 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 39(2); 2026 > Article
-
Original Article
- Clinical and radiographic outcomes of elastic stable intramedullary nailing for pediatric humeral shaft fractures: a retrospective case series
-
Kang-San Lee1,2
 , Dongju Shin1, Sang Hee Kim1, Il Seo1, Tae-Hoon Kim1, Sung Jung Kim1
, Dongju Shin1, Sang Hee Kim1, Il Seo1, Tae-Hoon Kim1, Sung Jung Kim1 -
Journal of Musculoskeletal Trauma 2026;39(2):156-161.
DOI: https://doi.org/10.12671/jmt.2025.00381
Published online: March 10, 2026
1W Institute for Orthopedic Trauma and Joint Surgery, W General Hospital, Daegu, Korea
2Daegu Top Union Orthopedic Surgery Clinic, Daegu, Korea
- Correspondence to: Sung Jung Kim W Institute for Orthopedic Trauma and Joint Surgery, W General Hospital, 1632, Dalgubeol-daero, Dalse-gu, Daegu 42642, Korea Tel: +82-53-522-5561 Email: os1947@msn.com
• Received: December 4, 2025 • Revised: January 20, 2026 • Accepted: January 23, 2026
© 2026 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 470 Views
- 19 Download
Abstract
-
Background Pediatric humeral shaft fractures are uncommon and are generally treated conservatively, with satisfactory clinical outcomes reported in most cases. However, conservative management often necessitates prolonged immobilization and frequent outpatient follow-up visits, and it carries an inherent risk of residual angular or translational deformity. Elastic stable intramedullary nailing (ESIN) provides a simple and minimally invasive method of fracture fixation that offers adequate stability without disrupting the periosteal blood supply, thereby permitting early mobilization and promoting rapid bone union. The purpose of this study was to evaluate the clinical and radiological outcomes of ESIN fixation in pediatric patients with humeral shaft fractures.
-
Methods The medical records of pediatric patients with humeral shaft fractures who underwent ESIN fixation between January 2015 and November 2025 were retrospectively reviewed. Data collected included patient demographics, mechanism of injury, fracture location, number of elastic nails used, time to union, degree of residual angulation, range of motion (ROM), and postoperative complications.
-
Results The mean age of the patients was 10.0 years (range, 7 to 15 years). The mean time to radiographic union was 5.4 weeks (range, 2.4 to 10.4 weeks). The mean coronal angulation was 0.2° (range, −9.1° to 5.8°), while the mean sagittal angulation was −1.3° (range, −6.9° to 5.3°). No cases of infection, nerve injury, or nail migration were observed during the follow-up period. At the final follow-up assessment, all patients demonstrated full shoulder and elbow ROM, with no residual deformity or pain reported.
-
Conclusions In this small retrospective case series, ESIN fixation resulted in favorable union rates and excellent functional outcomes in pediatric humeral shaft fractures.
-
Level of evidence IV.
Introduction
Pediatric humeral shaft fractures are relatively uncommon injuries, accounting for approximately 2%–5% of all long-bone fractures in children [1,2]. Most cases can be successfully managed with conservative treatment such as functional bracing or cast immobilization, given the strong remodeling potential of the growing bone [3]. However, prolonged immobilization often causes discomfort, requires frequent outpatient follow-ups, and carries a risk of angular or translational deformity, particularly in older children and adolescents [4].
Elastic stable intramedullary nailing (ESIN) has become an established minimally invasive fixation technique for pediatric long-bone fractures [5,6]. This method provides stable fixation without disrupting the periosteal blood supply, allowing early joint motion and reliable bone union [7]. While ESIN has been successfully reported in several Asian studies, clinical series focusing on its role in achieving early mobilization and minimizing the burden of prolonged immobilization in this population remain limited [5].
The purpose of this study was to evaluate the clinical and radiologic outcomes of ESIN for pediatric humeral shaft fractures, with particular focus on its potential for rapid functional recovery, based on our institutional experience.
