 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 38(4); 2025 > Article
-
Review Article
- Innovative applications of artificial intelligence in orthopedics focusing on fracture and trauma treatment: a narrative review
-
Chul-Ho Kim
 , Ji Wan Kim
, Ji Wan Kim -
Journal of Musculoskeletal Trauma 2025;38(4):178-185.
DOI: https://doi.org/10.12671/jmt.2025.00283
Published online: October 24, 2025
Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- Correspondence to: Ji Wan Kim Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43gil, Songpa-gu, Seoul 05505, Korea Tel: +82-2-3010-3530 Email: jaykim@amc.seoul.kr
• Received: August 14, 2025 • Accepted: September 4, 2025
© 2025 The Korean Orthopaedic Trauma Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,447 Views
- 36 Download
- 1 Crossref
Abstract
-
Artificial intelligence (AI) is bringing about transformative changes in orthopedic surgery, with its potential being particularly prominent in the field of fracture and trauma treatment. This review explores the current applications and future prospects of AI-driven surgical planning and simulation, robot and image-based navigation surgery, and image-assisted diagnostic technologies. Robotic assistance in orthopedic surgery, which was initially applied to improve accuracy in component implantation for knee and hip arthroplasty and to achieve high precision in spinal screw placement, has recently expanded its use to include accurate, minimally invasive reduction of pelvic fractures. In diagnostics, AI aids in the early prediction and classification of ambiguous fractures in various anatomical regions—for example, detecting shoulder or hip fractures, identifying incomplete atypical femur fractures, and classifying femoral neck fractures—through X-ray image analysis. This improves diagnostic accuracy and reduces medical costs. However, significant challenges remain, including high initial costs, steep learning curves, a lack of long-term studies, data bias, and ethical concerns. Continued research, interdisciplinary collaboration, and policy support are crucial for the widespread adoption of these technologies.Level of evidence: IV.
Introduction
Artificial intelligence (AI) is defined as the application of algorithms that provide machines with the ability to perform tasks traditionally requiring human intelligence, governed by pattern recognition and self-correction on large amounts of data to avoid errors [1]. The orthopedic field is rich with large datasets from digital medical imaging and registries, making it an ideal candidate for extensive AI applications, expanding its potential impact [1].
The influence of AI in orthopedics is already evident in diverse areas such as image recognition, risk prediction, and clinical decision-making [2]. Furthermore, in real surgical practice, conventional surgical methods are heavily reliant on the surgeon's experience and skill, which can lead to variability in outcomes. AI and robotic technologies hold the promise to overcome these limitations, enhancing surgical precision, enabling minimally invasive approaches, and accelerating patient recovery [3].
Looking ahead, the establishment of a fully integrated clinical pathway that leverages AI and robotics in orthopedic trauma is a development we can expect to see implemented in the near future (Fig. 1). This modern workflow, which can be described as 'The integrated pathway of AI and robotics in orthopedic trauma,' will represent a significant leap forward in patient treatment.
This review aims to systematically explore the current applications and innovative advancements of AI in orthopedic surgery, with a specific focus on fracture and trauma treatment.
This is a literature-based study; therefore, neither approval by an institutional review board nor informed consent is required
AI-driven surgical planning and robotic-assisted surgery
The utilization of robots in orthopedic surgery has been trialed since early stages [4], holding the potential for significant improvements in surgical planning, accuracy of component implantation, and patient safety. Robotic-assisted systems aid in enhancing the accuracy of preoperative planning and translating planned surgical steps into intraoperative execution (Fig. 2) [5].
In cases of unstable hip fracture, hip arthroplasty is sometimes favored over osteosynthesis. Particularly in elderly patients, those with poor bone quality, or when deformity is present, robotic-assisted hip arthroplasty can be especially beneficial.
In the late 1980s, the ROBODOC system was introduced in the United States. While not strictly a modern machine learning–based AI-assisted robotic system, it contributed to improved femoral component fit and positioning, as well as reduced limb length discrepancy in hip arthroplasty [6,7]. With the progressive development of AI technologies, the Mako robotic-arm assisted surgery system has become a valuable tool in hip surgery. In hip arthroplasty, it is particularly helpful for acetabular reaming and cup insertion. The Mako system (Stryker) uses computed tomography (CT) scans to generate patient-specific three-dimensional (3D) models for optimal implant placement planning, and its robotic arm provides haptic feedback to guide precise bone preparation.
When combined with minimally invasive surgery, the Mako system can achieve optimal synergy, allowing direct acetabular reaming to the planned cup size and accurate cup insertion. This enables shorter operative time and smaller incisions while minimizing damage to surrounding tissues.
In spine surgery, robots offer essential precision, especially for patients with complex deformities. The SpineAssist robot (Mazor Surgical Technologies) demonstrated remarkable accuracy in pedicle screw placement, with 96% of screws placed within 1 mm of their planned trajectory [8]. Robotic-assisted systems like TiRobot (TINAVI Medical Technologies) provide superior accuracy in percutaneous screw fixation for thoracolumbar fractures compared to manual placement [9]. Robots integrate preoperative and intraoperative imaging data, reducing the need for fluoroscopy and minimizing radiation exposure for both patients and medical staff [10,11]. Robotic guidance overcomes human physiological fatigue, ensuring high operative accuracy, good repeatability, and strong operational stability [12].
