distal-radius bone graft for proximal scaphoid nonunion with dorsal intercalated segment instability deformity: a report of three cases
-
Seonjeong Lee
 , Won Sun Lee, Jae Kwang Kim
, Won Sun Lee, Jae Kwang Kim -
DOI: https://doi.org/10.12671/jmt.2026.00136
Published online: July 7, 2026
Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Correspondence to: Jae Kwang Kim Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3523 Email: orth4535@gmail.com
• Received: March 27, 2026 • Revised: April 30, 2026 • Accepted: May 11, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 36 Views
- 1 Download
Abstract
-
Proximal scaphoid nonunion is difficult to treat because the proximal fragment is small and biologically compromised. Secure fixation can be especially challenging when dorsal intercalated segment instability (DISI) is present and requires correction. We report three male patients with proximal scaphoid nonunion and DISI deformity who underwent volar fixation with two 2.4-mm headless compression screws and cancellous bone graft harvested from the distal radius at the Lister tubercle. Preoperative computed tomography confirmed a proximal nonunion line and proximal fragment dimensions considered sufficient for dual-screw fixation, and magnetic resonance imaging showed no definite avascular necrosis. Early postoperative computed tomography showed maintained fixation and alignment in all three patients. Although CT-confirmed union at final follow-up was not uniformly available, radiographic union defined on plain radiographs was achieved in all cases without loss of alignment or carpal collapse. Carpal alignment improved in two patients, but DISI persisted in one. One patient underwent secondary removal of a preexisting loose body and one screw. This small case series suggests that dual-screw fixation with cancellous grafting may be technically feasible in selected proximal scaphoid nonunions with concomitant DISI.Level of evidence: IV.
Introduction
Scaphoid nonunion remains a challenging problem in wrist surgery, particularly when the nonunion involves the proximal pole. The proximal fragment is often small and biologically compromised, making stable fixation and reliable union difficult to achieve [1]. In addition, proximal scaphoid nonunion may be accompanied by carpal malalignment, including dorsal intercalated segment instability (DISI), which further complicates treatment [2,3].
Headless compression screw fixation is widely used for scaphoid fractures and nonunions [4-6]. However, in proximal nonunion, a single-screw construct may provide insufficient rotational control because of the limited size of the proximal fragment and the multidirectional loading environment of the scaphoid [7]. Biomechanical evidence suggests that a dual-screw construct can improve qualitative rotational control compared with a single screw, although overall stiffness and load to failure may be similar [8]. Garcia et al. [9] reported excellent union in a heterogeneous series of scaphoid nonunions treated with two headless compression screws and bone grafting; however, the majority of cases involved waist or distal third, and the presence of concomitant DISI in those subgroups was not specifically described.
The purpose of this report is to describe three proximal scaphoid nonunions with DISI deformity treated using a uniform strategy of dorsal cancellous bone graft harvest from the distal radius at the Lister tubercle and volar fixation with two 2.4-mm headless compression screws. We focused on feasibility, radiographic alignment, functional outcomes, and complications of this technique in carefully selected cases.
Case reports
This retrospective case series was approved by the Institutional Review Board (IRB) Committees of the Medical Research Institute of Asan Medical Center (IRB No. S2025-1785-0001) and was conducted in accordance with the principles of the Declaration of Helsinki. Because the study used anonymized patient data and posed minimal risk to the participants, the requirement for informed consent was waived by the IRB.
This retrospective report describes three male patients with symptomatic proximal scaphoid nonunion and DISI deformity who were treated by a single senior surgeon between March 2023 and March 2025 using the same technique of dorsal distal-radius cancellous bone grafting and volar dual 2.4-mm headless compression screw fixation. Proximal nonunion was defined when the fracture or nonunion line was located proximal to the dorsal apex of the scaphoid on computed tomography (CT) [10]. DISI deformity was defined as a radiolunate (RL) angle of 15° or greater on lateral radiographs [11]. No patient showed advanced degenerative arthritic change at presentation. Preoperative magnetic resonance imaging (MRI) was available in all patients and did not show definite proximal-pole avascular necrosis (AVN). Demographic and radiographic characteristics of the three cases are summarized in Table 1.
Preoperative CT was used to assess nonunion location, displacement, proximal fragment morphology, and the feasibility of dual distal-to-proximal screw fixation. Proximal fragment width and depth were measured on reconstructed coronal and sagittal CT images using the cut in each plane on which the proximal fragment appeared longest (Fig. 1). Because two 2.4-mm screws occupy a combined diameter of 4.8 mm and the DePuy Synthes 2.4-mm short-thread screw has a 4-mm leading threaded portion, fragment width greater than 4.8 mm and fragment depth greater than 4 mm were used as supportive thresholds when considering this technique. Depth was defined as the distance from the nonunion line to the proximal subchondral boundary in the intended distal-to-proximal screw direction. However, because the proximal pole has a dome-shaped three-dimensional morphology and usable bone stock varies according to the exact screw trajectory and the bone bridge required between the two screws, these measurements were not considered absolute criteria. Final suitability for dual-screw fixation was determined qualitatively by integrating the measurements with overall fragment morphology, the proximal extent of the fracture line, possible screw trajectories, and proximity to the articular surfaces.
Radiographic union at the latest follow-up was assessed on plain radiographs by the treating surgeon. CT-confirmed union was not uniformly available at final follow-up; rather, union was defined as bridging callus at least three cortices on posteroanterior, lateral, and/or oblique views, similar to the radiographic definition used by Rodriguez-Fontan et al. [12]. Time to union was defined as the first postoperative visit at which radiographic bridging across at least three cortices was observed. Postoperative radiographs were routinely obtained at approximately 2 weeks, 6 weeks, 12 weeks, 6 months, 12 months, and 24 months, and CT was additionally obtained at approximately 6 weeks. In all three cases, union was first observed on radiographs obtained approximately 12 weeks after surgery (Table 2). Early postoperative CT was used to confirm screw position and alignment. Functional outcomes were retrospectively extracted from clinical records and included wrist volar flexion and dorsiflexion, grip strength, visual analog scale (VAS) pain score, Disabilities of the Arm, Shoulder and Hand (DASH) score, and patient satisfaction.
In all cases, the procedure followed a two-incision strategy conceptually similar to the cancellous-grafting technique that was previously described [13], but joystick Kirschner (K)-wire manipulation of the fragments was not used. Through a volar approach, the nonunion site was exposed, interposed fibrous tissue and sclerotic bone were excised, and the nonunion surfaces were prepared until viable cancellous bone was encountered. Scaphoid reduction and carpal alignment were confirmed under fluoroscopic guidance, but degree of DISI correction varied (Table 1). Guidewires for the planned screws and an additional temporary derotational K-wire were then inserted from the distal scaphoid toward the proximal pole to maintain the reduced position. Through a separate limited dorsal approach centered just proximal to the Lister tubercle, cancellous bone graft was harvested with identification and protection of the extensor pollicis longus tendon. This dorsal harvest was preferred because cancellous bone could be obtained readily through a small dorsal cortical window.
