 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 34(1); 2021 > Article
- Original Article Comparing Outcomes of Screw Fixation and Non-Fixation for Small-Sized Posterior Malleolar Fragment in Ankle Trimalleolar Fractures
- Jee-Wook Ko, Gun-Woo Lee, Keun-Bae Lee
-
Journal of Musculoskeletal Trauma 2021;34(1):8-15.
DOI: https://doi.org/10.12671/jkfs.2021.34.1.8
Published online: January 31, 2021
Department of Orthopedic Surgery, Chonnam National University Medical School and Hospital, Gwangju, Korea
- 1,210 Views
- 13 Download
- 0 Crossref
- 0 Scopus
Abstract
Purpose
This study was undertaken to compare outcomes of screw fixation and non-fixation of a small-sized posterior malleolar fragment involving less than 25% articular surface in ankle trimalleolar fractures.
Materials and Methods: A total of 32 consecutive ankles (32 patients), with posterior malleolar fragment involving 15%-25% of the joint surface, were enrolled in the study. Patients were divided into 2 groups according to whether the fragment was fixed or not (fixed: 20 ankles, non-fixed: 12 ankles).
The minimum follow-up period was 12 months. Median size of the posterior malleolar fragment in the fixed and non-fixed groups were 24.6% (range, 22.3%-25.0%) and 22.1% (range, 17.4%-24.3%), respectively. Complications as well as clinical and radiographic outcomes were compared and analyzed between the two groups.
Results: Clinical outcomes, including American Orthopaedic Foot & Ankle Society (p=0.501), visual analogue scale (p=0.578), and ankle range of motion (p=0.552), showed no difference between groups at the final follow-up. No differences were obtained in the radiographic outcomes, including joint stepoff (p=0.289) and fragment gap (p=0.289). Complications, including 1 case of delayed union and 1 case of wound infection, were reported in the fixed group.
Conclusion: Clinical outcomes and radiographic outcomes of the non-fixation group were satisfactory and comparable to the fixation group. Our results indicate that anatomical reduction with small-sized posterior malleolar fragment in ankle trimalleolar fractures is sufficient for satisfactory outcomes, without the need for additional internal fixation.
J Korean Fract Soc. 2021 Jan;34(1):8-15. Korean.
Published online Jan 25, 2021.
https://doi.org/10.12671/jkfs.2021.34.1.8
Published online Jan 25, 2021.
https://doi.org/10.12671/jkfs.2021.34.1.8
Copyright © 2021 The Korean Fracture Society. All rights reserved.
Original Article
Comparing Outcomes of Screw Fixation and Non-Fixation for Small-Sized Posterior Malleolar Fragment in Ankle Trimalleolar Fractures

Abstract
Purpose
This study was undertaken to compare outcomes of screw fixation and non-fixation of a small-sized posterior malleolar fragment involving less than 25% articular surface in ankle trimalleolar fractures.
Materials and Methods
A total of 32 consecutive ankles (32 patients), with posterior malleolar fragment involving 15%–25% of the joint surface, were enrolled in the study. Patients were divided into 2 groups according to whether the fragment was fixed or not (fixed: 20 ankles, non-fixed: 12 ankles). The minimum follow-up period was 12 months. Median size of the posterior malleolar fragment in the fixed and non-fixed groups were 24.6% (range, 22.3%–25.0%) and 22.1% (range, 17.4%–24.3%), respectively. Complications as well as clinical and radiographic outcomes were compared and analyzed between the two groups.
Results
Clinical outcomes, including American Orthopaedic Foot & Ankle Society (p=0.501), visual analogue scale (p=0.578), and ankle range of motion (p=0.552), showed no difference between groups at the final follow-up. No differences were obtained in the radiographic outcomes, including joint stepoff (p=0.289) and fragment gap (p=0.289). Complications, including 1 case of delayed union and 1 case of wound infection, were reported in the fixed group.