For fracture treatment, particularly complex cases like pelvic fractures, robotic-assisted systems are bringing about significant advancements [13-15]. The intelligent robot-assisted fracture reduction system intelligently designs the optimal reduction path and target position based on preoperative 3D CT scans, and a robotic arm autonomously reduces the affected hemipelvis according to this pre-planned path [13]. This system has enabled accurate and minimally invasive closed reduction for most patients with unstable pelvic fractures, achieving an average residual displacement of 6.65±3.59 mm and an excellent/good reduction rate of 85%. A significant advantage is zero radiation exposure for surgeons during the procedure. The Trauma Pod concept, a semi-automated telerobotic surgical system, also demonstrates future potential for surgical stabilization of critically wounded patients [16]. Robotic assistance has also been investigated for navigating entry points and distal locking bolts in intramedullary nailing [17,18], and for safe robot-assisted identification, dissection, and primary repair of nerves in brachial plexus surgery [19,20].
In addition to pelvic fractures, robot-assisted systems have demonstrated significant clinical benefits in treating intertrochanteric fractures in elderly patients [21,22]. Compared to traditional surgery, robot-assisted proximal femur nail antirotation surgery for unstable femoral intertrochanteric fractures results in a shorter operation time (62.3 minutes vs. 79.5 minutes) [22]. The robot’s precise navigation and positioning capabilities reduce the need for repeated manual adjustments and fluoroscopy, leading to a decrease in both intraoperative blood loss (86.8 mL vs. 148.0 mL) and perioperative hidden blood loss (504.7 mL vs. 744.2 mL). This also significantly lowers the rate of allogeneic blood transfusions. The enhanced precision of robot-assisted surgery also translates to faster patient recovery, with patients able to walk independently with crutches sooner (4.0 days vs. 5.2 days) and without crutches in less time (3.9 months vs. 5.1 months) [22]. Postoperative pain relief is quicker, and hip function scores are significantly higher one year after surgery (86.7 points vs. 82.7 points) [21].
Image-based assisted diagnostic technologies
AI is extensively applied in medical image analysis to enhance diagnostic accuracy and support clinical decision-making [23]. In orthopedics, AI is specifically used for fracture identification and classification, as well as nuanced grading of diseases [24-26].
Early prediction of fractures is crucial for patient prognosis. For incomplete atypical femoral fractures (AFFs), X-ray identification can be challenging, leading to delayed diagnosis and a risk of progression to complete fractures. To address this, an AI model called AFFnet has been developed using a deep convolutional neural network (CNN) to detect and classify AFFs from anteriorposterior radiographs [27]. This model was trained on a dataset including incomplete AFFs, complete AFFs, typical femoral fractures, and non-fractured femurs. AFFnet, which uses a novel Box Attention Guide module to direct its focus to key features, showed superior performance to a conventional model (ResNet-50). It achieved a sensitivity of 82% for detecting incomplete AFFs, which was higher than ResNet-50's 56%. This AI-based diagnostic tool has the potential to improve AFF detection, reduce radiologist error, and allow for urgent intervention to improve patient outcomes.
In upper extremity fractures, AI-based fracture detection is one of the most extensively studied and well-developed areas compared to other anatomical regions. In particular, for distal radius fractures, several commercialized AI programs have already been introduced, and their performance is reported to be excellent. Russe et al. [28] reported that the BoneView (Gleamer) program achieved a diagnostic accuracy exceeding 97% and a segmentation accuracy exceeding 94% in real-world clinical data for distal radius fractures. Similarly, in shoulder fractures, a recently developed AI model—an ensemble of Faster R-CNN (ResNet50-FPN, ResNeXt), EfficientDet, and RF-DETR—demonstrated outstanding performance, achieving a diagnostic accuracy of 96% and an F1-score of 0.961 [29].
The Garden classification for femoral neck fractures (FNFs) is a widely used system, but its reliability is a significant drawback [30,31]. To address this, a deep learning model was developed to detect and classify FNFs from plain radiographs [32]. This model, using Faster R-CNN and DenseNet-121, achieved a fracture detection accuracy of 94.1%. It also achieved high area under the curves for different Garden classifications: 0.94 for Garden I/II and 0.99 for Garden III/IV fractures. The model improved the diagnostic accuracy of emergency physicians from 86.3% to 92.0% and significantly enhanced the training outcomes of orthopedic trainees. The model's ability to provide a heatmap visualizing the probable fracture area further aids in diagnosis and physician training. This deep learning algorithm is a promising approach to improve fracture diagnosis and medical education without the costs and radiation of CT scans.
A systematic review of AI and machine learning for hip fracture diagnosis and classification found that AI models demonstrate high accuracy, often exceeding that of human clinicians alone [33]. Across 14 studies [34-47], AI's diagnostic accuracy ranged from 79.3% to 98%, with classification accuracy reaching up to 98.5%. The most common deep learning architectures used were GoogLeNet and DenseNet. While these results are promising, the review concludes that AI should be viewed as a powerful tool to assist and supplement clinical judgment, reducing workload and stress for physicians, rather than a complete replacement. Further research is still needed to validate its effectiveness in real-world clinical settings.
Intraoperative 3D imaging plays a crucial role in enhancing surgical accuracy and preventing the need for repeat operations [48]. The use of intraoperative 3D imaging systems like the Iso-C3D (Siemens Medical Solutions) during fracture surgery allows for the analysis of articular fractures and implant positions.