A portion of the cancellous graft was first packed into the dorsal and deep aspect of the prepared cavity while preserving the planned screw paths. Fixation was then performed with two 2.4-mm cannulated short-thread headless compression screws with a 4-mm leading threaded portion (DePuy Synthes). Each 2.4-mm screw was inserted over its guidewire so that the leading thread crossed the nonunion site and engaged the proximal fragment. After definitive fixation, the guidewires and temporary derotational K-wire were removed, and the remaining volar defect was packed with cancellous bone graft. Reduction, the degree of DISI correction, screw position, and absence of radiocarpal or midcarpal joint violation were checked on anteroposterior, lateral, oblique, and scaphoid-view fluoroscopy. Postoperatively, the wrist was immobilized in a thumb-spica cast for 2 months, followed by range-of-motion exercises.
Patient information and clinical findings
A 23-year-old male patient presented with persistent pain in the left wrist, which was his non-dominant side, after a fall approximately 8 months earlier. He had initially been told that plain radiographs were unremarkable, but his symptoms persisted despite conservative treatment. At presentation, he reported pain during exercise and wrist hyperextension, with difficulty loading the hand. He had a 2 pack-year smoking history and no diabetes.
Diagnostic assessment
Plain radiographs demonstrated scaphoid nonunion with carpal malalignment, and CT confirmed proximal scaphoid nonunion with DISI deformity. Preoperative SL and RL angles were 73.6° and 20.4°, respectively. Preoperative nonenhanced MRI did not show definite AVN.
Therapeutic intervention
He underwent nonunion debridement, dorsal cancellous bone graft harvest from the Lister tubercle, and volar fixation using two 2.4-mm headless compression screws. The wrist was immobilized in a thumb-spica cast for 2 months, followed by range-of-motion exercises.
Follow-up and outcomes
Postoperative CT obtained 7 weeks after surgery demonstrated maintained screw position. Immediate postoperative scapholunate (SL) and RL angles were 74.6° and 23.7°, and final SL and RL angles were 73.4° and 24.0°, indicating persistent DISI despite union. At 11 months after surgery, plain radiographs demonstrated union without loss of alignment or hardware failure (Fig. 2). Final wrist volar flexion/dorsiflexion was 70°/60°, grip strength was 34.5 kg (82% of the contralateral side), VAS pain score was 0, DASH score was 9.09, and the patient was very satisfied (Table 2).
Patient information and clinical findings
A 45-year-old male patient presented with chronic pain in the right wrist, which was his dominant side, after a remote wrist injury approximately 10 years earlier. His symptoms were most bothersome during wrist flexion and daily activities. He was a non-smoker and had no diabetes.
Diagnostic assessment
Plain radiographs demonstrated scaphoid nonunion with carpal malalignment, and CT confirmed proximal scaphoid nonunion with DISI deformity. Preoperative SL and RL angles were 59.3° and 15.3°, respectively. Preoperative gadolinium-enhanced MRI showed no evidence of AVN.
Therapeutic intervention
He underwent the same operative procedure, including dorsal cancellous bone graft harvest from the distal radius at the Lister tubercle and volar fixation with two 2.4-mm headless compression screws. The wrist was immobilized in a thumb-spica cast for 2 months, after which range-of-motion exercises were initiated.
Follow-up and outcomes
Postoperative CT obtained 7 weeks after surgery demonstrated maintained fixation and alignment. Immediate postoperative SL and RL angles were 62.2° and 9.7°, and final SL and RL angles were 60.3° and 12.4°. At 7 months after surgery, follow-up radiographs showed union without loss of alignment or hardware failure (Fig. 3). Final wrist volar flexion/dorsiflexion was 70°/50°, grip strength was 30.0 kg (85% of the contralateral side), VAS pain score was 1, DASH score was 13.63, and the patient was very satisfied (Table 2).
Patient information and clinical findings
A 41-year-old male patient presented with chronic pain in the left wrist, which was his non-dominant side. He had a remote history of wrist injury 10 to 20 years earlier and had reportedly been told at that time that no fracture was present. Persistent symptoms remained, and the pain worsened after a traffic accident while he was gripping the steering wheel. He was an ex-smoker and had no diabetes.
Diagnostic assessment
Plain radiographs demonstrated scaphoid nonunion with carpal malalignment, and CT confirmed proximal scaphoid nonunion with DISI deformity. Preoperative SL and RL angles were 59.4° and 18.5°, respectively. Preoperative nonenhanced MRI did not show definite AVN. On retrospective review, a small loose body adjacent to the scaphoid was identifiable on both preoperative radiographs and CT (Fig. 4B).
Therapeutic intervention
He also underwent the same operative procedure, including dorsal cancellous bone graft harvest from the distal radius at the Lister tubercle and volar fixation with two 2.4-mm headless compression screws. The wrist was immobilized in a thumb-spica cast for 2 months, after which range-of-motion exercises were initiated.
Follow-up and outcomes
Postoperative CT obtained 6 weeks after the index procedure demonstrated maintained screw position and alignment without definite joint penetration. Immediate postoperative SL and RL angles were 53.9° and 15.2°, and final SL and RL angles were 60.7° and 12.7°. During follow-up, persistent pain on wrist extension developed. Because the loose body had been present preoperatively and remained visible on follow-up imaging, and because irritation from one slightly long screw could not be excluded, secondary surgery was performed approximately 20 months after the index procedure. The loose body and one headless compression screw were removed; the exact pathological origin of the loose body was not confirmed. At 23 months after the index procedure, final follow-up radiographs demonstrated maintained union and alignment without fixation failure (Fig. 4). Final wrist volar flexion/dorsiflexion was 70°/60°, grip strength was 36.9 kg (94% of the contralateral side), VAS pain score was 0, DASH score was 9.17, and the patient was very satisfied (Table 2).
Discussion
This report describes three selected cases of proximal scaphoid nonunion with DISI deformity, without definite preoperative AVN, treated using dorsal distal-radius cancellous bone grafting and volar fixation with two 2.4-mm short-thread headless compression screws. The main observation is not that this technique reliably corrects DISI or is superior to single-screw fixation, but rather that dual-screw fixation was technically feasible in carefully selected proximal nonunions when preoperative CT suggested sufficient proximal fragment size and morphology, including enough depth for the 4-mm leading thread to cross the nonunion site and enough width to accommodate two safe screw trajectories. Radiographic union was observed in all three patients, and final patient-centered outcomes were favorable; however, carpal alignment correction was not uniform and one patient required secondary surgery.
The potential advantage of two screws is improved rotational control of the proximal fragment. This concept is supported by biomechanical data showing that a dual-screw construct may better maintain rotational stability than a single-screw construct, although stiffness and load-to-failure values may not differ significantly. Compared with Garcia et al. [9], the present report is more homogeneous in both pathology and technique. Garcia et al. [9] treated a heterogeneous group of scaphoid nonunions, only a minority of which involved the proximal third; among those proximal-third cases, most were approached dorsally, and most grafts in the overall series were harvested from the iliac crest. In contrast, all three patients in the present report had proximal scaphoid nonunion with DISI deformity and were managed with the same strategy: local cancellous graft harvested from the distal radius and distal-to-proximal dual short-thread screw fixation through a volar approach. This may represent the main technical distinction and clinical relevance of the present report.