Methods
We conducted this study in compliance with the principles of the Declaration of Helsinki. Ethical approval for this study was obtained from the Public Institutional Review Board (PIRB) via the e-IRB system of the Ministry of Health and Welfare, Republic of Korea. The requirement for informed consent was waived due to the retrospective nature of the study (IRB No. P01-202512-01-001).
This study is a retrospective, single-center case series.
This study was conducted at W Institute for Orthopedic Trauma and Joint Surgery, W General Hospital (Daegu, Korea). The medical records of patients aged under 18 years who underwent surgical treatment for humeral shaft fractures at our institution between January 2015 and November 2025 were retrospectively reviewed.
Patients were followed postoperatively through scheduled outpatient visits, with radiographic and clinical assessment of union typically performed at weekly intervals until healing criteria were met. Final outcomes were assessed at the last follow-up visit.
The surgical indications at this institution included displaced humeral shaft fractures with angulation exceeding age-dependent limits (≥30° in children <10 years, ≥20° in older children), or unstable alignment after closed reduction. Other indications included open fractures, polytrauma, and associated nerve injury.
All surgeries were performed by orthopedic surgeons specializing in pediatric or upper extremity trauma. Anesthesia was administered as either brachial plexus block or general anesthesia, depending on the patient’s age and level of cooperation. The patient was placed in a supine position on a radiolucent table with the injured arm draped free, and fluoroscopy was used throughout the procedure.
A posterior entry technique through the distal humeral cortex was used in all cases. A small longitudinal incision was made over the posterior aspect of the distal humerus just proximal to the olecranon fossa. The triceps muscle was bluntly split to expose the posterior cortex, and an awl was used under fluoroscopic guidance to create the entry portal into the medullary canal (Fig. 1).
A single or double prebent titanium elastic nail (diameter, 2.0–3.0 mm) was chosen, with a diameter approximately one-third of the narrowest portion of the medullary canal [8]. In smaller humeri, the available canal diameter and posterior entry approach sometimes limited the maximal nail size, so a single nail was used to avoid excessive force during insertion. When the canal width allowed, two nails were inserted to achieve optimal end-point divergence and three-point elastic fixation. Proper alignment and rotational stability were confirmed under fluoroscopic control. After satisfactory reduction and fixation were achieved, the nail was cut and impacted beneath the posterior cortex to prevent soft-tissue irritation. Postoperatively, the arm was supported in a simple sling for comfort. Early gentle shoulder and elbow motion was initiated within the first postoperative week, and full range of motion (ROM) was allowed once radiographic callus formation was evident. All implants were removed after radiologic union was achieved (Fig. 2).
During the study period, a total of seven patients aged under 18 years underwent surgical treatment for humeral shaft fractures at our institution. Among them, two patients were treated with plate fixation due to distal shaft fracture location, which limited the feasibility of achieving stable fixation with ESIN, and were therefore excluded from the analysis. The remaining five patients who underwent ESIN were included in this study.
Medical records and radiographs provided patient age/sex, injury mechanism, and fracture site. Surgical variables included details like elastic nail count. Primary radiologic outcome variables were bone union time, removal time, follow-up time, and final follow-up angulation (coronal/sagittal planes). Clinical outcome variables were shoulder/elbow range of motion or ROM, residual pain, and complications.
Data were from the electronic medical records of this hospital. Radiologic assessments included bone union and postoperative angulation in both the coronal (varus/valgus) and sagittal (anterior/posterior) planes on anteroposterior and lateral radiographs, measured at the final follow-up. Positive values were defined as valgus or anterior angulation, whereas negative values indicated varus or posterior angulation. Bone union was defined as the earliest appearance of bridging callus formation on at least three cortices on radiographs, accompanied by the absence of tenderness at the fracture site. Union time was recorded at the postoperative visit (typically at weekly intervals) when these radiographic and clinical criteria were first met. Implant removal was scheduled once union was achieved; however, the exact timing varied depending on each patient’s circumstances, such as school schedule and outpatient availability. Clinical results were evaluated based on shoulder and elbow ROM, residual pain, and complications such as nonunion, infection, nail migration, or reoperation.
