 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(4); 2011 > Article
-
Original Article
- The Impact on Clinical Results by Sagittal Imbalance in Posterior Fixation for Thoraco-lumbar Burst Fractures
- Seung-Wook Baek, M.D., Kyu-Dong Shim, M.D., Ye-Soo Park, M.D.
-
Journal of the Korean Fracture Society 2011;24(4):354-360.
DOI: https://doi.org/10.12671/jkfs.2011.24.4.354
Published online: October 30, 2011
Department of Orthopaedic Surgery, Guri Hospital, Hanyang University College of Medicine, Guri, Korea.
- Address reprint requests to: Ye-Soo Park, M.D. Department of Orthopaedic Surgery, Guri Hospital, Hanyang University College of Medicine, 249-1, Gyomun-dong, Guri 471-701, Korea. Tel: 82-31-560-2317, Fax: 82-31-557-8781, hyparkys@hanyang.ac.kr
• Received: February 18, 2011 • Revised: March 28, 2011 • Accepted: July 5, 2011
Copyright © 2011 The Korean Fracture Society
- 731 Views
- 1 Download
Abstract
-
Purpose
- Evaluate the effects of sagittal imbalance on the clinical outcomes in thoracolumbar burst fractures.
-
Materials and Methods
- We evaluated 11 patients who had received posterior fixation for unstable burst fractures. Radiologic assessment including the compression ratio, focal kyphotic angle and sagittal balance were obtained. The clinical outcomes were assessed by ODI, VAS and SF-36. We subdivided the patients into sagittal balance and imbalance group, and compared with clinical outcomes. The relationship between radiologic and clinical outcomes was examined using correlation analysis.
-
Results
- The radiologic assessment were changed on preoperative and postoperative as follows: mean compression ratio: 15.2%, 4.9%, mean focal kyphotic angle: 43.2°, 20.9°. The mean sagittal balance was 11.5 cm. The mean score of VAS, ODI, Physical and Mental Component Summary of SF-36 were 3.7, 45.8, 43.3 and 39.8, respectively. The ODI was significantly higher in sagittal imbalance group, and SF-36 was significantly higher in sagittal balance group (p<0.05). The VAS was correlated with compression ratio and focal kyphotic angle. The ODI and Mental Component Summary of SF-36 were correlated with sagittal imbalance.
-
Conclusion
- Sagittal balance effects on the functions of spine, surgical treatment should be carefully considered with unstable burst fractures.
- 1. Böhler J. Operative treatment of fractures of the dorsal and lumbar spine. J Trauma, 1970;10:1119-1122.Article
- 2. Bridwell KH, Lewis SJ, Rinella A, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbalance. Surgical technique. J Bone Joint Surg Am, 2004;86-A:1 Suppl. 44-50.
- 3. Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations. Spine (Phila Pa 1976), 1992;17:8 Suppl. S317-S324.Article
- 4. Cobb JR. Outline for the study of scoliosis. Instructional Course Lectures, The American Academy of Orthopaedic Surgeons. Ann Arbor JW Edwards, 1948;5:261-275.
- 5. Chang KW. Oligosegmental correction of post-traumatic thoracolumbar angular kyphosis. Spine (Phila Pa 1976), 1993;18:1909-1915.Article
- 6. Denis F, Armstrong GW, Searls K, Matta L. Acute thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between operative and nonoperative treatment. Clin Orthop Relat Res, 1984;(189):142-149.Article
- 7. During J, Goudfrooij H, Keessen W, Beeker TW, Crowe A. Toward standards for posture. Postural characteristics of the lower back system in normal and pathologic conditions. Spine (Phila Pa 1976), 1985;10:83-87.