A prospective study on 109 fractures found that intraoperative 3D imaging led to a revision rate of 9.2% for error correction, which may prevent a second operation [49]. This technology is particularly useful for syndesmotic injuries, iliosacral screw fixation, and intraarticula fractures, with revision rates of 23.1%, 8.3%, and 6.6%, respectively, for these fracture sites. The revisions included changing malpositioned implants in six cases, correcting articular reduction in one, and revising syndesmosis malreduction in three. These errors were not visible with conventional 2D fluoroscopy. All surgical staff can exit the operating room during the 62-second 3D scan, which is comparable to the radiation exposure of a standard CT scan or conventional C-arm fluoroscopy, addressing concerns about radiation contamination.
3D intraoperative imaging and navigation are applied in various trauma cases, including acetabular fractures and limb fractures (wrist, rotational femoral malunion, distal tibiofibular syndesmosis, calcaneal fractures) [50-53]. The next frontier in surgical navigation involves integrating robotics, currently being validated for tasks like the reduction of long-bone fractures [54].
Researchers are developing deep learning models to predict bone mineral density and fracture risk from conventional X-ray images, such as chest X-rays [55,56]. This approach offers a significant advantage over specialized dual-energy X-ray absorptiometry scans, as X-rays are more common and less expensive. By using AI to analyze these readily available images, this method could enable opportunistic screening for osteoporosis, leading to earlier detection and intervention for individuals with bone density issues.
Another study focuses on the development and validation of a deep learning-based method for the automated measurement of psoas muscle volume in CT scans [57]. This new AI-driven system dramatically reduces measurement time while providing accurate and consistent results. The automated method is highlighted as a more efficient and reliable tool for diagnosing sarcopenia (age-related muscle loss) and is expected to help establish normal ranges for psoas muscle volume in large populations.
Challenges and future outlook
While AI offers numerous benefits to the orthopedic field, several challenges must be addressed for its widespread clinical adoption [5].
The initial equipment costs for robotic systems can exceed $800,000, with ongoing operational costs also being significant [58]. However, proponents argue that reduced revision rates due to improved accuracy and faster recovery can lead to long-term cost savings [58,59]. Studies suggest that while direct costs of robotic-assisted surgeries are higher, reductions in hospital stay duration and postoperative complications can lead to lower overall healthcare expenditures [60].
The learning curve associated with new technology requires careful consideration of its impact on training. Initial robotic surgeries may experience longer operative times, and serious complications such as patellar tendon rupture, fracture, or nerve injury have been reported during the early operations of a surgeon’s learning curve [9,61]. However, as proficiency increases, surgical efficiency is expected to improve, potentially leading to shorter operative times. Robotic surgery is well-suited for simulation training, which can translate to improved performance in the operating theatre [5].
Current AI research in orthopedics is growing but remains in its early stages, primarily consisting of small, retrospective studies. A lack of long-term, high-impact studies is cited as a limitation restricting the widespread implementation of robotic systems. The diversity of study designs and measurement techniques also makes direct comparisons between studies difficult. To enhance the credibility and generalizability of findings, future research should aim for larger sample sizes, cover a broader range of fracture types, and adopt prospective randomized controlled trial designs and multi-center studies.
Conclusions
AI and robotics have demonstrated immense potential in orthopedics including fracture and trauma treatment, by enhancing surgical precision, reinforcing patient safety, and improving diagnostic accuracy. Advances in preoperative planning and simulation, robotic-assisted surgery, and image-based diagnostic technologies have already yielded significant progress and clinical benefits.
However, widespread adoption faces challenges such as high initial costs, a lack of long-term clinical data, and data bias concerns. To overcome these issues, strong interdisciplinary collaboration and large-scale prospective studies are essential. Successfully integrating these technologies promises to revolutionize the treatment of musculoskeletal conditions and unlock new frontiers in patient care.
-
Author contribution
Conceptualization: CHK, JWK. Data curation: CHK, JWK. Formal analysis: CHK, JWK. Methodology: CHK, JWK. Investigation: CHK, JWK. Resources: CHK, JWK. Software: CHK, JWK. Supervision: JWK. Validation: CHK, JWK. Project administration: CHK, JWK. Visualization: CHK. Writing-original draft: CHK. Writing-review & editing: JWK. All authors read and approved the final manuscript.
-
Conflict of interests
Ji Wan Kim is a Deputy Editor of this journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
-
Funding
None.
-
Data availability
Not applicable.
-
Acknowledgments
None.
-
Supplementary materials
None.
-
Disclosure of generative AI use
During the preparation of this manuscript, Gemini Pro 2.5 and NotebookLM were used to summarize background literature, assist in language editing, and grammar checking. The authors reviewed and edited the content generated by the AI tool and take full responsibility for the final version of the manuscript. The AI tool was not listed as an author and was used solely as a supportive resource.
Article Information
Fig. 1.