Because this was a retrospective case series of surgically treated patients, selection bias and confounding by indication are possible; operative treatment was chosen based on fracture characteristics and clinical considerations at the institution. To reduce selection bias within the ESIN cohort, we included consecutive pediatric humeral shaft fracture cases treated with ESIN during the study period and extracted variables using predefined radiographic and clinical criteria.
There was no sample size estimation.
Continuous variables were summarized using means and ranges. Given the small sample size, descriptive statistics were primarily used, and no inferential statistical analyses were performed. All statistical calculations were performed using IBM SPSS ver. 26.0 (IBM Corp.). There were no missing data in this study.
Results
A total of five patients (four males and one female; mean age, 10 years; range, 7–15 years) were included in the study (Table 1). The mechanisms of injury consisted of falls from height in one patient, a traffic accident in two, and a slip down in two. The mean follow-up period was 18.7 weeks (range, 11.1–25.9 weeks). The mean bone union time was 5.4 weeks (range, 2.4–10.4 weeks). At the final follow-up, the mean coronal (varus/valgus) angulation was 0.2° (range, –9.1° to 5.8°), and the mean sagittal (anterior/posterior) angulation was –1.3° (range, –6.9° to 5.3°) (Table 2).
No cases of infection, nerve injury, or nail migration were observed. At the final follow-up, all patients achieved full shoulder and elbow ROM without residual pain or deformity, and no patient required early implant removal due to irritation or discomfort.
Discussion
This study demonstrated that ESIN provided consistent bone union and favorable functional outcomes in most pediatric humeral shaft fractures. The technique offers several advantages, including minimal soft-tissue disruption, preservation of the periosteal blood supply, and the potential for early joint mobilization. All patients achieved solid bone union within an average of 5.4 weeks and regained full shoulder and elbow motion without pain or deformity. Notably, bridging callus formation was observed as early as 2.4 weeks in some cases, which may reflect the preserved periosteal blood supply.
Several studies have discussed the mechanical stability of flexible intramedullary nailing in long-bone fractures. Lascombes et al. [8] emphasized that the stability of elastic nailing depends on the ratio between nail diameter and the medullary canal width, suggesting that insufficient nail occupancy may reduce construct rigidity and lead to delayed union or loss of alignment. In addition, Johnson et al. [9] conducted a biomechanical study evaluating the influence of the nail’s length beyond the fracture site on overall construct stability. They reported that fixations extending less than two bone diameters beyond the fracture were grossly unstable, showing significantly reduced bending resistance and higher displacement under load. In contrast, fixations extending at least three diameters maintained sufficient stiffness and load-bearing capacity, highlighting the importance of adequate working length for stable fixation. Integrating these findings with the present study, adequate nail diameter and sufficient working length are essential to achieve stable fixation and prevent loss of alignment in pediatric humeral shaft fractures. However, it should be noted that these biomechanical principles are largely derived from studies on lower-extremity long bones, where greater nail occupancy is generally feasible.
In the pediatric humerus, the medullary canal is often substantially narrower, which may limit the ability to achieve the “adequate” nail diameter suggested by biomechanical studies. Despite this limitation, the present series demonstrated favorable alignment maintenance and union, which may be partly attributable to the lower mechanical loading demands of the upper extremity.