A central concern is whether two 2.4-mm screws can be safely accommodated in a small proximal fragment and whether distal-to-proximal compression can be achieved when the nonunion line is very proximal. In our series, the proximal fragment measured 5.60 to 7.06 mm in width and 5.90 to 9.12 mm in depth on coronal CT, and 8.20 to 16.53 mm in width and 5.37 to 7.55 mm in depth on sagittal CT (Table 1). These measurements were obtained on the reconstructed CT cut in each plane on which the fragment appeared largest (Fig. 1). We used 2.4-mm short-thread screws and limited this technique to cases in which CT suggested that the 4-mm leading thread could cross the nonunion and engage the proximal fragment. However, because the proximal fragment is approximately dome-shaped, maximum-cut measurements do not guarantee that two screws will be securely engaged along their entire trajectories. Thus, the decision to use dual 2.4-mm screws was made qualitatively by integrating the measurements with fragment morphology, the proximal extent of the fracture line, possible parallel screw trajectories, the anticipated bone bridge between screws, and the distance from the articular surfaces. These criteria support the technical feasibility of compression in the present selected cases, but the safety margin remains narrow. Two 2.4-mm screws occupy substantial volume and require an adequate bone bridge between trajectories; therefore, this technique should not be generalized to all proximal pole nonunions. Smaller-diameter screws, alternative trajectories, single-screw fixation, vascularized grafting, or salvage procedures may be more appropriate when CT shows severe fragmentation, limited bone stock, insufficient proximal fragment depth for the leading thread to cross the nonunion site, or unsafe proximity to the articular surfaces.
The alignment data also requires cautious interpretation. Final RL angle decreased below the DISI threshold in case 2 and case 3, whereas DISI persisted in case 1 despite radiographic union and favorable symptoms. Therefore, the present cases do not prove that dual-screw fixation reliably corrects DISI. Rather, they suggest that volar reduction and dual-screw fixation may maintain acceptable alignment in selected cases, while complete correction is not guaranteed.
Bone graft selection was based on the expected defect morphology. Three-dimensional CT studies have shown that the defect pattern in scaphoid nonunion varies by location: waist or distal nonunion tends to create a larger volar-based wedge-shaped defect, whereas proximal nonunion more often leaves a flatter crescent-shaped defect localized around the fracture site [14]. This distinction helps explain why structural corticocancellous wedge grafting is intuitive in unstable waist nonunion with humpback collapse [15-17], yet may be less necessary in selected proximal nonunions. In the present cases, DISI correction was not obtained by wedge-graft mechanics, but rather by fluoroscopic reduction and maintenance with the screw construct; the cancellous graft was used primarily to fill the residual crescent-type cavity. Accordingly, cancellous graft was used as a biological filler rather than as a structural wedge, with part of the graft placed dorsally before screw insertion and the remaining volar defect packed after fixation. This rationale is supported by Cohen et al. [18], who reported successful treatment of scaphoid waist nonunion with humpback deformity without structural graft when stable screw fixation was obtained, and by Kim et al. [13], who found that cancellous grafting provided earlier union and similar deformity restoration and wrist function compared with corticocancellous grafting in unstable scaphoid nonunion treated with headless compression screw fixation. The dorsal Lister tubercle harvest was also practical in this setting because cancellous bone can be obtained easily through a small dorsal cortical window without disrupting the volar cortex or crowding the primary volar exposure used for reduction and screw placement.
The secondary procedure in case 3 deserves specific discussion. A small loose body adjacent to the scaphoid was retrospectively identifiable on both preoperative radiographs and CT, indicating that it was not necessarily caused by the dual-screw fixation procedure. CT obtained 6 weeks after the index procedure, before secondary surgery, showed maintained screw position without definite joint penetration. During follow-up, the patient developed persistent pain on wrist extension. Because the exact pain generator was uncertain and could have been related either to the preexisting loose body or to irritation from one slightly long screw, both the loose body and one screw were removed approximately 20 months after the index procedure. The loose body was not pathologically characterized. This case therefore should not be interpreted as definitive evidence of iatrogenic proximal fragment blowout or screw loosening inherent to dual-screw fixation. Nevertheless, it highlights the limited technical margin of this procedure and the importance of meticulous screw length selection, postoperative imaging review, and careful follow-up when extension pain persists.
The chronicity of nonunion varied widely among the three patients, from 8 months to 10–20 years. This heterogeneity may influence biology, deformity stiffness, cartilage status, and functional recovery, and it limits interpretation of the outcomes. Preoperative MRI was performed in all patients and did not show definite proximal-pole AVN. Therefore, our series does not address proximal nonunion with established AVN, in which vascularized grafting may be more strongly considered. Nevertheless, only one patient underwent gadolinium-enhanced MRI and intraoperative punctate bleeding was not systematically documented, so vascularity assessment remained limited.
This report has several limitations. It includes only three patients and represents a retrospective single-surgeon experience without a control group. The cases were selected based on fragment size, fragment depth, qualitative assessment of fragment morphology, and feasibility of two distal-to-proximal screw trajectories, which limits generalizability. Moreover, the fragment dimensions were measured on the CT cut in each plane in which the fragment appeared largest; therefore, these values may overestimate usable bone stock in the approximately dome-shaped proximal fragment and cannot guarantee secure purchase of both screws. Union was assessed on plain radiographs at final follow-up rather than uniformly confirmed by CT, which is a significant limitation in scaphoid nonunion research. Radioulnar deviation, preoperative VAS pain scores, and formal return-to-work or return-to-sport timing were not consistently available. Because all cases used 2.4-mm short-thread screws, this report cannot compare short-thread and long-thread designs or smaller screw options.
In conclusion, this small retrospective series suggests that volar dual 2.4-mm short-thread headless compression screw fixation combined with staged dorsal-to-volar distal-radius cancellous bone grafting is technically feasible for selected proximal scaphoid nonunions with concomitant DISI deformity when preoperative CT assessment suggests sufficient proximal fragment size, depth, and morphology for two safe distal-to-proximal screw trajectories. Although CT-confirmed union at final follow-up was not uniformly available, radiographic union defined on plain radiographs and favorable short-term functional outcomes were observed in all three patients. The DISI correction was not uniform and one patient required secondary surgery. Larger studies with standardized CT-based union assessment, functional outcome measures, and longer follow-up are needed to validate this technique.
-
Author contributions
Conceptualization: JKK. Data curation: SL, WSL. Formal analysis: SL, WSL. Investigation: SL, WSL. Methodology: JKK. Project administration: JKK. Visualization: SL, WSL. Writing–original draft preparation: SL. Writing–review & editing: SL, WSL, JKK. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
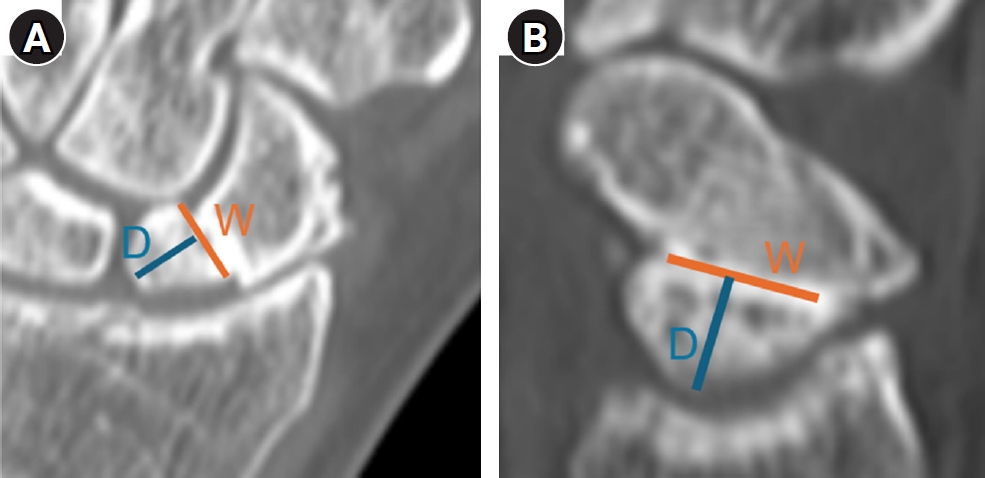
Computed tomography-based assessment of proximal fragment dimensions. (A) Width (W) and depth (D) measured on the reconstructed coronal image using the section in which the proximal fragment appeared longest. (B) Width (W) and depth (D) measured similarly on the reconstructed sagittal image using the section in which the proximal fragment appeared longest. Depth was defined as the distance from the nonunion line to the proximal subchondral boundary in the intended distal-to-proximal screw direction.