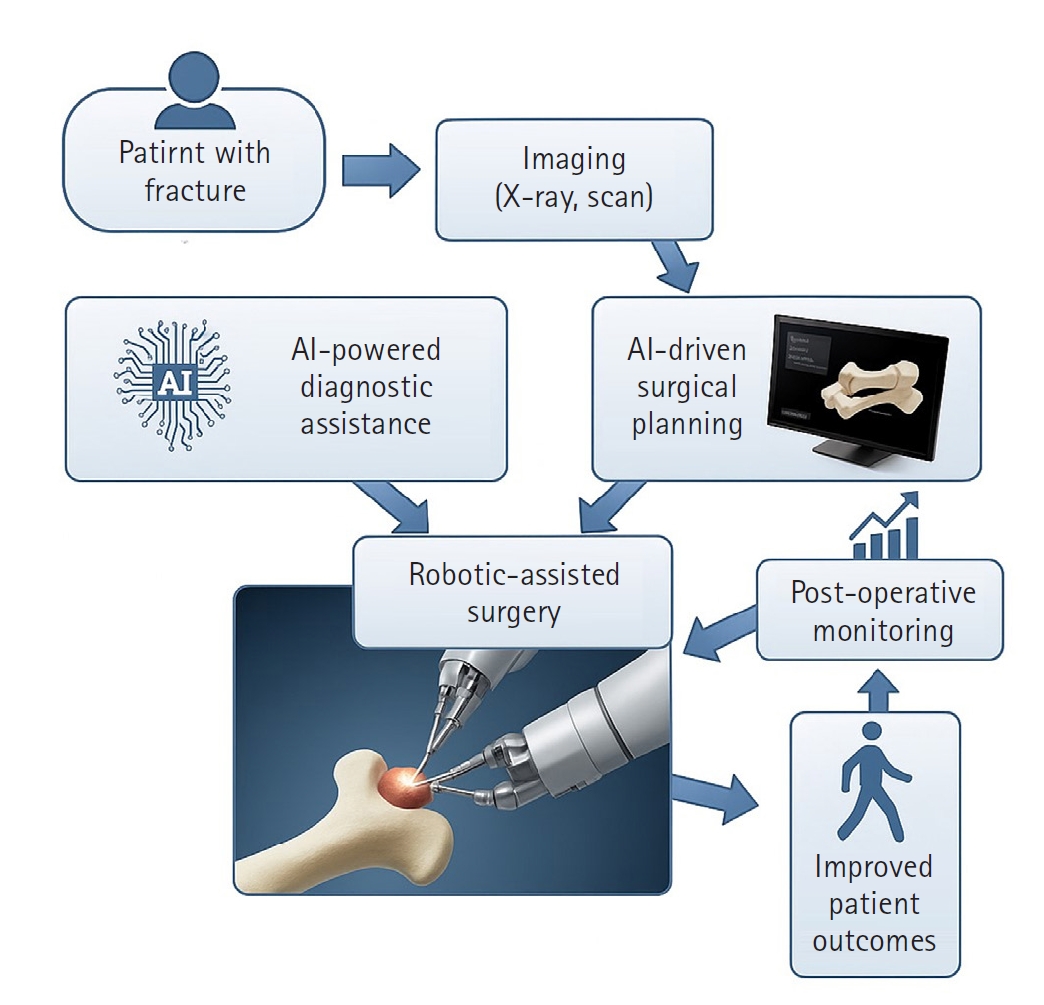
The integrated pathway of artificial intelligence (AI) and robotics in orthopedic trauma. This flowchart illustrates the modern workflow for treating fractures using artificial intelligence and robotics. The process starts with patient imaging, where AI algorithms assist in the diagnosis and classification of fractures. Next, AI-driven preoperative planning is conducted to determine the optimal surgical approach. During surgery, robotic systems execute the plan with high precision, which ultimately leads to improved patient outcomes, including faster recovery and improved safety.
Fig. 2.
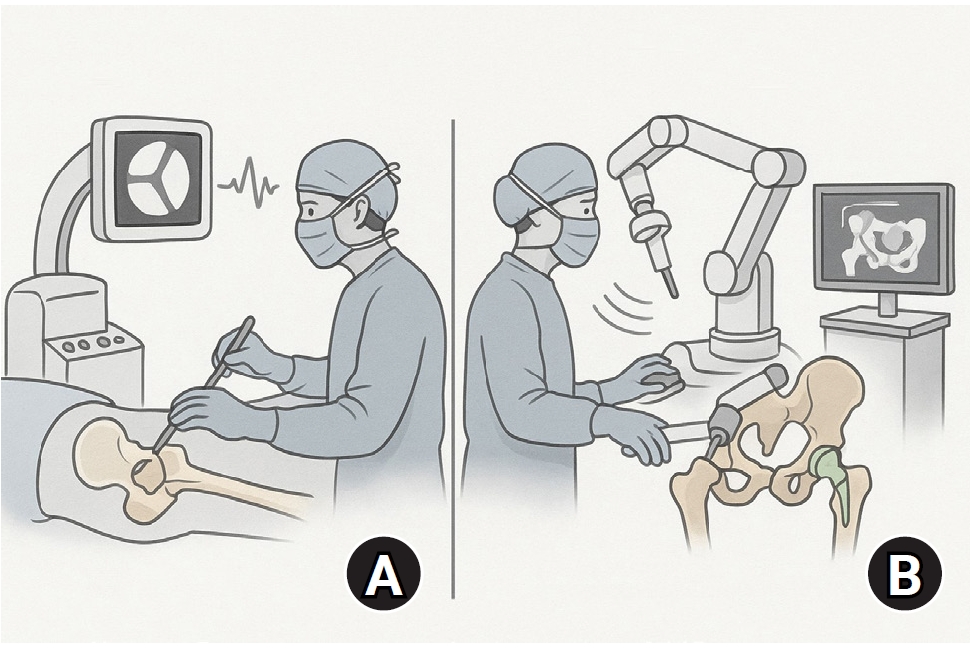
Precision of robotic-assisted surgery vs. conventional methods. A comparative view of surgical techniques. The conventional method (A) relies on the surgeon's experience and is guided by two-dimensional fluoroscopy, which can have variability. The robotic-assisted method (B) provides haptic feedback to guide the surgeon in executing the plan with high accuracy. This increases the precision of implant placement and fracture reduction while minimizing radiation exposure for the surgical staff.