- 8. Farcy JP, Schwab FJ. Management of flatback and related kyphotic decompensation syndromes. Spine (Phila Pa 1976), 1997;22:2452-2457.Article
- 9. Guilfoyle MR, Seeley H, Laing RJ. The Short Form 36 health survey in spine disease--validation against condition-specific measures. Br J Neurosurg, 2009;23:401-405.Article
- 10. Heary RF, Bono CM. Pedicle subtraction osteotomy in the treatment of chronic, posttraumatic kyphotic deformity. J Neurosurg Spine, 2006;5:1-8.Article
- 11. Jeon CH, Kim DJ, Kim DJ, Lee HM, Park HJ. Cross-cultural adaptation of the Korean version Of the oswestry disability index (ODI). J Korean Soc Spine Surg, 2005;12:146-152.Article
- 12. Kang CN, Kim JO, Kang OY, Ahn SO. The comparision of conservative treatment with operative treatment in bursting fracture. J Korean Soc Fract, 1995;8:807-814.Article
- 13. Kim CH, Hwang JK, Choi YJ, Kim KH, Song JS, Kang JH. Treatment of thoraco-lumbar bursting fractures according to load-sharing classification. J Korean Fract Soc, 2005;18:69-75.Article
- 14. Kim KT, Lee JH. Sagittal imbalance. J Korean Soc Spine Surg, 2009;16:142-151.Article
- 15. Kruz LT, Herkowitz HN, Samberg LC. Management of major thoracic and thoracolumbar spine injuries. State of the Art Reviews, 1989;302:243-267.
- 16. Kuner EH, Kuner A, Schlickewei W, Mullaji AB. Ligamentotaxis with an internal spinal fixator for thoracolumbar fractures. J Bone Joint Surg Br, 1994;76:107-112.ArticlePDF
- 17. Lehmer SM, Keppler L, Biscup RS, Enker P, Miller SD, Steffee AD. Posterior transvertebral osteotomy for adult thoracolumbar kyphosis. Spine (Phila Pa 1976), 1994;19:2060-2067.Article
- 18. Lee CS, Chung SS, Chung KH, Kim SR. Significance of pelvic incidence in the development of abnormal sagittal alignment. J Korean Orthop Assoc, 2006;41:274-280.ArticlePDF
- 19. Lee CS, Kim YT, Kim E. Clinical study of lumbar degenerative kyphosis. J Korean Soc Spine Surg, 1997;4:27-35.
- 20. Lee CS, Lee CK, Kim YT, Hong YM, Yoo JH. Dynamic sagittal imbalance of the spine in degenerative flat back: significance of pelvic tilt in surgical treatment. Spine (Phila Pa 1976), 2001;26:2029-2035.
- 21. Lenke LG, Bridwell KH, Baldus C, Blanke K, Schoenecker PL. Cotrel-Dubousset instrumentation for adolescent idiopathic scoliosis. J Bone Joint Surg Am, 1992;74:1056-1067.Article
- 22. Mahar A, Kim C, Wedemeyer M, Mitsunaga L, Odell T, Johnson B, Garfin S. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture. Spine (Phila Pa 1976), 2007;32:1503-1507.Article
- 23. McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine (Phila Pa 1976), 1994;19:1741-1744.Article
- 24. McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am, 1993;75:162-167.Article
- 25. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976), 1993;18:955-970.
- 26. Steib JP, Charles YP, Aoui M. In situ contouring technique in the treatment of thoracolumbar fractures. Eur Spine J, 2010;19:Suppl 1. S66-S68.ArticlePDF
- 27. Vialle R, Levassor N, Rillardon L, Templier A, Skalli W, Guigui P. Radiographic analysis of the sagittal alignment and balance of the spine in asymptomatic subjects. J Bone Joint Surg Am, 2005;87:260-267.Article
- 28. Yoon HK, Jeon HS, Cho KN, Kang SI. Prognostic factors to final results after conservative or surgical treatment of thoracolumbar burst fractures. J Korean Soc Spine Surg, 1998;5:215-223.
- 29. Young MH. Long-term consequences of stable fractures of the thoracic and lumbar vertebral bodies. J Bone Joint Surg Br, 1973;55:295-300.ArticlePDF
- 30. Yue JJ, Sossan A, Selgrath C, Deutsch LS, Wilkens K, Testaiuti M, Gabriel JP. The treatment of unstable thoracic spine fractures with transpedicular screw instrumentation: a 3-year consecutive series. Spine (Phila Pa 1976), 2002;27:2782-2787.Article
REFERENCES
Fig. 1
A 80-year-old female with L1 burst fracture.
(A) Preoperative lateral plain radiographs shows a loss of anterior height of L1.
(B) Lateral radiograph after operation shows correction of the compression ratio and focal kyphotic angle.
(C) Standing lateral whole spine radiographs obtained 1 years after operation shows loss of reduction in sagittal imbalance.