Conclusion
Clinical outcomes and radiographic outcomes of the non-fixation group were satisfactory and comparable to the fixation group. Our results indicate that anatomical reduction with small-sized posterior malleolar fragment in ankle trimalleolar fractures is sufficient for satisfactory outcomes, without the need for additional internal fixation.
Keywords
Ankle, Posterior malleolus fracture, Small-sized fragment, Screw fixation, Non-fixation
Figures
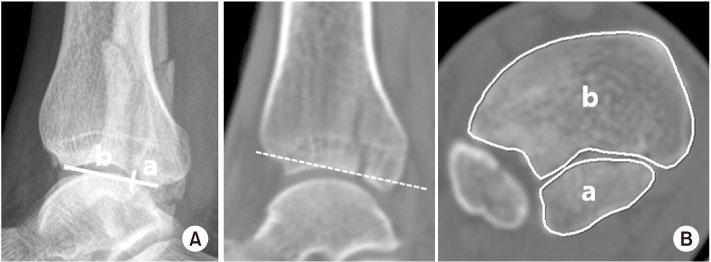
Fig. 1
(A) Method of measuring proportion of the posterior malleolar fragment by calculating length of the fragment on lateral plain radiograph; a/(a+b). (B) In the current study, ratio of the posterior malleolar fragment to the joint surface was measured on the axial image of computed tomography at the level corresponding to the distal tibia joint surface, using automatic area calculating tool of the PACS system; a/(a+b).

Fig. 2
(A) A 56-year-old female sustained a rotational ankle fracture with a posterior malleolar fracture. (B) Articular involvement of posterior malleolar fragment to the joint surface area of the distal tibia was 19.0% on axial computed tomography (CT) imaging. Preoperative step-off and fragment gap were 2.0 mm and 2.5 mm, respectively, on the sagittal CT imaging. (C) The posterior malleolar fragment was fixed using a posterior to anterior lag screw. (D) At 27 months postoperatively, the fracture site was well united without step-off, and showed a mild joint irregularity at the fracture site.