- 1. Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg 2018;268:70-6.PubMed
- 2. Hui AT, Alvandi LM, Eleswarapu AS, Fornari ED. Artificial intelligence in modern orthopaedics: current and future applications. JBJS Rev 2022;10.
- 3. Ram PR, Jeyaraman M, Jeyaraman N, Yadav S, Venkatasalam R. Revolutionizing orthopedic healthcare: the role of robotics. Cureus 2023;15:e44820.ArticlePubMedPMC
- 4. Lang JE, Mannava S, Floyd AJ, et al. Robotic systems in orthopaedic surgery. J Bone Joint Surg Br 2011;93:1296-9.ArticlePubMedPDF
- 5. Karthik K, Colegate-Stone T, Dasgupta P, Tavakkolizadeh A, Sinha J. Robotic surgery in trauma and orthopaedics: a systematic review. Bone Joint J 2015;97-B:292-9.PubMed
- 6. Bargar WL, Bauer A, Börner M. Primary and revision total hip replacement using the Robodoc system. Clin Orthop Relat Res 1998;(354):82-91.ArticlePubMed
- 7. Lim SJ, Kim SM, Lim BH, Moon YW, Park YS. Comparison of manual rasping and robotic milling for short metaphyseal-fitting stem implantation in total hip arthroplasty: a cadaveric study. Comput Aided Surg 2013;18:33-40.ArticlePubMed
- 8. Sukovich W, Brink-Danan S, Hardenbrook M. Miniature robotic guidance for pedicle screw placement in posterior spinal fusion: early clinical experience with the SpineAssist. Int J Med Robot 2006;2:114-22.ArticlePubMed
- 9. Xiao X, Wang X, Meng B, Pan X, Zhao H. Comparison of robotic AI-assisted and manual pedicle screw fixation for treating thoracolumbar fractures: a retrospective controlled trial. Front Bioeng Biotechnol 2025;13:1491775.ArticlePubMedPMC
- 10. Jiang B, Pennington Z, Zhu A, et al. Three-dimensional assessment of robot-assisted pedicle screw placement accuracy and instrumentation reliability based on a preplanned trajectory. J Neurosurg Spine 2020;33:519-28.ArticlePubMed
- 11. Mason A, Paulsen R, Babuska JM, et al. The accuracy of pedicle screw placement using intraoperative image guidance systems. J Neurosurg Spine 2014;20:196-203.ArticlePubMed
- 12. Ma M, Wang Z, Ye J, Chen X. Effectiveness of TiRobot-assisted and free-hand percutaneous kyphoplasty via pedicle of vertebra in treatment of osteoporotic vertebral compression fracture of thoracic vertebra. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2023;37:1106-12.PubMedPMC
- 13. Wu Z, Dai Y, Zeng Y. Intelligent robot-assisted fracture reduction system for the treatment of unstable pelvic fractures. J Orthop Surg Res 2024;19:271.ArticlePubMedPMCPDF
- 14. Zhao C, Cao Q, Sun X, Wu X, Zhu G, Wang Y. Intelligent robot-assisted minimally invasive reduction system for reduction of unstable pelvic fractures. Injury 2023;54:604-14.ArticlePubMed
- 15. Zhao C, Wang Y, Wu X, Zhu G, Shi S. Design and evaluation of an intelligent reduction robot system for the minimally invasive reduction in pelvic fractures. J Orthop Surg Res 2022;17:205.ArticlePubMedPMCPDF
- 16. Garcia P, Rosen J, Kapoor C, et al. Trauma Pod: a semi-automated telerobotic surgical system. Int J Med Robot 2009;5:136-46.ArticlePubMed
- 17. Lei H, Sheng L, Manyi W, Junqiang W, Wenyong L. A biplanar robot navigation system for the distal locking of intramedullary nails. Int J Med Robot 2010;6:61-5.ArticlePubMedPDF
- 18. Oszwald M, Westphal R, Klepzig D, et al. Robotized access to the medullary cavity for intramedullary nailing of the femur. Technol Health Care 2010;18:173-80.ArticlePubMed
- 19. Garcia JC, Lebailly F, Mantovani G, Mendonca LA, Garcia J, Liverneaux P. Telerobotic manipulation of the brachial plexus. J Reconstr Microsurg 2012;28:491-4.ArticlePubMed
- 20. Mantovani G, Liverneaux P, Garcia JC, Berner SH, Bednar MS, Mohr CJ. Endoscopic exploration and repair of brachial plexus with telerobotic manipulation: a cadaver trial. J Neurosurg 2011;115:659-64.ArticlePubMed
- 21. Lan H, Tan Z, Li KN, Gao JH, Liu TH. Intramedullary nail fixation assisted by orthopaedic robot navigation for intertrochanteric fractures in elderly patients. Orthop Surg 2019;11:255-62.ArticlePubMedPMCPDF
- 22. Lu C, Wei X, Li L, et al. Robot-assisted PFNA surgery improves clinical outcomes in the treatment of unstable femoral intertrochanteric fractures in elderly patients compared with traditional PFNA surgery. Sci Rep 2025;15:3836.ArticlePubMedPMCPDF
- 23. Federer SJ, Jones GG. Artificial intelligence in orthopaedics: a scoping review. PLoS One 2021;16:e0260471.ArticlePubMedPMC
- 24. Eller-Vainicher C, Chiodini I, Santi I, et al. Recognition of morphometric vertebral fractures by artificial neural networks: analysis from GISMO Lombardia database. PLoS One 2011;6:e27277.ArticlePubMedPMC
- 25. Saygılı A, Albayrak S. An efficient and fast computer-aided method for fully automated diagnosis of meniscal tears from magnetic resonance images. Artif Intell Med 2019;97:118-30.ArticlePubMed
- 26. Carballido-Gamio J, Yu A, Wang L, et al. Hip fracture discrimination based on Statistical Multi-parametric Modeling (SMPM). Ann Biomed Eng 2019;47:2199-212.ArticlePubMedPMCPDF
- 27. Nguyen HH, Le DT, Shore-Lorenti C. AFFnet: a deep convolutional neural network for the detection of atypical femur fractures from anteriorposterior radiographs. Bone 2024;187:117215.ArticlePubMed
- 28. Russe MF, Rebmann P, Tran PH. AI-based X-ray fracture analysis of the distal radius: accuracy between representative classification, detection and segmentation deep learning models for clinical practice. BMJ Open 2024;14:e076954.ArticlePubMedPMC
- 29. Hemanth Kumar M, Karthika M, Saianiruth M, et al. A deep learning-based ensemble system for automated shoulder fracture detection in clinical radiographs [Preprint]. Posted 2025 Jul 17. arXiv 2507.13408. https://arxiv.org/abs/2507.13408.