Fig. 2.
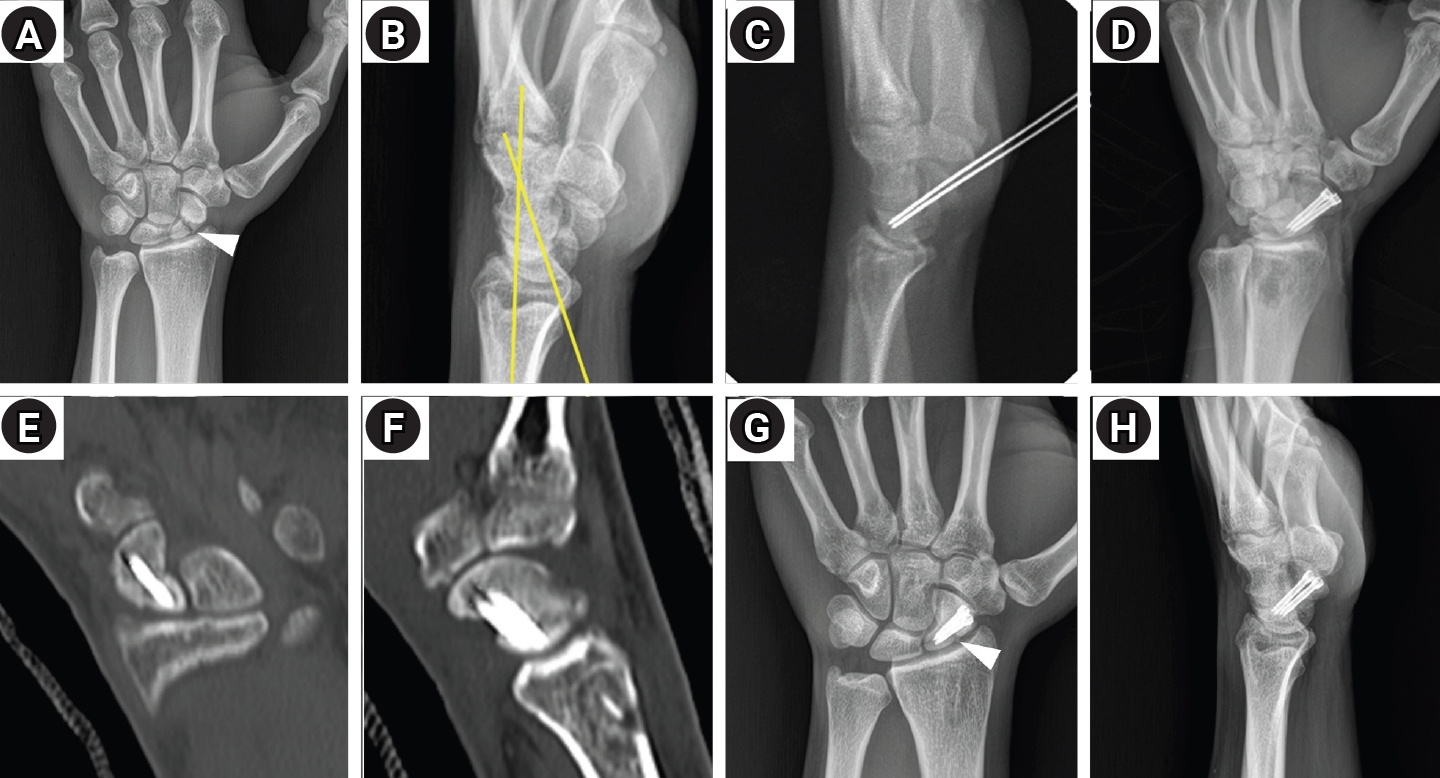
Imaging course of case 1. (A) Initial posteroanterior radiograph showing proximal scaphoid nonunion; the arrowhead indicates the fracture line. (B) Initial lateral radiograph demonstrating DISI deformity; the yellow lines indicate a radiolunate angle of 20.4°. (C, D) Intraoperative fluoroscopic images showing guidewire placement followed by dual 2.4-mm short-thread headless compression screw fixation through a volar approach. (E, F) Follow-up computed tomography obtained 7 weeks after surgery. Coronal and sagittal reconstructed images aligned with the scaphoid axis demonstrate satisfactory intraosseous positioning of the two 2.4-mm screws and adequate purchase of the proximal fragment. (G, H) Radiographs obtained 11 months after surgery show union without loss of alignment or hardware failure; the arrowhead in (G) indicates bridging callus at the nonunion site.
Fig. 3.