Although the present study did not directly compare ESIN with conservative treatment, previous literature has discussed differences in angular correction between the two approaches. In a comparative study between conservative and surgical treatment for pediatric humeral shaft fractures, Canavese et al. [3] reported better correction of angular deformity in the surgically treated group compared with the nonoperative group. In contrast, Hannonen et al. [10] demonstrated that even though surgical fixation for pediatric humeral shaft fractures has become more common in recent years, most cases still achieve satisfactory union and function with conservative management. Considering the generally accepted limits of angular deformity in nonoperative management (approximately 20°–30° in younger children and 15°–20° in older children), the present study demonstrated superior alignment correction, suggesting that ESIN can provide more reliable angular control while allowing early rehabilitation in carefully selected cases [10].
The retrospective design and small number of cases limit the generalizability of the findings, and statistical interpretation should be approached with caution. The follow-up duration was relatively short, precluding the evaluation of long-term functional or radiographic outcomes such as remodeling or residual deformity. Because no control group was available, direct comparison with conservative treatment or other fixation methods could not be made. Nevertheless, this study provides valuable insight into the practical indications and limitations of ESIN for pediatric humeral shaft fractures.
These findings support previous reports that ESIN provides stable fixation and predictable healing for humeral shaft fractures in skeletally immature patients.
In this small retrospective series, ESIN provided reliable alignment maintenance and favorable functional recovery, allowing early mobilization in appropriately selected pediatric humeral shaft fractures. While most fractures can be successfully managed nonoperatively, ESIN may serve as a useful surgical option when unacceptable angulation or instability persists after closed reduction. Larger comparative studies are warranted to further clarify its indications.
-
Author contributions
Conceptualization: DS, SJK. Data curation: KSL, SHK, IS. Formal analysis: THK. Investigation: KSL, IS. Methodology: KSL, SJK. Project administration: SJK. Visualization: KSL, SHK. Writing-original draft: KSL. Writing-review & editing: all authors. All authors read and approved the final manuscript.
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Contact the corresponding author for data availability.
-
Acknowledgments
None.
-
Supplementary materials
None.
Article Information
Fig. 1.
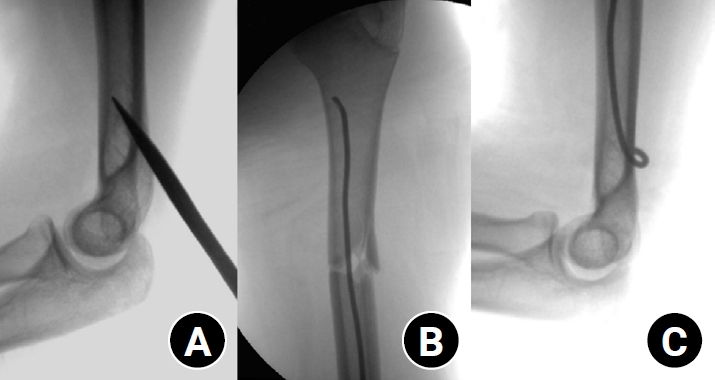
Intraoperative fluoroscopic images demonstrating the surgical technique of elastic stable intramedullary nailing for a pediatric humeral shaft fracture. (A) The entry point was created at the posterior cortex of the distal humerus using an awl under fluoroscopic guidance. (B) The prebent elastic nail was advanced across the fracture site under continuous fluoroscopic visualization. (C) The distal ends of the nails were contoured and buried subcutaneously to minimize soft-tissue irritation.
Fig. 2.