Fig. 3
(A) A 68-year-old male sustained a rotational ankle fracture with a posterior malleolar fracture. (B) Articular involvement of posterior malleolar fragment to the joint surface area of the distal tibia was 23.6% on the axial computed tomography (CT) imaging. Preoperative step-off and fragment gap were 2.0 mm and 1.5 mm, respectively, on the sagittal CT imaging. (C) After reduction of the lateral malleolus, the posterior malleolar fragment was not fixed. (D) At 24 months postoperatively, the fracture site union was achieved, with no articular step-off and joint irregularity.
Tables
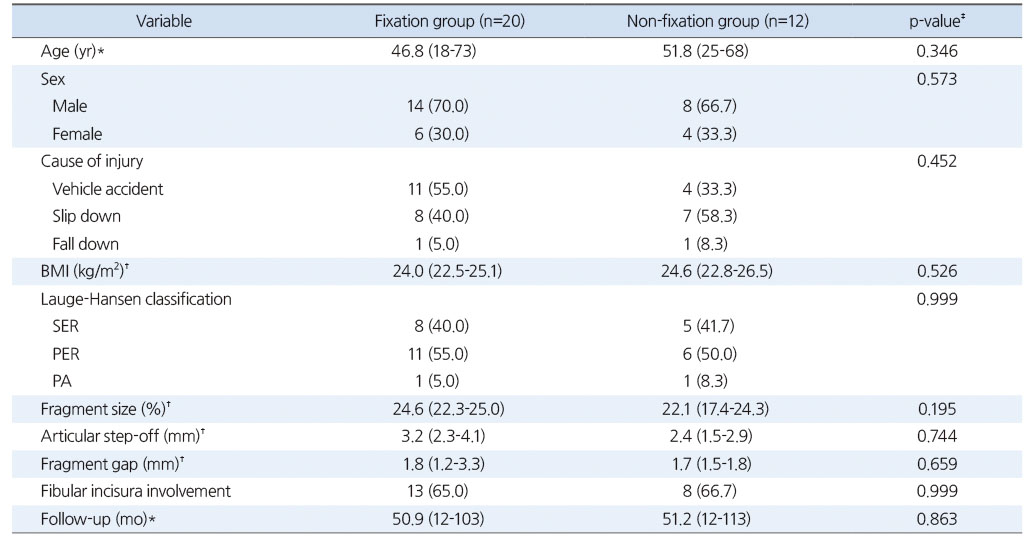
Table 1
Demographic Data and Preoperative Radiographic Results of Fixation and Non-Fixation Groups for Posterior Malleolar Fragment in Ankle
Trimalleolar Fractures
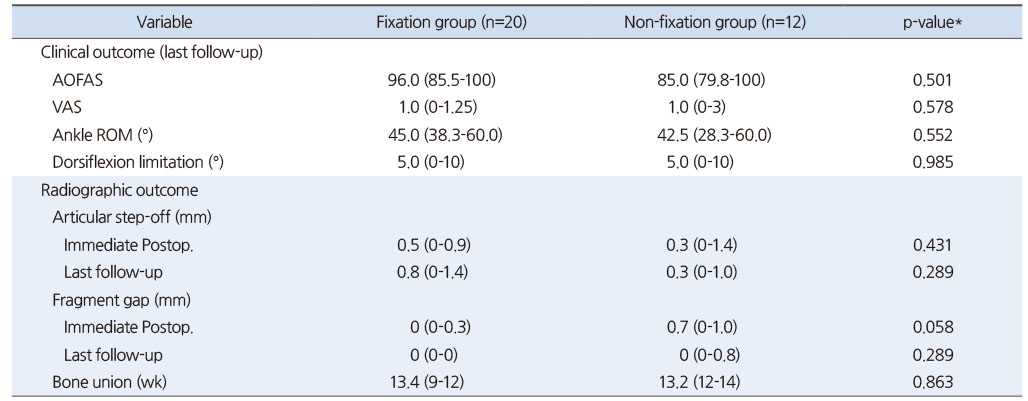
Table 2
Comparison of Clinical and Radiographic Outcomes of Fixation and Non-Fixation Groups for Posterior Malleolar Fragment in Ankle Trimalleolar Fractures
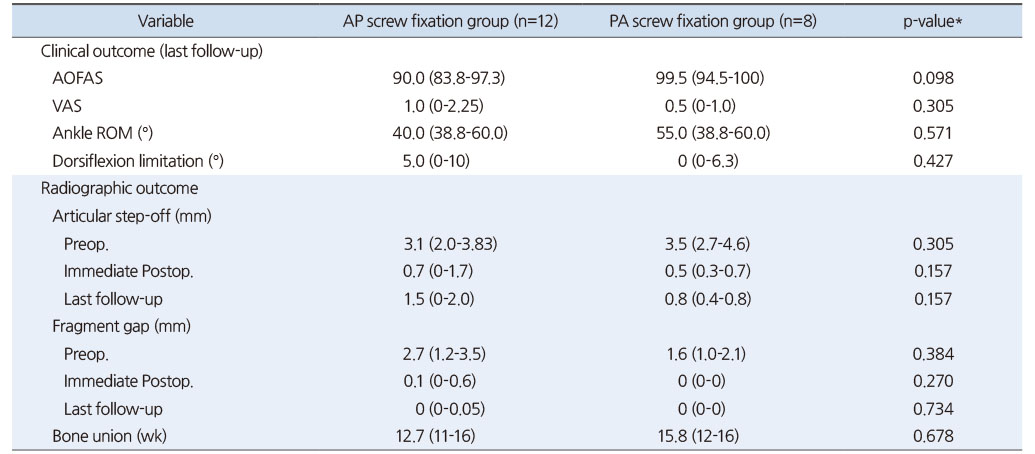
Table 3
Comparison of Clinical and Radiographic Outcomes of AP Screw and PA Screw Fixation Groups for Posterior Malleolar Fragment in Ankle Trimalleolar Fractures
Notes
Financial support:None.