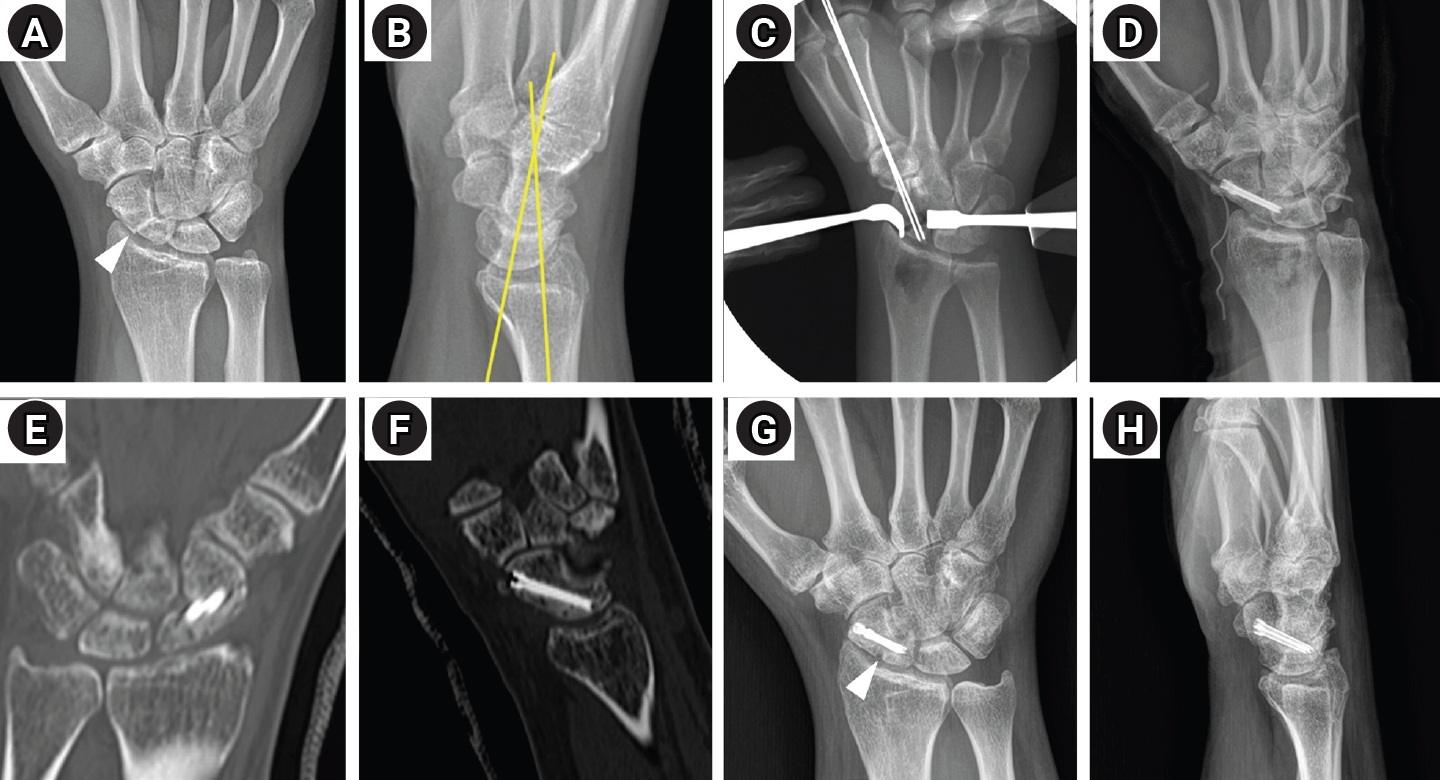
Imaging course of case 2. (A) Initial posteroanterior radiograph showing proximal scaphoid nonunion; the arrowhead indicates the fracture line. (B) Initial lateral radiograph demonstrating DISI deformity; the yellow lines indicate a radiolunate angle of 15.3°. (C, D) Intraoperative fluoroscopic images showing guidewire placement followed by dual 2.4-mm short-thread headless compression screw fixation through a volar approach. (E, F) Follow-up computed tomography obtained 7 weeks after surgery. Coronal and sagittal reconstructed images aligned with the scaphoid axis demonstrate satisfactory intraosseous positioning of the two 2.4-mm screws and adequate purchase of the proximal fragment. (G, H) Radiographs obtained 7 months after surgery show union without loss of alignment or hardware failure; the arrowhead in (G) indicates bridging callus at the nonunion site.
Fig. 4.
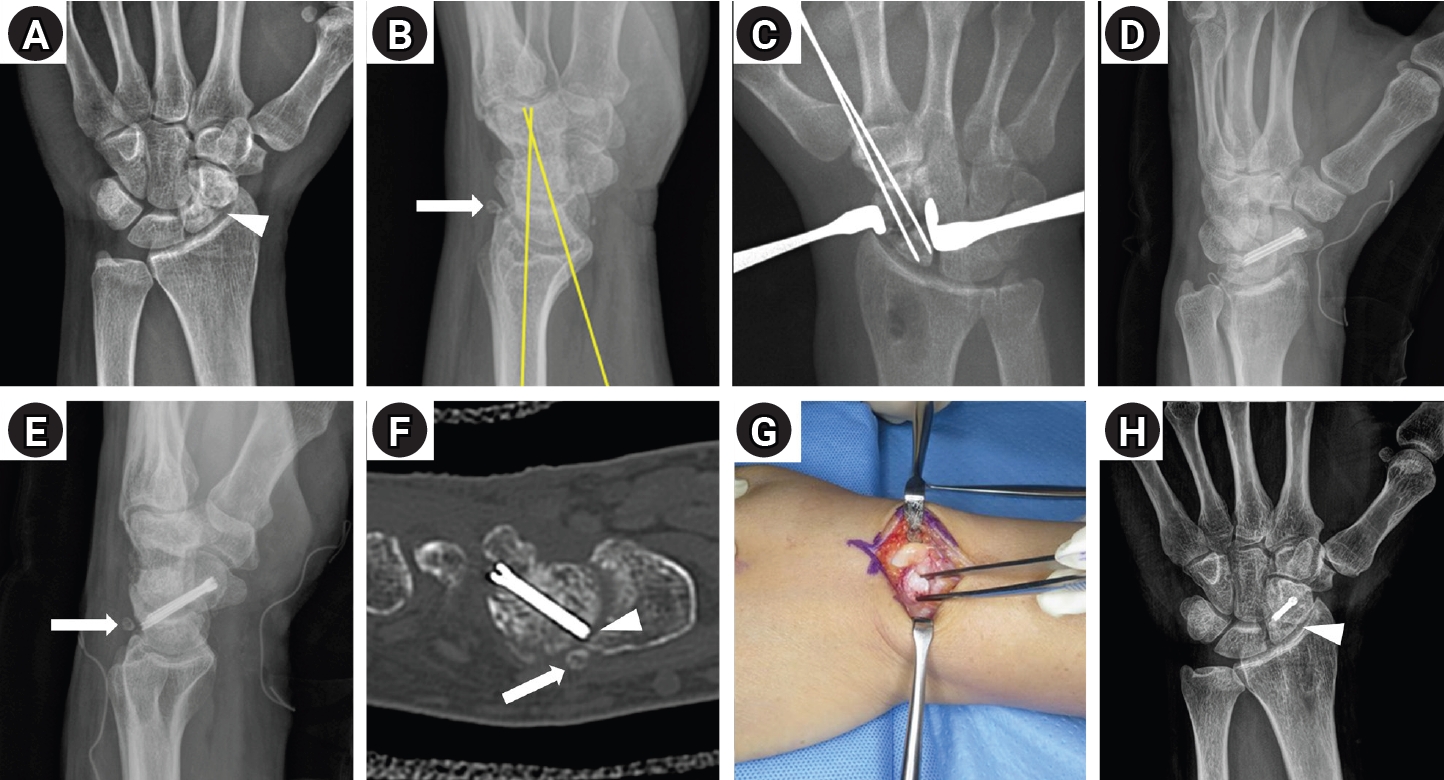
Imaging course of case 3. (A) Initial posteroanterior radiograph showing proximal scaphoid nonunion; the arrowhead indicates the fracture line. (B) Initial lateral radiograph demonstrating DISI deformity; the yellow lines indicate a radiolunate angle of 18.5°, and the arrow indicates a loose body at the dorsal aspect of the scaphoid. (C, D) Intraoperative fluoroscopic images showing guidewire placement followed by dual 2.4-mm short-thread headless compression screw fixation through a volar approach. (E) Follow-up lateral radiograph obtained before secondary surgery showing the loose body near the dorsal aspect of the scaphoid (arrow). (F) Follow-up computed tomography obtained 6 weeks after the index procedure demonstrates satisfactory intraosseous screw positioning without definite joint penetration; the arrow indicates the loose body, and the arrowhead indicates the tip of a slightly long screw. (G) Intraoperative image obtained during secondary surgery showing removal of the loose body. (H) Final follow-up radiograph after secondary surgery demonstrates maintained union and alignment without fixation failure; the arrowhead indicates bridging callus at the nonunion site.
Table 1.
Demographic and radiographic characteristics of the three cases
Table 2.