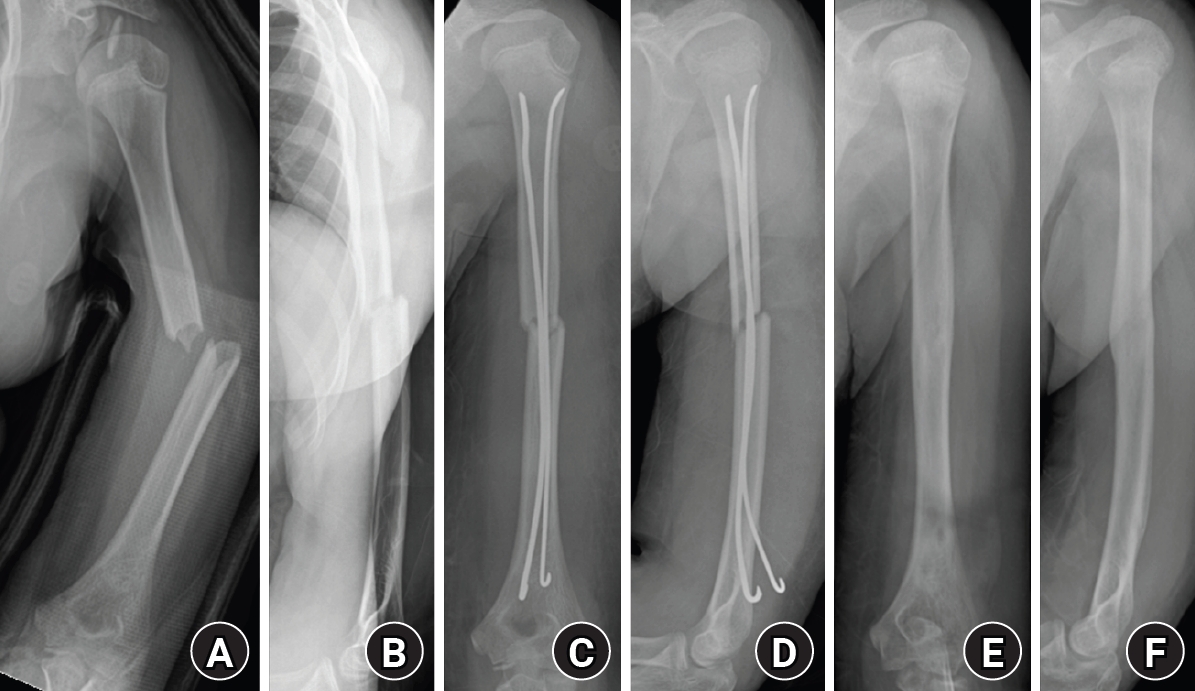
Radiographs of a representative case demonstrating successful bone healing following elastic stable intramedullary nailing fixation. (A, B) Preoperative anteroposterior and lateral radiographs showing a midshaft humeral fracture. (C, D) Immediate postoperative radiographs demonstrating satisfactory fracture alignment and stable fixation with elastic nails. (E, F) Follow-up radiographs obtained after implant removal showing complete bone union and restoration of normal humeral alignment.
Table 1.
Demographic, clinical, and radiologic characteristics of patients
Table 2.
Radiologic outcomes
| Variable | Mean (range) |
|---|---|
| Union time (wk, n=5) | 5.4 (2.4 to 10.4) |
| Coronal angulation (°) | 0.2 (–9.1 to 5.8) |
| Sagittal angulation (°) | –1.3 (–6.9 to 5.3) |
- 1. Caviglia H, Garrido CP, Palazzi FF, Meana NV. Pediatric fractures of the humerus. Clin Orthop Relat Res 2005;432:49-56.Article
- 2. O'Shaughnessy MA, Parry JA, Liu H, Stans AA, Larson AN, Milbrandt TA. Management of paediatric humeral shaft fractures and associated nerve palsy. J Child Orthop 2019;13:508-15.ArticlePubMedPMCPDF
- 3. Canavese F, Marengo L, Cravino M, et al. Outcome of conservative versus surgical treatment of humeral shaft fracture in children and adolescents: comparison between nonoperative treatment (Desault's bandage), external fixation and elastic stable intramedullary nailing. J Pediatr Orthop 2017;37:e156-63.ArticlePubMed
- 4. van de Wall BJ, Ochen Y, Beeres FJ, et al. Conservative vs. operative treatment for humeral shaft fractures: a meta-analysis and systematic review of randomized clinical trials and observational studies. J Shoulder Elbow Surg 2020;29:1493-504.ArticlePubMed