Fig. 2
A 42-year-old male with L1 burst fracture.
(A) Preoperative lateral plain radiographs shows a loss of anterior height of L1.
(B) Lateral radiograph after operation shows correction of the compression ratio and focal kyphotic angle.
(C) Standing lateral whole spine radiographs obtained 1 years after operation shows no reduction loss in normal sagittal alignment.

Table 1Main clinical and radiographic characteristics of 11 patients with thoracolumbar burst fracture



Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteThe Impact on Clinical Results by Sagittal Imbalance in Posterior Fixation for Thoraco-lumbar Burst Fractures
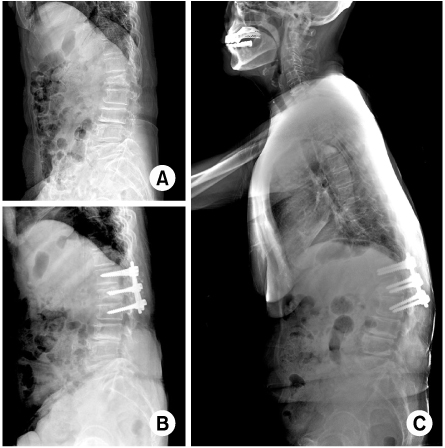
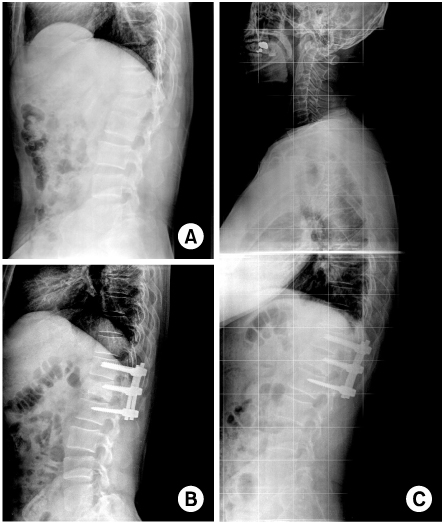
Fig. 1
A 80-year-old female with L1 burst fracture.
(A) Preoperative lateral plain radiographs shows a loss of anterior height of L1.
(B) Lateral radiograph after operation shows correction of the compression ratio and focal kyphotic angle.
(C) Standing lateral whole spine radiographs obtained 1 years after operation shows loss of reduction in sagittal imbalance.
Fig. 2
A 42-year-old male with L1 burst fracture.
(A) Preoperative lateral plain radiographs shows a loss of anterior height of L1.
(B) Lateral radiograph after operation shows correction of the compression ratio and focal kyphotic angle.
(C) Standing lateral whole spine radiographs obtained 1 years after operation shows no reduction loss in normal sagittal alignment.
Fig. 1
Fig. 2
The Impact on Clinical Results by Sagittal Imbalance in Posterior Fixation for Thoraco-lumbar Burst Fractures
Main clinical and radiographic characteristics of 11 patients with thoracolumbar burst fracture
Mos.: Months, Pre-op.: Preoperative, Post-op.: Postoperative, TKA: Thoracic kyphotic angle, LLA: Lumbar lordotic angle, ODI: Oswestry disability index.
Score of VAS, ODI and SF-36
PCS: Physical component summary, MCS: Mental component summary. *Independent t-test.
Correlations between radiological and clinical outcomes
The table shows correlations between each radiological and clinical outcome. Correlations between variables were using Spearman's rank correlations (rs). PCS: Physical component summary, MCS: Mental component summary. *p<0.05, †p<0.01.
Table 1
Main clinical and radiographic characteristics of 11 patients with thoracolumbar burst fracture
Mos.: Months, Pre-op.: Preoperative, Post-op.: Postoperative, TKA: Thoracic kyphotic angle, LLA: Lumbar lordotic angle, ODI: Oswestry disability index.
Table 2
Score of VAS, ODI and SF-36
PCS: Physical component summary, MCS: Mental component summary. *Independent t-test.
Table 3
Correlations between radiological and clinical outcomes
The table shows correlations between each radiological and clinical outcome. Correlations between variables were using Spearman's rank correlations (rs). PCS: Physical component summary, MCS: Mental component summary. *p<0.05, †p<0.01.

