 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 25(1); 2012 > Article
-
Original Article
- Risk Factors of Periprosthetic Fracture after Total Knee Arthroplasty
- Ju-Young Shin, M.D., Hyung-Jun Kim, M.D., Seung-Han Cha, M.D., Dong-Heon Kim, M.D.
-
Journal of the Korean Fracture Society 2012;25(1):1-7.
DOI: https://doi.org/10.12671/jkfs.2012.25.1.1
Published online: January 31, 2012
Department of Orthopaedic Surgery, College of Medicine, Konkuk University, Chungju, Korea.
- Address reprint requests to: Dong-Heon Kim, M.D. Department of Orthopaedic Surgery, College of Medicine, Konkuk University, 620-5, Kyohyun-dong, Chungju 380-704, Korea. Tel: 82-43-840-8250, Fax: 82-43-844-7300, kdkim@kku.ac.kr
• Received: March 1, 2011 • Revised: May 31, 2011 • Accepted: November 22, 2011
Copyright © 2012 The Korean Fracture Society
- 1,056 Views
- 2 Download
- 1 Crossref
Abstract
-
Purpose
- To evaluate the incidence rate and risk factors for periprosthetic fracture after total knee replacement (TKR).
-
Materials and Methods
- We carried out a retrospective case-control study of 596 patients (951 knees) who underwent TKR between 1999 and 2006 and who were followed up over 36 months. We classified patients into group I (study group) and group II (control group). We subdivided risk factors as pre-operative, intra-operative, and post-operative factors. Age, osteoporosis, revision arthroplasty, CVA, and alcohol dependence were categorized as pre-operative factors; anterior femoral notching and prosthetic types (mobile, fixed, and load-bearing) were considered intra-operative factors; and post-operative activity level was classified as a post-operative factor. We obtained information from the patients' charts, X-ray film, and telephone interviews.
-
Results
- The overall incidence rate was 2.25%; 3 patients were male, and 18 were female (14.28% and 85.72%, respectively). Old age (p<0.01, odds ratio=1.14), osteoporosis (p=0.01, odds ratio=4.74), revision arthroplasty (p=0.01, odds ratio=7.46), CVA (p=0.02, odds ratio=8.55), and alcohol dependence (p=0.03, odds ratio=44.54) were statistically significant among the pre-operative factors. Among the intra-operative factors, anterior femoral notching (p<0.01, odds ratio=11.74) was significant, and continued heavy labor (p<0.01, odds ratio=8.14) was significant among the post-operative factors.
-
Conclusion
- We concluded that old age, osteoporosis, revision arthroplasty, comorbidity related with falling down, anterior femoral notching, and continued heavy labor were associated with periprosthetic fracture after TKR.
- 1. Aaron RK, Scott R. Supracondylar fracture of the femur after total knee arthroplasty. Clin Orthop Relat Res, 1987;(219):136-139.Article
- 2. Bassey EJ, Dallosso HM, Fentem PH, Irving JM, Patrick JM. Validation of a simple mechanical accelerometer (pedometer) for the estimation of walking activity. Eur J Appl Physiol Occup Physiol, 1987;56:323-330.ArticlePubMedPDF
- 3. Bergland A, Jarnlo GB, Laake K. Predictors of falls in the elderly by location. Aging Clin Exp Res, 2003;15:43-50.ArticlePubMedPDF
- 4. Bhattacharyya T, Chang D, Meigs JB, Estok DM 2nd, Malchau H. Mortality after periprosthetic fracture of the femur. J Bone Joint Surg Am, 2007;89:2658-2662.Article
- 5. Blatter G, Fiechter T, Magerl F. Peri-prosthesis fractures in total hip endoprostheses. Orthopade, 1989;18:545-551.
- 6. Cain PR, Rubash HE, Wissinger HA, McClain EJ. Periprosthetic femoral fractures following total knee arthroplasty. Clin Orthop Relat Res, 1986;(208):205-214.Article
- 7. Cameron HU, Fedorkow DM. The patella in total knee arthroplasty. Clin Orthop Relat Res, 1982;(165):197-199.Article
- 8. Cook PJ, Exton-Smith AN, Brocklehurst JC, Lempert-Barber SM. Fractured femurs, falls and bone disorders. J R Coll Physicians Lond, 1982;16:45-49.ArticlePubMedPMC
- 9. Culp RW, Schmidt RG, Hanks G, Mak A, Esterhai JL Jr, Heppenstall RB. Supracondylar fracture of the femur following prosthetic knee arthroplasty. Clin Orthop Relat Res, 1987;(222):212-222.Article
- 10. Dahm DL, Barnes SA, Harrington JR, Sayeed SA, Berry DJ. Patient-reported activity level after total knee arthroplasty. J Arthroplasty, 2008;23:401-407.Article
- 11. Delport PH, Van Audekercke R, Martens M, Mulier JC. Conservative treatment of ipsilateral supracondylar femoral fracture after total knee arthroplasty. J Trauma, 1984;24:846-849.ArticlePubMed
- 12. Dennis DA. Periprosthetic fractures following total knee arthroplasty. J Bone Joint Surg Am, 2001;83:120. Article
- 13. Felix NA, Stuart MJ, Hanssen AD. Periprosthetic fractures of the tibia associated with total knee arthroplasty. Clin Orthop Relat Res, 1997;(345):113-124.Article
- 14. Figgie MP, Goldberg VM, Figgie HE III, Sobel M. The results of treatment of supracondylar fracture above total knee arthroplasty. J Arthroplasty, 1990;5:267-276.ArticlePubMed
- 15. Grace JN, Sim FH. of the patella after total knee arthroplasty. Clin Orthop Relat Res, 1988;(230):168-175.