- 5. Li J, Wu J, Zhang Y, et al. Elastic stable intramedullary nailing for pediatric humeral shaft fractures under ultrasonographic guidance: a retrospective study. Front Pediatr 2021;9:806100.ArticlePubMed
- 6. Marengo L, Nasto LA, Michelis MB, Boero S. Elastic stable intramedullary nailing (ESIN) in paediatric femur and tibia shaft fractures: comparison between titanium and stainless steel nails. Injury 2018;49 Suppl 3:S8-11.ArticlePubMed
- 7. Annabell L, Shore BJ, Hedequist DJ, Hogue GD. Evaluation and management of pediatric humeral shaft fractures. J Am Acad Orthop Surg 2023;31:265-73.ArticlePubMed
- 8. Lascombes P, Haumont T, Journeau P. Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-34.ArticlePubMed
- 9. Johnson CW, Carmichael KD, Morris RP, Gilmer B. Biomechanical study of flexible intramedullary nails. J Pediatr Orthop 2009;29:44-8.Article
- 10. Hannonen J, Sassi E, Hyvönen H, Sinikumpu JJ. A shift from non-operative care to surgical fixation of pediatric humeral shaft fractures even though their severity has not changed. Front Pediatr 2020;8:580272.ArticlePubMedPMC
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteClinical and radiographic outcomes of elastic stable intramedullary nailing for pediatric humeral shaft fractures: a retrospective case series
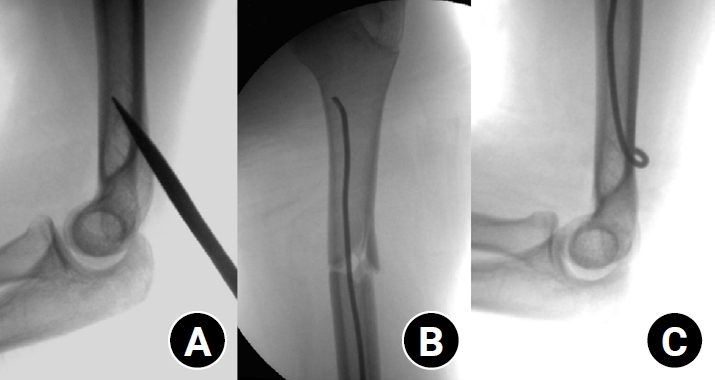
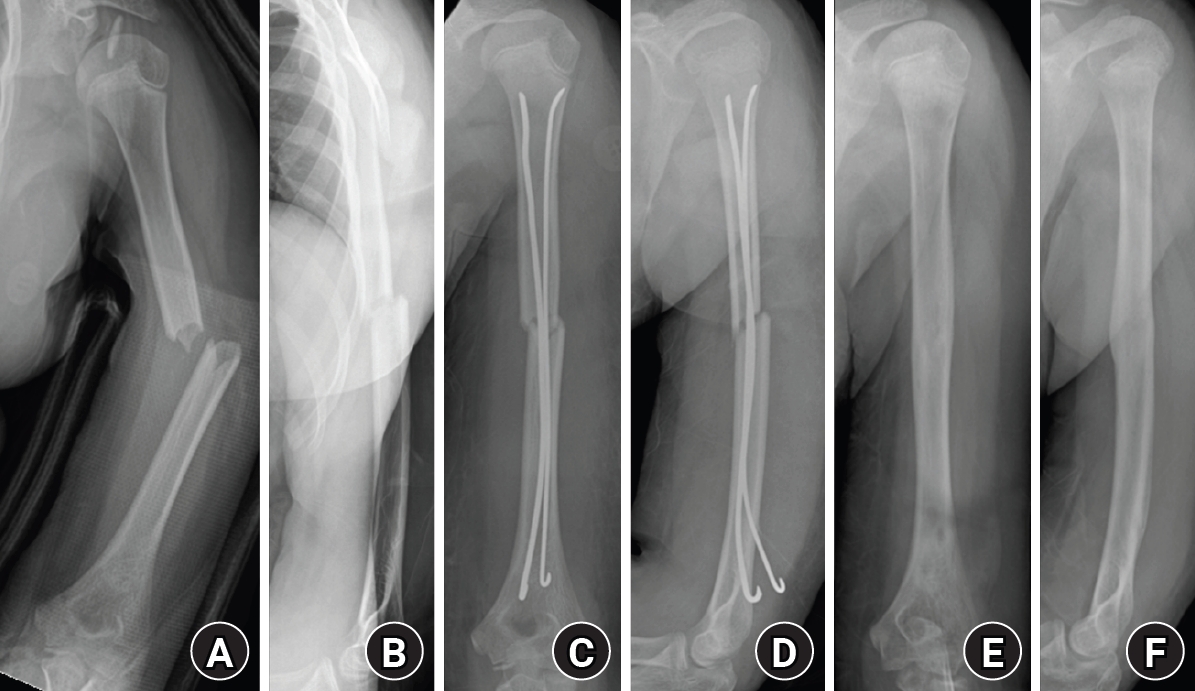
Fig. 1. Intraoperative fluoroscopic images demonstrating the surgical technique of elastic stable intramedullary nailing for a pediatric humeral shaft fracture. (A) The entry point was created at the posterior cortex of the distal humerus using an awl under fluoroscopic guidance. (B) The prebent elastic nail was advanced across the fracture site under continuous fluoroscopic visualization. (C) The distal ends of the nails were contoured and buried subcutaneously to minimize soft-tissue irritation.