Conflict of interests:None.
References
-
Daly PJ, Fitzgerald RH Jr, Melton LJ, Ilstrup DM. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand 1987;58:539–544.
-
-
Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures--an increasing problem. Acta Orthop Scand 1998;69:43–47.
-
-
Jaskulka RA, Ittner G, Schedl R. Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma 1989;29:1565–1570.
-
-
Harper MC, Hardin G. Posterior malleolar fractures of the ankle associated with external rotation-abduction injuries. Results with and without internal fixation. J Bone Joint Surg Am 1988;70:1348–1356.
-
-
Talbot M, Steenblock TR, Cole PA. Posterolateral approach for open reduction and internal fixation of trimalleolar ankle fractures. Can J Surg 2005;48:487–490.
-
-
Bartoníček J, Rammelt S, Kostlivý K, Vaněček V, Klika D, Trešl I. Anatomy and classification of the posterior tibial fragment in ankle fractures. Arch Orthop Trauma Surg 2015;135:505–516.
-
-
Gardner MJ, Brodsky A, Briggs SM, Nielson JH, Lorich DG. Fixation of posterior malleolar fractures provides greater syndesmotic stability. Clin Orthop Relat Res 2006;447:165–171.
-
-
Odak S, Ahluwalia R, Unnikrishnan P, Hennessy M, Platt S. Management of posterior malleolar fractures: a systematic review. J Foot Ankle Surg 2016;55:140–145.
-
-
Macko VW, Matthews LS, Zwirkoski P, Goldstein SA. The joint-contact area of the ankle. The contribution of the posterior malleolus. J Bone Joint Surg Am 1991;73:347–351.
-
-
De Vries JS, Wijgman AJ, Sierevelt IN, Schaap GR. Long-term results of ankle fractures with a posterior malleolar fragment. J Foot Ankle Surg 2005;44:211–217.
-
-
Wei SY, Okereke E, Winiarsky R, Lotke PA. Nonoperatively treated displaced bimalleolar and trimalleolar fractures: a 20-year follow-up. Foot Ankle Int 1999;20:404–407.
-
-
Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am 2006;88:1085–1092.
-
-
Bartoníček J, Rammelt S, Tuček M. Posterior malleolar fractures: changing concepts and recent developments. Foot Ankle Clin 2017;22:125–145.
-
-
Rammelt S, Boszczyk A. Computed tomography in the diagnosis and treatment of ankle fractures: a critical analysis review. JBJS Rev 2018;6:e7.
-
-
Weber M. Trimalleolar fractures with impaction of the posteromedial tibial plafond: implications for talar stability. Foot Ankle Int 2004;25:716–727.
-
-
Mason LW, Marlow WJ, Widnall J, Molloy AP. Pathoanatomy and associated injuries of posterior malleolus fracture of the ankle. Foot Ankle Int 2017;38:1229–1235.
-
-
Miller AN, Carroll EA, Parker RJ, Helfet DL, Lorich DG. Posterior malleolar stabilization of syndesmotic injuries is equivalent to screw fixation. Clin Orthop Relat Res 2010;468:1129–1135.
-
-
Fitzpatrick DC, Otto JK, McKinley TO, Marsh JL, Brown TD. Kinematic and contact stress analysis of posterior malleolus fractures of the ankle. J Orthop Trauma 2004;18:271–278.
-
-
Hartford JM, Gorczyca JT, McNamara JL, Mayor MB. Tibiotalar contact area. Contribution of posterior malleolus and deltoid ligament. Clin Orthop Relat Res 1995;(320):182–187.
-
-
Langenhuijsen JF, Heetveld MJ, Ultee JM, Steller EP, Butzelaar RM. Results of ankle fractures with involvement of the posterior tibial margin. J Trauma 2002;53:55–60.
-
-
Mingo-Robinet J, López-Durán L, Galeote JE, Martinez-Cervell C. Ankle fractures with posterior malleolar fragment: management and results. J Foot Ankle Surg 2011;50:141–145.