- 16. Gujarathi N, Putti AB, Abboud RJ, MacLean JG, Espley AJ, Kellett CF. Risk of periprosthetic fracture after anterior femoral notching. Acta Orthop, 2009;80:553-556.Article
- 17. Hirsh DM, Bhalla S, Roffman M. Supracondylar fracture of the femur following total knee replacement. Report of four cases. J Bone Joint Surg Am, 1981;63:162-163.Article
- 18. Huch K, Müller KA, Stürmer T, Brenner H, Günther KP. Sports activities 5 years after total knee or hip arthroplasty: the Ulm Osteoarthritis Study. Ann Rheum Dis, 2005;64:1715-1720.Article
- 19. Jones DL, Cauley JA, Kriska AM, et al. Physical activity and risk of revision total knee arthroplasty in individuals with knee osteoarthritis: a matched case-control study. J Rheumatol, 2004;31:1384-1390.
- 20. Kim KI, Egol KA, Hozack WJ, Parvizi J. Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res, 2006;446:167-175.Article
- 21. Kuster MS. Exercise recommendations after total joint replacement: a review of the current literature and proposal of scientifically based guidelines. Sports Med, 2002;32:433-445.
- 22. Lavernia CJ, Sierra RJ, Hungerford DS, Krackow K. Activity level and wear in total knee arthroplasty: a study of autopsy retrieved specimens. J Arthroplasty, 2001;16:446-453.
- 23. Lesh ML, Schneider DJ, Deol G, Davis B, Jacobs CR, Pellegrini VD Jr. The consequences of anterior femoral notching in total knee arthroplasty. A biomechanical study. J Bone Joint Surg Am, 2000;82-A:1096-1101.
- 24. Marx RG, Jones EC, Atwan NC, Closkey RF, Salvati EA, Sculco TP. Measuring improvement following total hip and knee arthroplasty using patient-based measures of outcome. J Bone Joint Surg Am, 2005;87:1999-2005.Article
- 25. Merkel KD, Johnson EW Jr. Supracondylar fracture of the femur after total knee arthroplasty. J Bone Joint Surg Am, 1986;68:29-43.Article
- 26. Mont MA, Marker DR, Seyler TM, Gordon N, Hungerford DS, Jones LC. Knee arthroplasties have similar results in high- and low-activity patients. Clin Orthop Relat Res, 2007;460:165-173.Article
- 27. Petersen MM, Lauritzen JB, Pedersen JG, Lund B. Decreased bone density of the distal femur after uncemented knee arthroplasty. A 1-year follow-up of 29 knees. Acta Orthop Scand, 1996;67:339-344.Article
- 28. Rand JA, Coventry MB. Stress fractures after total knee arthroplasty. J Bone Joint Surg Am, 1980;62:226-233.Article
- 29. Ritter MA, Thong AE, Keating EM, et al. The effect of femoral notching during total knee arthroplasty on the prevalence of postoperative femoral fractures and on clinical outcome. J Bone Joint Surg Am, 2005;87:2411-2414.Article
- 30. Shawen SB, Belmont PJ Jr, Klemme WR, Topoleski LD, Xenos JS, Orchowski JR. Osteoporosis and anterior femoral notching in periprosthetic supracondylar femoral fractures: a biomechanical analysis. J Bone Joint Surg Am, 2003;85-A:115-121.