Final outcomes of the three cases
- 1. Large TM, Adams MR, Loeffler BJ, Gardner MJ. Posttraumatic avascular necrosis after proximal femur, proximal humerus, talar neck, and scaphoid fractures. J Am Acad Orthop Surg 2019;27:794-805.ArticlePubMed
- 2. de Roo MG, Dobbe JG, van der Horst CM, Streekstra GJ, Strackee SD. Carpal kinematic changes after scaphoid nonunion: an in vivo study with four-dimensional CT imaging. J Hand Surg Eur Vol 2019;44:1056-64.ArticlePubMedPMCPDF
- 3. Alanen M, Aspinen S, Höglund T, Sippo R, Waris E. Computer-aided three-dimensional analysis of carpal alignment in scaphoid nonunion advanced collapse wrists: a comparative study with scapholunate advanced collapse and healthy wrists. BMC Musculoskelet Disord 2025;26:423.ArticlePubMedPMCPDF
- 4. Newport ML, Williams CD, Bradley WD. Mechanical strength of scaphoid fixation. J Hand Surg Br 1996;21:99-102.ArticlePubMedPDF
- 5. Trumble TE, Clarke T, Kreder HJ. Non-union of the scaphoid: treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am 1996;78:1829-37.ArticlePubMed
- 6. Manske PR, McCarthy JA, Strecker WB. Use of the Herbert bone screw for scaphoid nonunions. Orthopedics 1988;11:1653-61.ArticlePubMed
- 7. Kobayashi M, Berger RA, Nagy L, et al. Normal kinematics of carpal bones: a three-dimensional analysis of carpal bone motion relative to the radius. J Biomech 1997;30:787-93.ArticlePubMed
- 8. Nicholson LT, Sochol KM, Azad A, Alluri RK, Hill JR, Ghiassi A. Single versus dual headless compression screw fixation of scaphoid nonunions: a biomechanical comparison. Hand (N Y) 2022;17:1122-7.ArticlePubMedPDF
- 9. Garcia RM, Leversedge FJ, Aldridge JM, Richard MJ, Ruch DS. Scaphoid nonunions treated with 2 headless compression screws and bone grafting. J Hand Surg Am 2014;39:1301-7.ArticlePubMed
- 10. Moritomo H, Viegas SF, Elder KW, et al. Scaphoid nonunions: a 3-dimensional analysis of patterns of deformity. J Hand Surg Am 2000;25:520-8.ArticlePubMed
- 11. Braun NS, Berger RA, Wolfe SW. Defining DISI and VISI. J Hand Surg Eur Vol 2021;46:566-8.ArticlePubMedPDF
