 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 34(1); 2021 > Article
- Original Article Clinical Outcomes of Customized Staple Fixation Using K-wire in Metacarpal Base or Neck Fractures
- Hong-ki Jin, Hyoung Min Kim, Yong Seung Oh, Jihoon Kim
-
Journal of Musculoskeletal Trauma 2021;34(1):23-29.
DOI: https://doi.org/10.12671/jkfs.2021.34.1.23
Published online: January 31, 2021
Department of Orthopedic Surgery, Good Samsun Hospital, Busan, Korea
- 1,472 Views
- 5 Download
- 1 Crossref
- 0 Scopus
Abstract
Purpose
This study was designed to evaluate the radiological and clinical outcomes of a new surgical technique—customized staple fixation using K-wire—in displaced metacarpal neck or base fractures.
Materials and Methods: From November 2016 to May 2017, 13 unstable metacarpal neck and base fractures (10 patients) were treated with II-shaped customized K-wire staples fixation, after performing open reductions through minimal dorsal incisions. The radiological and clinical outcomes were retrospectively evaluated.
Results: A mean of 2.6 staples were used for each fracture fixation. Preoperative angulation of 36.3°was reduced to 3.1° postoperatively. A week after surgery, the volar short arm splint was replaced with a dorsal splint to initiate active range of motion exercise, and the splint was subsequently removed after 3 weeks. The radiologic union was achieved at a mean of 5.1 weeks, and total active motion was recovered at a mean of 7.4 weeks. On a mean, K-wire staples were removed at 16.5 weeks after the surgery, and the mean treatment took 18.6 weeks. At the final follow-up (at mean 27.3 weeks), no significant difference was observed for total active motion of the digits and grip strength, when compared to the contralateral hand. Complete union was achieved in all fractures without deformity, or complications such as infection or nerve injury. All patients were satisfied with the cosmetic and functional outcomes.
Conclusion: K-wire stapling is an effective alternative modality in treating unstable displaced metacarpal neck or base fractures. It requires minimal incision to enable open reduction. In addition, early mobilization is ensured through the rigid fixations. Moreover, it prevents postoperative joint stiffness and reduces the time needed for treatment.
J Korean Fract Soc. 2021 Jan;34(1):23-29. Korean.
Published online Jan 25, 2021.
https://doi.org/10.12671/jkfs.2021.34.1.23
Published online Jan 25, 2021.
https://doi.org/10.12671/jkfs.2021.34.1.23
Copyright © 2021 The Korean Fracture Society. All rights reserved.
Original Article
Clinical Outcomes of Customized Staple Fixation Using K-wire in Metacarpal Base or Neck Fractures

Abstract
Purpose
This study was designed to evaluate the radiological and clinical outcomes of a new surgical technique—customized staple fixation using K-wire—in displaced metacarpal neck or base fractures.
Materials and Methods
From November 2016 to May 2017, 13 unstable metacarpal neck and base fractures (10 patients) were treated with II-shaped customized K-wire staples fixation, after performing open reductions through minimal dorsal incisions. The radiological and clinical outcomes were retrospectively evaluated.
Results
A mean of 2.6 staples were used for each fracture fixation. Preoperative angulation of 36.3° was reduced to 3.1° postoperatively. A week after surgery, the volar short arm splint was replaced with a dorsal splint to initiate active range of motion exercise, and the splint was subsequently removed after 3 weeks. The radiologic union was achieved at a mean of 5.1 weeks, and total active motion was recovered at a mean of 7.4 weeks. On a mean, K-wire staples were removed at 16.5 weeks after the surgery, and the mean treatment took 18.6 weeks. At the final follow-up (at mean 27.3 weeks), no significant difference was observed for total active motion of the digits and grip strength, when compared to the contralateral hand. Complete union was achieved in all fractures without deformity, or complications such as infection or nerve injury. All patients were satisfied with the cosmetic and functional outcomes.
Conclusion
K-wire stapling is an effective alternative modality in treating unstable displaced metacarpal neck or base fractures. It requires minimal incision to enable open reduction. In addition, early mobilization is ensured through the rigid fixations. Moreover, it prevents postoperative joint stiffness and reduces the time needed for treatment.
Keywords
Metacarpal fracture, Neck, Base, Staple, Open reduction
Figures

Fig. 1
A 2-cm longitudinal incision was made at the fracture site. After open reduction, the fracture site was temporarily fixed using the K-wire.
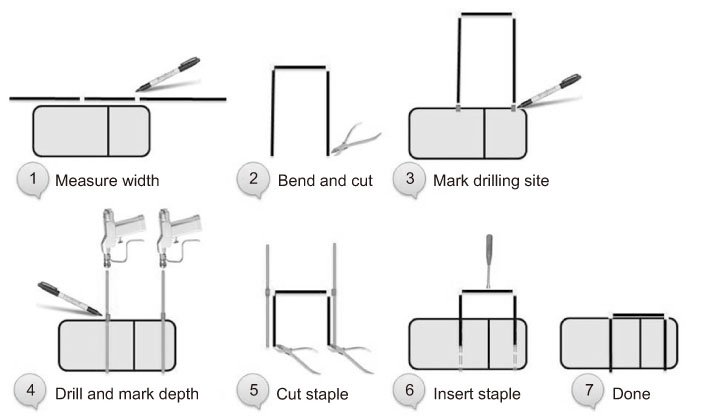
Fig. 2
Procedure of customized K-wire stapling technique.