- 30. Kazley JM, Banerjee S, Abousayed MM, Rosenbaum AJ. Classifications in brief: garden classification of femoral neck fractures. Clin Orthop Relat Res 2018;476:441-5.ArticlePubMedPMC
- 31. Zlowodzki M, Bhandari M, Keel M, Hanson BP, Schemitsch E. Perception of garden's classification for femoral neck fractures: an international survey of 298 orthopaedic trauma surgeons. Arch Orthop Trauma Surg 2005;125:503-5.ArticlePubMedPDF
- 32. Xing P, Zhang L, Wang T, Wang L, Xing W, Wang W. A deep learning algorithm that aids visualization of femoral neck fractures and improves physician training. Injury 2024;55:111997.ArticlePubMed
- 33. Cha Y, Kim JT, Park CH, Kim JW, Lee SY, Yoo JI. Artificial intelligence, machine learning on diagnosis, classification of hip fracture. systematic review. J Orthop Surg Res 2022;17:520.PubMedPMC
- 34. Sato Y, Takegami Y, Asamoto T, et al. Artificial intelligence improves the accuracy of residents in the diagnosis of hip fractures: a multicenter study. BMC Musculoskelet Disord 2021;22:407.PubMedPMC
- 35. Murphy EA, Ehrhardt B, Gregson CL, et al. Machine learning outperforms clinical experts in classification of hip fractures. Sci Rep 2022;12:2058.ArticlePubMedPMCPDF
- 36. Yoon SJ, Hyong Kim T, Joo SB, Eel Oh S. Automatic multi-class intertrochanteric femur fracture detection from CT images based on AO/OTA classification using faster R-CNN-BO method. J Appl Biomed 2020;18:97-105.ArticlePubMed
- 37. Adams M, Chen W, Holcdorf D, McCusker MW, Howe PD, Gaillard F. Computer vs human: deep learning versus perceptual training for the detection of neck of femur fractures. J Med Imaging Radiat Oncol 2019;63:27-32.ArticlePubMedPDF
- 38. Urakawa T, Tanaka Y, Goto S, Matsuzawa H, Watanabe K, Endo N. Detecting intertrochanteric hip fractures with orthopedist-level accuracy using a deep convolutional neural network. Skeletal Radiol 2019;48:239-44.ArticlePubMedPDF
- 39. Cheng CT, Ho TY, Lee TY, et al. Application of a deep learning algorithm for detection and visualization of hip fractures on plain pelvic radiographs. Eur Radiol 2019;29:5469-77.ArticlePubMedPMCPDF
- 40. Krogue JD, Cheng KV, Hwang KM, et al. Automatic hip fracture identification and functional subclassification with deep learning. Radiol Artif Intell 2020;2:e190023.ArticlePubMedPMC
- 41. Yu JS, Yu SM, Erdal BS, et al. Detection and localisation of hip fractures on anteroposterior radiographs with artificial intelligence: proof of concept. Clin Radiol 2020;75:237.e1-9.ArticlePubMed
- 42. Mutasa S, Varada S, Goel A, Wong TT, Rasiej MJ. Advanced deep learning techniques applied to automated femoral neck fracture detection and classification. J Digit Imaging 2020;33:1209-17.ArticlePubMedPMCPDF
- 43. Beyaz S, Açıcı K, Sümer E. Femoral neck fracture detection in X-ray images using deep learning and genetic algorithm approaches. Jt Dis Relat Surg 2020;31:175-83.ArticlePubMedPMC