- 12. Rodriguez-Fontan F, Tucker NJ, Pflug EM, Leversedge FJ, Catalano LW, Lauder A. Proximal hamate reconstruction of proximal pole scaphoid nonunion: a case series and analysis of clinical outcomes. Hand (N Y) 2024;19:967-77.ArticlePubMedPDF
- 13. Kim JK, Yoon JO, Baek H. Corticocancellous bone graft vs cancellous bone graft for the management of unstable scaphoid nonunion. Orthop Traumatol Surg Res 2018;104:115-20.ArticlePubMed
- 14. Oka K, Murase T, Moritomo H, Goto A, Sugamoto K, Yoshikawa H. Patterns of bone defect in scaphoid nonunion: a 3-dimensional and quantitative analysis. J Hand Surg Am 2005;30:359-65.ArticlePubMed
- 15. Tomaino MM, King J, Pizillo M. Correction of lunate malalignment when bone grafting scaphoid nonunion with humpback deformity: rationale and results of a technique revisited. J Hand Surg Am 2000;25:322-9.ArticlePubMed
- 16. Bindra R, Bednar M, Light T. Volar wedge grafting for scaphoid nonunion with collapse. J Hand Surg Am 2008;33:974-9.ArticlePubMed
- 17. Fernandez DL. A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-7.ArticlePubMed
- 18. Cohen MS, Jupiter JB, Fallahi K, Shukla SK. Scaphoid waist nonunion with humpback deformity treated without structural bone graft. J Hand Surg Am 2013;38:701-5.ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteFixation with two headless compression screws and a distal-radius bone graft for proximal scaphoid nonunion with dorsal intercalated segment instability deformity: a report of three cases
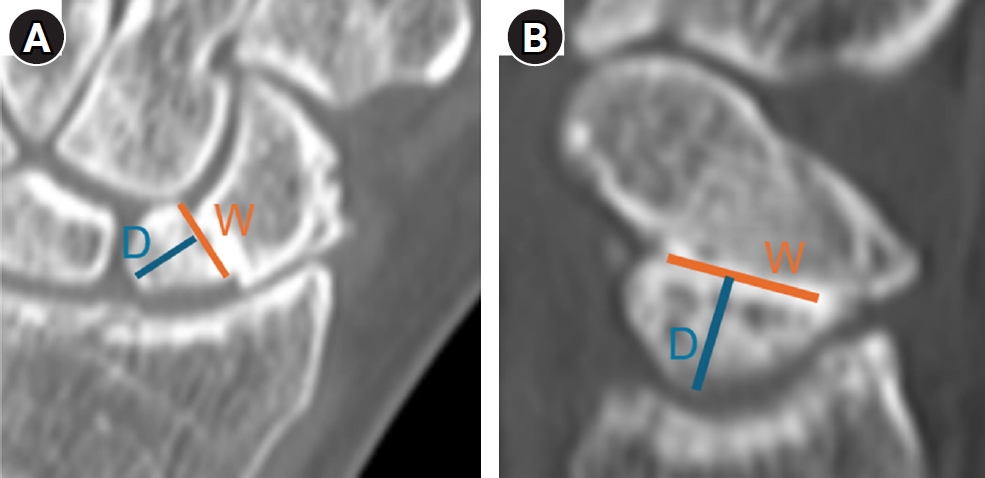
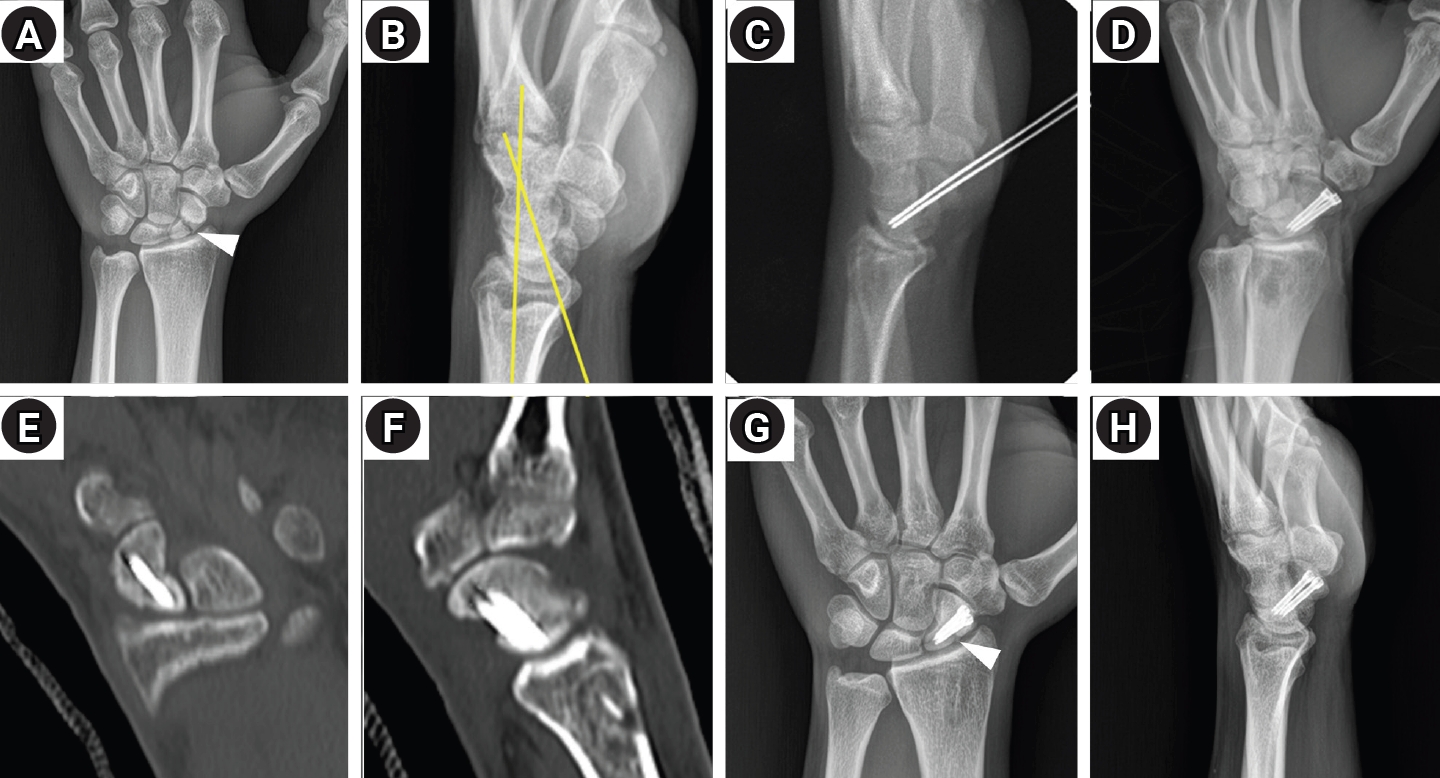
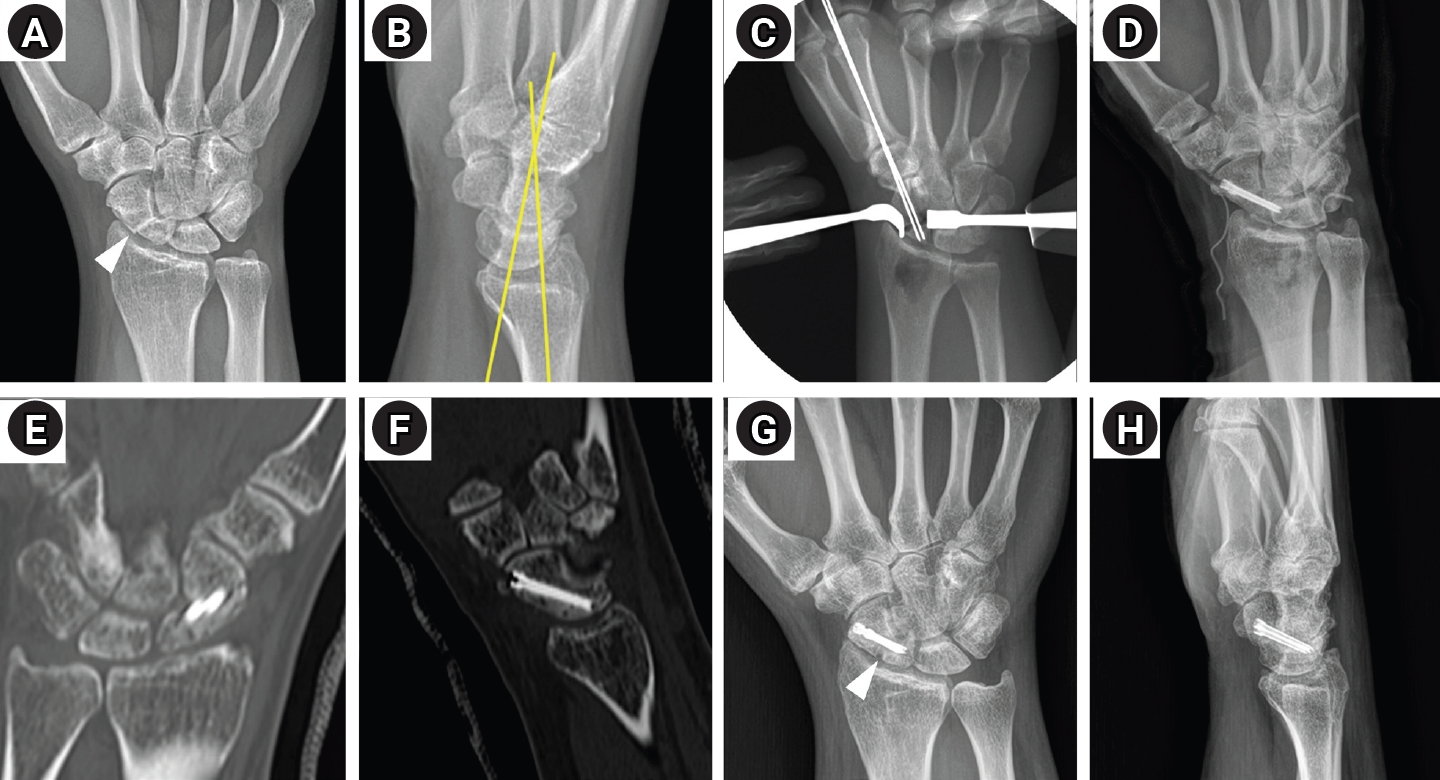
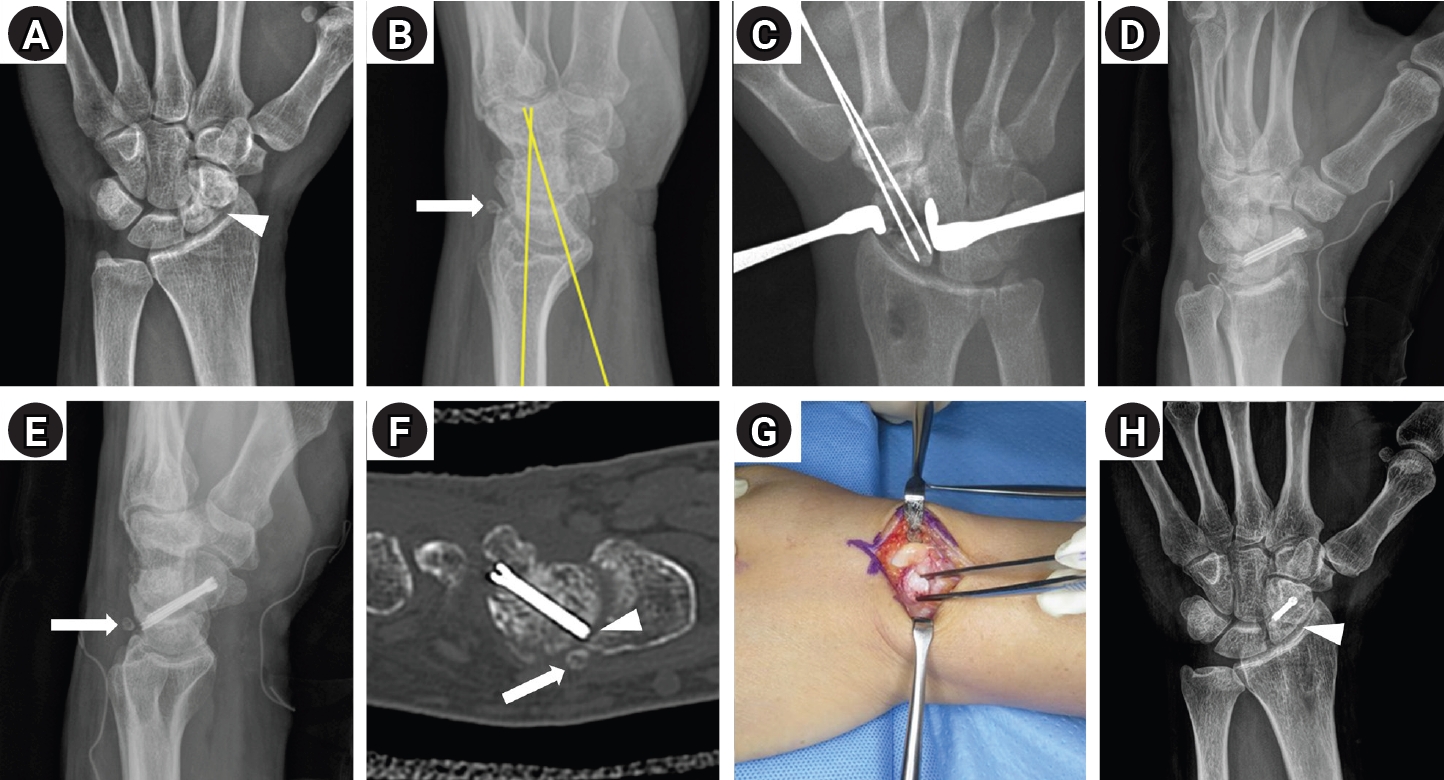
Fig. 1. Computed tomography-based assessment of proximal fragment dimensions. (A) Width (W) and depth (D) measured on the reconstructed coronal image using the section in which the proximal fragment appeared longest. (B) Width (W) and depth (D) measured similarly on the reconstructed sagittal image using the section in which the proximal fragment appeared longest. Depth was defined as the distance from the nonunion line to the proximal subchondral boundary in the intended distal-to-proximal screw direction.