-
-
Solan MC, Sakellariou A. Posterior malleolus fractures: worth fixing. Bone Joint J 99. B 2017:1413–1419.
-
-
Evers J, Fischer M, Zderic I, et al. The role of a small posterior malleolar fragment in trimalleolar fractures: a biomechanical study. Bone Joint J 2018;100-B:95–100.
-
-
Kitaoka HB, Alexander IJ, Adelaar RS, et al. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 1997;18:187–188.
-
-
O'Connor TJ, Mueller B, Ly TV, Jacobson AR, Nelson ER, Cole PA. “A to p” screw versus posterolateral plate for posterior malleolus fixation in trimalleolar ankle fractures. J Orthop Trauma 2015;29:e151–e156.
-
-
Raasch WG, Larkin JJ, Draganich LF. Assessment of the posterior malleolus as a restraint to posterior subluxation of the ankle. J Bone Joint Surg Am 1992;74:1201–1206.
-
-
Drijfhout van Hooff CC, Verhage SM, Hoogendoorn JM. Influence of fragment size and postoperative joint congruency on long-term outcome of posterior malleolar fractures. Foot Ankle Int 2015;36:673–678.
-
-
Meijer DT, Doornberg JN, Sierevelt IN, et al. Guesstimation of posterior malleolar fractures on lateral plain radiographs. Injury 2015;46:2024–2029.
-
-
Büchler L, Tannast M, Bonel HM, Weber M. Reliability of radiologic assessment of the fracture anatomy at the posterior tibial plafond in malleolar fractures. J Orthop Trauma 2009;23:208–212.
-
-
Ferries JS, DeCoster TA, Firoozbakhsh KK, Garcia JF, Miller RA. Plain radiographic interpretation in trimalleolar ankle fractures poorly assesses posterior fragment size. J Orthop Trauma 1994;8:328–331.
-
-
Burns WC 2nd, Prakash K, Adelaar R, Beaudoin A, Krause W. Tibiotalar joint dynamics: indications for the syndesmotic screw--a cadaver study. Foot Ankle 1993;14:153–158.
-
-
Scheidt KB, Stiehl JB, Skrade DA, Barnhardt T. Posterior malleolar ankle fractures: an in vitro biomechanical analysis of stability in the loaded and unloaded states. J Orthop Trauma 1992;6:96–101.
-
-
Miller MA, McDonald TC, Graves ML, et al. Stability of the syndesmosis after posterior malleolar fracture fixation. Foot Ankle Int 2018;39:99–104.
-
-
Baumbach SF, Herterich V, Damblemont A, Hieber F, Böcker W, Polzer H. Open reduction and internal fixation of the posterior malleolus fragment frequently restores syndesmotic stability. Injury 2019;50:564–570.
-
-
Erdem MN, Erken HY, Burc H, Saka G, Korkmaz MF, Aydogan M. Comparison of lag screw versus buttress plate fixation of posterior malleolar fractures. Foot Ankle Int 2014;35:1022–1030.
-
-
Kang C, Hwang DS, Lee JK, Won Y, Song JH, Lee GS. Screw fixation of the posterior malleolus fragment in ankle fracture. Foot Ankle Int 2019;40:1288–1294.
-
-
Xu HL, Li X, Zhang DY, et al. A retrospective study of posterior malleolus fractures. Int Orthop 2012;36:1929–1936.
-
-
Berkes MB, Little MT, Lazaro LE, et al. Articular congruity is associated with short-term clinical outcomes of operatively treated SER IV ankle fractures. J Bone Joint Surg Am 2013;95:1769–1775.
-
-
Verhage SM, Krijnen P, Schipper IB, Hoogendoorn JM. Persistent postoperative step-off of the posterior malleolus leads to higher incidence of post-traumatic osteoarthritis in trimalleolar fractures. Arch Orthop Trauma Surg 2019;139:323–329.
-
 Cite
Cite