- 44. Mawatari T, Hayashida Y, Katsuragawa S, et al. The effect of deep convolutional neural networks on radiologists' performance in the detection of hip fractures on digital pelvic radiographs. Eur J Radiol 2020;130:109188.ArticlePubMed
- 45. Yamada Y, Maki S, Kishida S, et al. Automated classification of hip fractures using deep convolutional neural networks with orthopedic surgeon-level accuracy: ensemble decision-making with antero-posterior and lateral radiographs. Acta Orthop 2020;91:699-704.ArticlePubMedPMC
- 46. Cheng CT, Chen CC, Cheng FJ, et al. A human-algorithm integration system for hip fracture detection on plain radiography: system development and validation study. JMIR Med Inform 2020;8:e19416.ArticlePubMedPMC
- 47. Bae J, Yu S, Oh J, et al. External validation of deep learning algorithm for detecting and visualizing femoral neck fracture including displaced and non-displaced fracture on plain X-ray. J Digit Imaging 2021;34:1099-109.ArticlePubMedPMCPDF
- 48. Yang YL, Zhou DS, He JL. Comparison of isocentric C-arm 3-dimensional navigation and conventional fluoroscopy for C1 lateral mass and C2 pedicle screw placement for atlantoaxial instability. J Spinal Disord Tech 2013;26:127-34.ArticlePubMed
- 49. Moon SW, Kim JW. Usefulness of intraoperative three-dimensional imaging in fracture surgery: a prospective study. J Orthop Sci 2014;19:125-31.ArticlePubMed
- 50. Hammerle D, Osterhoff G, Allemann F, Werner CM. Comparison of intraoperative 2D vs. 3D imaging in open reduction and fixation of distal radius fractures. Eur J Trauma Emerg Surg 2020;46:557-63.ArticlePubMedPDF
- 51. Khoury A, Whyne CM, Daly M, et al. Intraoperative cone-beam CT for correction of periaxial malrotation of the femoral shaft: a surface-matching approach. Med Phys 2007;34:1380-7.ArticlePubMedPDF
- 52. Franke J, von Recum J, Suda AJ, Grutzner PA, Wendl K. Intraoperative three-dimensional imaging in the treatment of acute unstable syndesmotic injuries. J Bone Joint Surg Am 2012;94:1386-90.ArticlePubMed
- 53. Franke J, Wendl K, Suda AJ, Giese T, Grützner PA, von Recum J. Intraoperative three-dimensional imaging in the treatment of calcaneal fractures. J Bone Joint Surg Am 2014;96:e72.ArticlePubMed
- 54. Dagnino G, Georgilas I, Morad S, et al. Image-guided surgical robotic system for percutaneous reduction of joint fractures. Ann Biomed Eng 2017;45:2648-62.ArticlePDF
- 55. Sato Y, Yamamoto N, Inagaki N, et al. Deep learning for bone mineral density and t-score prediction from chest X-rays: a multicenter study. Biomedicines 2022;10:2323.Article
- 56. Zhou L, Nguyen T, Choi S, Yoon J. U-net-based deep learning hybrid model: research and evaluation for precise prediction of spinal bone density on abdominal radiographs. Bioengineering (Basel) 2025;12:385.