Fig. 2. Imaging course of case 1. (A) Initial posteroanterior radiograph showing proximal scaphoid nonunion; the arrowhead indicates the fracture line. (B) Initial lateral radiograph demonstrating DISI deformity; the yellow lines indicate a radiolunate angle of 20.4°. (C, D) Intraoperative fluoroscopic images showing guidewire placement followed by dual 2.4-mm short-thread headless compression screw fixation through a volar approach. (E, F) Follow-up computed tomography obtained 7 weeks after surgery. Coronal and sagittal reconstructed images aligned with the scaphoid axis demonstrate satisfactory intraosseous positioning of the two 2.4-mm screws and adequate purchase of the proximal fragment. (G, H) Radiographs obtained 11 months after surgery show union without loss of alignment or hardware failure; the arrowhead in (G) indicates bridging callus at the nonunion site.
Fig. 3. Imaging course of case 2. (A) Initial posteroanterior radiograph showing proximal scaphoid nonunion; the arrowhead indicates the fracture line. (B) Initial lateral radiograph demonstrating DISI deformity; the yellow lines indicate a radiolunate angle of 15.3°. (C, D) Intraoperative fluoroscopic images showing guidewire placement followed by dual 2.4-mm short-thread headless compression screw fixation through a volar approach. (E, F) Follow-up computed tomography obtained 7 weeks after surgery. Coronal and sagittal reconstructed images aligned with the scaphoid axis demonstrate satisfactory intraosseous positioning of the two 2.4-mm screws and adequate purchase of the proximal fragment. (G, H) Radiographs obtained 7 months after surgery show union without loss of alignment or hardware failure; the arrowhead in (G) indicates bridging callus at the nonunion site.
Fig. 4. Imaging course of case 3. (A) Initial posteroanterior radiograph showing proximal scaphoid nonunion; the arrowhead indicates the fracture line. (B) Initial lateral radiograph demonstrating DISI deformity; the yellow lines indicate a radiolunate angle of 18.5°, and the arrow indicates a loose body at the dorsal aspect of the scaphoid. (C, D) Intraoperative fluoroscopic images showing guidewire placement followed by dual 2.4-mm short-thread headless compression screw fixation through a volar approach. (E) Follow-up lateral radiograph obtained before secondary surgery showing the loose body near the dorsal aspect of the scaphoid (arrow). (F) Follow-up computed tomography obtained 6 weeks after the index procedure demonstrates satisfactory intraosseous screw positioning without definite joint penetration; the arrow indicates the loose body, and the arrowhead indicates the tip of a slightly long screw. (G) Intraoperative image obtained during secondary surgery showing removal of the loose body. (H) Final follow-up radiograph after secondary surgery demonstrates maintained union and alignment without fixation failure; the arrowhead indicates bridging callus at the nonunion site.
Fig. 1.
Fig. 2.
Fig. 3.
Fig. 4.
Fixation with two headless compression screws and a distal-radius bone graft for proximal scaphoid nonunion with dorsal intercalated segment instability deformity: a report of three cases
| Case | Age/sex | Side/dominance | Smoking | Injury-to-surgery interval | MRI/AVN assessment | Proximal fragment size (coronal width/depth, mm) | Proximal fragment size (sagittal width/depth, mm) | Preop SL/RL (°) | Immediate postop SL/RL (°) | Final F/U SL/RL (°) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 23/male | Left/non-dominant | Current smoker (2 pack-years) | 8 mo | Nonenhanced MRI; no AVN | 5.6/5.9 | 8.2/5.37 | 73.6/20.4 | 74.6/23.7 | 73.4/24.0 |
| 2 | 45/male | Right/dominant | Non-smoker | approximately 10 yr | Gd-enhanced MRI; no AVN | 6.49/6.18 | 11.23/6.01 | 59.3/15.3 | 62.2/9.7 | 60.3/12.4 |
| 3 | 41/male | Left/non-dominant | Ex-smoker | 10-20 yr | Nonenhanced MRI; no AVN | 7.06/9.12 | 16.53/7.55 | 59.4/18.5 | 53.9/15.2 | 60.7/12.7 |
| Case | Latest F/U (mo) | Time to union (wk) | Final ROM VF/DF (°) | Final grip strength kg (% contra) | Final VAS | Final DASH | Patient satisfaction | Complication |
|---|---|---|---|---|---|---|---|---|
| 1 | 11 | 12 | 70/60 | 34.5 (82) | 0 | 9.09 | Very satisfied | None |
| 2 | 7 | 12 | 70/50 | 30.0 (85) | 1 | 13.63 | Very satisfied | None |
| 3 | 23 | 12 | 70/60 | 36.9 (94) | 0 | 9.17 | Very satisfied | Secondary removal of a preexisting loose body and one screw at 20 mo |
Table 1. Demographic and radiographic characteristics of the three cases
MRI, magnetic resonance imaging; AVN, avascular necrosis; SL, scapholunate; RL, radiolunate; Preop, preoperative; postop, postoperative; F/U, follow-up; Gd, gadolinium. Enhanced MRI indicates whether gadolinium-enhanced MRI was obtained.
Table 2. Final outcomes of the three cases
F/U, follow-up; VF, volar flexion; DF, dorsiflexion; contra, contralateral side; VAS, visual analog scale; DASH, Disabilities of the Arm, Shoulder and Hand.