Fig. 2. Radiographs of a representative case demonstrating successful bone healing following elastic stable intramedullary nailing fixation. (A, B) Preoperative anteroposterior and lateral radiographs showing a midshaft humeral fracture. (C, D) Immediate postoperative radiographs demonstrating satisfactory fracture alignment and stable fixation with elastic nails. (E, F) Follow-up radiographs obtained after implant removal showing complete bone union and restoration of normal humeral alignment.
Fig. 1.
Fig. 2.
Clinical and radiographic outcomes of elastic stable intramedullary nailing for pediatric humeral shaft fractures: a retrospective case series
| Case | Age (yr)/sex | Side | Mechanism of injury | Fracture site | No. of nails | Union time (wk) | Removal time (wk) | Follow-up time (wk) | Coronal angulation (°) | Sagittal angulation (°) | Final range of motion | Complication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 8/Male | Right | Slip down | Mid | 1 | 2.4 | 3.4 | 11.1 | 3.1 | 5.3 | Full | None |
| 2 | 15/Male | Left | Traffic accident | Mid | 1 | 3.2 | 6.4 | 20.6 | 5.8 | ‒2.5 | Full | None |
| 3 | 10/Male | Right | Traffic accident | Mid | 1 | 10.4 | 18.9 | 20.4 | ‒9.1 | ‒1.0 | Full | None |
| 4 | 7/Female | Right | Fall from height | Proximal | 1 | 3.4 | 3.6 | 15.7 | 0.8 | ‒1.2 | Full | None |
| 5 | 10/Male | Left | Slip down | Mid | 2 | 7.4 | 25.9 | 25.9 | 0.5 | ‒6.9 | Full | None |
| Variable | Mean (range) |
|---|---|
| Union time (wk, n=5) | 5.4 (2.4 to 10.4) |
| Coronal angulation (°) | 0.2 (–9.1 to 5.8) |
| Sagittal angulation (°) | –1.3 (–6.9 to 5.3) |
Table 1. Demographic, clinical, and radiologic characteristics of patients
Positive values indicate valgus or anterior angulation; negative values indicate varus or posterior angulation.
Table 2. Radiologic outcomes