- 57. Choi W, Kim CH, Yoo H, Yun HR, Kim DW, KiM JW. Development and validation of a reliable method for automated measurements of psoas muscle volume in CT scans using deep learning-based segmentation: a cross-sectional study. BMJ Open 2024;14:e079417.Article
- 58. Swank ML, Alkire M, Conditt M, Lonner JH. Technology and cost-effectiveness in knee arthroplasty: computer navigation and robotics. Am J Orthop (Belle Mead NJ) 2009;38(2 Suppl):32-6.
- 59. Pearle AD, O'Loughlin PF, Kendoff DO. Robot-assisted unicompartmental knee arthroplasty. J Arthroplasty 2010;25:230-7.Article
- 60. Elswick CM, Strong MJ, Joseph JR, Saadeh Y, Oppenlander M, Park P. Robotic-assisted spinal surgery: current generation instrumentation and new applications. Neurosurg Clin N Am 2020;31:103-10.
- 61. Gao S, Lv Z, Fang H. Robot-assisted and conventional freehand pedicle screw placement: a systematic review and meta-analysis of randomized controlled trials. Eur Spine J 2018;27:921-30.ArticlePDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- AI-Assisted Fracture Detection in Orthopedic and Trauma Imaging: Where It Works, Where It Fails, and Principles for Safe Clinical Deployment
Wojciech Michał Glinkowski, Paweł Kaminski, Rafał Obuchowicz
Diagnostics.2026; 16(10): 1420. CrossRef
 ePub Link
ePub Link Cite
CiteInnovative applications of artificial intelligence in orthopedics focusing on fracture and trauma treatment: a narrative review
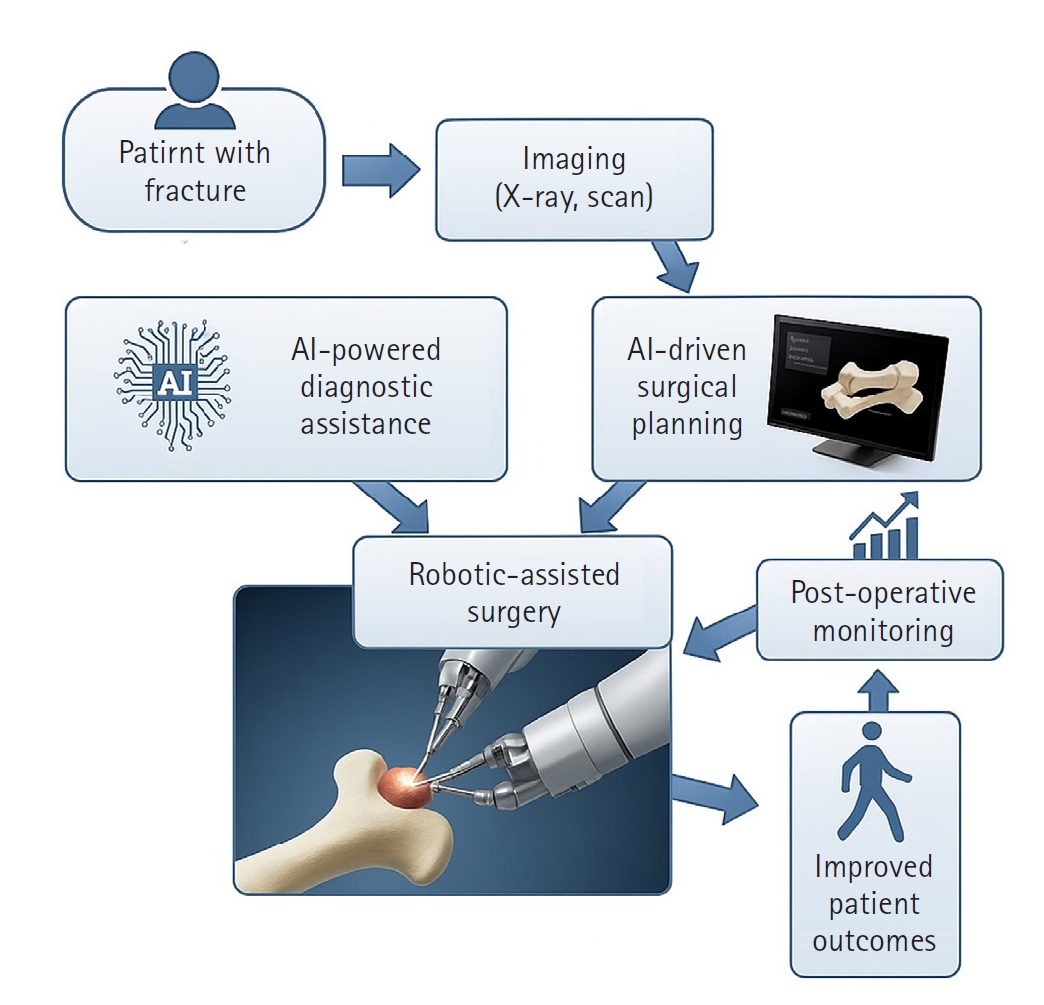
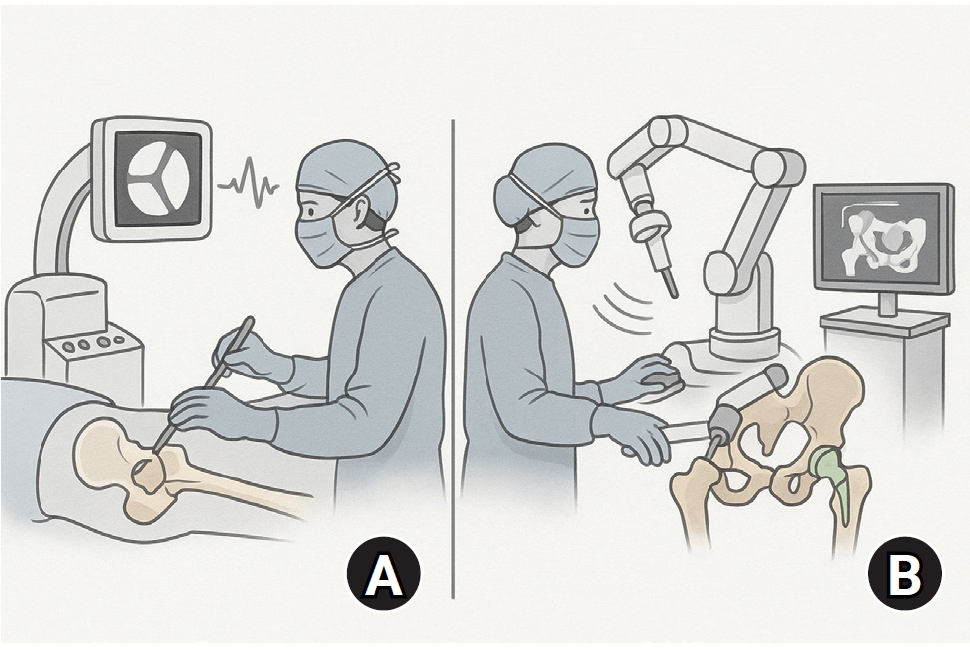
Fig. 1. The integrated pathway of artificial intelligence (AI) and robotics in orthopedic trauma. This flowchart illustrates the modern workflow for treating fractures using artificial intelligence and robotics. The process starts with patient imaging, where AI algorithms assist in the diagnosis and classification of fractures. Next, AI-driven preoperative planning is conducted to determine the optimal surgical approach. During surgery, robotic systems execute the plan with high precision, which ultimately leads to improved patient outcomes, including faster recovery and improved safety.
Fig. 2. Precision of robotic-assisted surgery vs. conventional methods. A comparative view of surgical techniques. The conventional method (A) relies on the surgeon's experience and is guided by two-dimensional fluoroscopy, which can have variability. The robotic-assisted method (B) provides haptic feedback to guide the surgeon in executing the plan with high accuracy. This increases the precision of implant placement and fracture reduction while minimizing radiation exposure for the surgical staff.
Fig. 1.
Fig. 2.
Innovative applications of artificial intelligence in orthopedics focusing on fracture and trauma treatment: a narrative review