- 31. Sheth NP, Pedowitz DI, Lonner JH. Periprosthetic patellar fractures. J Bone Joint Surg Am, 2007;89:2285-2296.Article
- 32. Zahiri CA, Schmalzried TP, Szuszczewicz ES, Amstutz HC. Assessing activity in joint replacement patients. J Arthroplasty, 1998;13:890-895.Article
REFERENCES
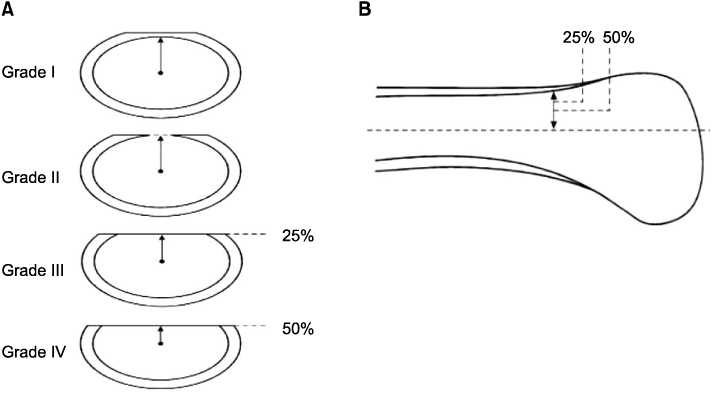
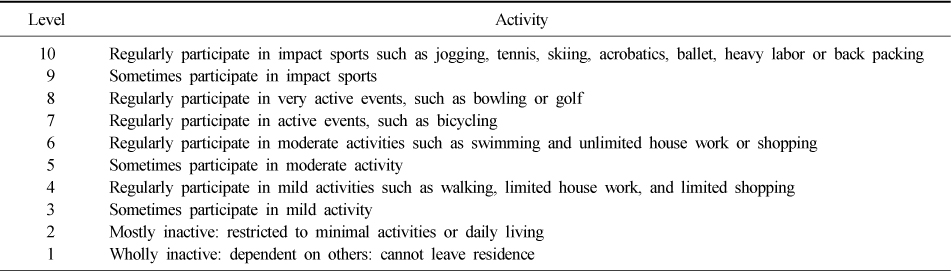
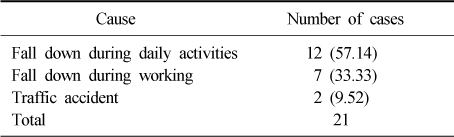
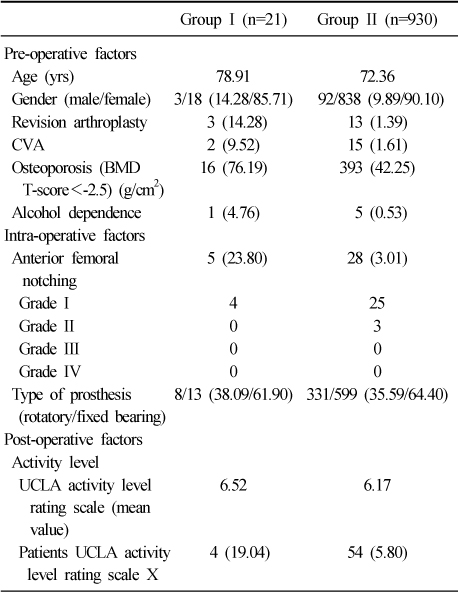
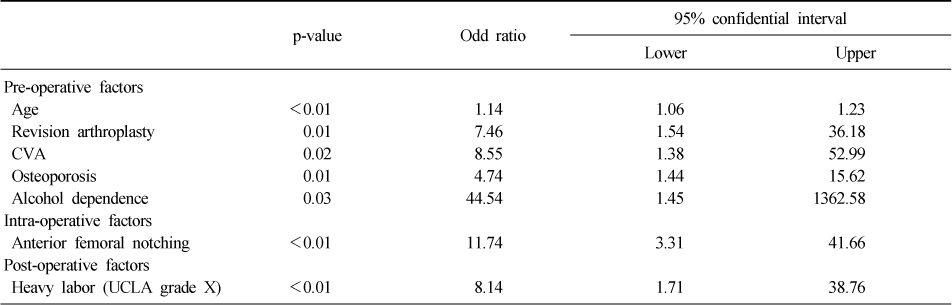
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Periprosthetic Distal Femoral Fracture Following Total Knee Arthroplasty Associated With Anterior Femoral Notching: A Case Report
Nay Aung Zin, Thiha Zaw, Sandar Shune Let Aung, Min Maung Maung, Htoo Aung Naing Shwe, Tun Tun
Cureus.2026;[Epub] CrossRef
 Cite
CiteRisk Factors of Periprosthetic Fracture after Total Knee Arthroplasty
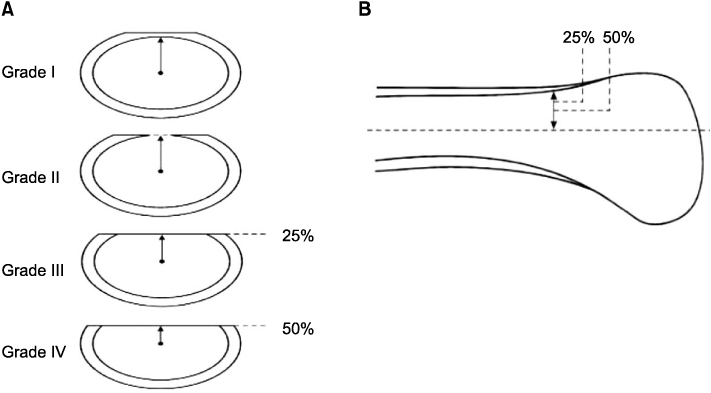
Fig. 1
(A) Tansverse sections of the distal femur showing notching.
(B) Sagittal section of the distal femur demonstrating grade III and IV notching.
Fig. 1
Risk Factors of Periprosthetic Fracture after Total Knee Arthroplasty
UCLA activity-level rating system
The cause of periprosthetic supracondylar fracture
Summary of patient's data
Risk factors by Multi-variable logistic regression
Table 1
UCLA activity-level rating system
Table 2
The cause of periprosthetic supracondylar fracture
Table 3
Summary of patient's data
Table 4
Risk factors by Multi-variable logistic regression