Fig. 3
(A) 5th metacarpal neck fracture with 31° dorsal angulation after trauma. (B) Postoperative x-ray shows reduction and secure fixation of the fracture site using 2 staple fixation. (C) Staples were removed 3 months after trauma.
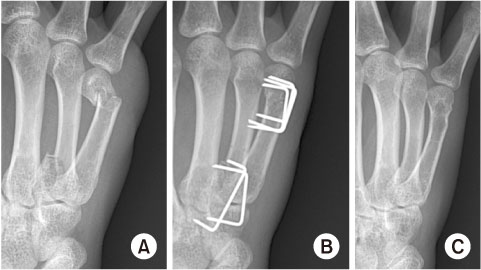
Fig. 4
(A) Fracture and lateral subluxation of the 4th metacarpal base, and 68° dorsal angulation after a punch injury with closed fist. (B) Postoperative x-ray shows reduction and secure fixation of the fracture site. (C) Staples were removed 1 year after trauma.

Fig. 5
At 1-year follow-up, normal total active motion of digits was restored without deformity or angulation.
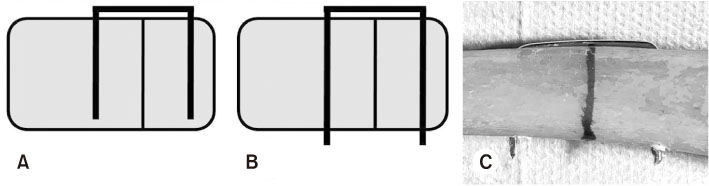
Fig. 6
(A) Conventional unicortical staple fixation method, ordinary staple. (B, C) Bicortical fixation of the K-wire staple.
Notes
Financial support:None.
Conflict of interests:None.
References
-
Nakashian MN, Pointer L, Owens BD, Wolf JM. Incidence of metacarpal fractures in the US population. Hand. N Y 2012;7:426–430.
-
-
Diaz-Garcia R, Waljee JF. Current management of metacarpal fractures. Hand Clin 2013;29:507–518.
-
-
Ali A, Hamman J, Mass DP. The biomechanical effects of angulated boxer’s fractures. J Hand Surg Am 1999;24:835–844.
-
-
Weinstein LP, Hanel DP. Metacarpal fractures. J Am Soc Surg Hand 2002;2:168–180.
-
-
Markiewitz AD. Complications of hand fractures and their prevention. Hand Clin 2013;29:601–620.
-
-
Low CK, Wong HC, Low YP, Wong HP. A cadaver study of the effects of dorsal angulation and shortening of the metacarpal shaft on the extension and flexion force ratios of the index and little fingers. J Hand Surg Br 1995;20:609–613.
-
-
Jahss SA. Fractures of the metacarpals: a new method of reduction and immobilization. J Bone Joint Surg 1938;20:178–186.
-
-
Harris AR, Beckenbaugh RD, Nettrour JF, Rizzo M. Metacarpal neck fractures: results of treatment with traction reduction and cast immobilization. Hand. N Y 2009;4:161–164.
-
-
Padegimas EM, Warrender WJ, Jones CM, Ilyas AM. Metacarpal neck fractures: a review of surgical indications and techniques. Arch Trauma Res 2016;5:e32933
-
-
Paul AS, Kurdy N, Kay PR. Fixation of closed metacarpal shaft fractures. Transverse K-wires in 22 cases. Acta Orthop Scand 1994;65:427–429.
-
-
Choi SJ, Chang SK. Treatment method of the metacarpal bone fractures with retrograde percutaneous intramedullary K-wire fixation to decrease the injury of extensor tendon. J Korean Soc Surg Hand 2004;9:117–122.
-
-
Hargreaves DG, Drew SJ, Eckersley R. Kirschner wire pin tract infection rates: a randomized controlled trial between percutaneous and buried wires. J Hand Surg Br 2004;29:374–376.
-
-
Kim TH, Kim BH, Jung IH, Kim DH. Antegrade intramedullary prebent K-wire fixation for the 5th metacarpal neck fracture. J Korean Fract Soc 2011;24:67–72.
-
-
Facca S, Ramdhian R, Pelissier A, Diaconu M, Liverneaux P. Fifth metacarpal neck fracture fixation: locking plate versus K-wire? Orthop Traumatol Surg Res 2010;96:506–512.
-
-
Page SM, Stern PJ. Complications and range of motion following plate fixation of metacarpal and phalangeal fractures. J Hand Surg Am 1998;23:827–832.
-
-
Feehan LM, Bassett K. Is there evidence for early mobilization following an extraarticular hand fracture? J Hand Ther 2004;17:300–308.
-
-
Feehan LM. Early controlled mobilization of potentially unstable extra-articular hand fractures. J Hand Ther 2003;16:161–170.
-
-
Freeland AE, Zardiackas LD, Terral GT, Blickentaff KR. Mechanical properties of 3M staples in bone block models. Orthopedics 1992;15:727–731.
-
-
Kwon GD, Yeo YB, Rho JH, et al. Biomechanical study of fixation methods for comminuted phalangeal fractures. J Korean Soc Surg Hand 2006;11:221–226.
-
-
Hoon QJ, Pelletier MH, Christou C, Johnson KA, Walsh WR. Biomechanical evaluation of shape-memory alloy staples for internal fixation-an in vitro study. J Exp Orthop 2016;3:19
-
 Cite
Cite
