 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 26(1); 2013 > Article
-
Original Article
- Coracoclavicular Screw Fixation and Tension Band Wiring in Treatment of Distal Clavicle Fracture
- Dae Gyu Kwon, M.D., Tong Joo Lee, M.D., Ph.D., Kyung Ho Moon, M.D., Ph.D., Byoung Ki Shin, M.D., Min Su Woo, M.D.
-
Journal of the Korean Fracture Society 2013;26(1):1-7.
DOI: https://doi.org/10.12671/jkfs.2013.26.1.1
Published online: January 17, 2013
Department of Orthopaedic Surgery, Inha University Hospital, Inha University School of Medicine, Incheon, Korea.
- Address reprint requests to: Tong Joo Lee, M.D., Ph.D. Department of Orthopaedic Surgery, Inha University Hospital, 27, Inhang-ro, Jung-gu, Incheon 400-711, Korea. Tel: 82-32-890-3044, Fax: 82-32-890-3467, TJLee@inha.ac.kr
• Received: June 20, 2012 • Revised: September 14, 2012 • Accepted: November 14, 2012
Copyright © 2013 The Korean Fracture Society
- 1,084 Views
- 6 Download
Abstract
-
Purpose
- The purpose of this study was to analyze the effectiveness of coracoclavicular screw fixation with tension band wiring in the treatment of displaced distal clavicle fractures.
-
Materials and Methods
- From October 2006 to December 2010, 18 patients with Neer type 2 displaced distal clavicle fracture were surgically treated. Fixation was performed, using coracoclavicular screw with tension band wiring. Radiographic and clinical evaluation was performed and the University of California at Los Angeles (UCLA) shoulder rating scale was employed for the assessment of shoulder joint function.
-
Results
- Osseous union was achieved approximately 9.5 weeks (8-11 weeks) in all patients. After the union, the screw and wire were removed under local anesthesia. All patients returned to the normal shoulder range of motion. Loosening of the screw was seen in two patients and breakage was seen in one patient. However, we could not observe the delayed union and complications, such as infection and refracture. All but one patient showed excellent results according to the UCLA shoulder score at one year after the operation.
-
Conclusion
- Coracoclavicular screw fixation with tension band wiring in the treatment of displaced distal clavicle fractures is a clinically useful technique with good result and less complication.
- 1. Ballmer FT, Gerber C. Coracoclavicular screw fixation for unstable fractures of the distal clavicle. A report of five cases. J Bone Joint Surg Br, 1991;73:291-294.ArticlePDF
- 2. Bezer M, Aydin N, Guven O. The treatment of distal clavicle fractures with coracoclavicular ligament disruption: a report of 10 cases. J Orthop Trauma, 2005;19:524-528.PubMed
- 3. Brunner U, Habermeyer P, Schweiberer L. Special status of lateral clavicular fracture. Orthopade, 1992;21:163-171.PubMed
- 4. Fazal MA, Saksena J, Haddad FS. Temporary coracoclavicular screw fixation for displaced distal clavicle fractures. J Orthop Surg (Hong Kong), 2007;15:9-11.ArticlePubMedPDF
- 5. Harris RI, Wallace AL, Harper GD, Goldberg JA, Sonnabend DH, Walsh WR. Structural properties of the intact and the reconstructed coracoclavicular ligament complex. Am J Sports Med, 2000;28:103-108.ArticlePDF
- 6. Jin CZ, Kim HK, Min BH. Surgical treatment for distal clavicle fracture associated with coracoclavicular ligament rupture using a cannulated screw fixation technique. J Trauma, 2006;60:1358-1361.ArticlePubMed
- 7. Kao FC, Chao EK, Chen CH, Yu SW, Chen CY, Yen CY. Treatment of distal clavicle fracture using Kirschner wires and tension-band wires. J Trauma, 2001;51:522-525.Article
- 8. Kona J, Bosse MJ, Staeheli JW, Rosseau RL. Type II distal clavicle fractures: a retrospective review of surgical treatment. J Orthop Trauma, 1990;4:115-120.
- 9. Levy O. Simple, minimally invasive surgical technique for treatment of type 2 fractures of the distal clavicle. J Shoulder Elbow Surg, 2003;12:24-28.Article
- 10. López JM, Torrens C, León V, Marín M. Unusual fracture of distal third of the clavicle in a hockey player: case report and a new approach to treatment. Knee Surg Sports Traumatol Arthrosc, 1999;7:132-134.ArticlePDF
- 11. Moneim MS, Balduini FC. Coracoid fracture as a complication of surgical treatment by coracoclavicular tape fixation. A case report. Clin Orthop Relat Res, 1982;(168):133-135.
- 12. Murphy DF, Greene WB, Dameron TB Jr. Displaced olecranon fractures in adults. Clinical evaluation. Clin Orthop Relat Res, 1987;(224):215-223.Article
- 13. Neer CS 2nd. Fracture of the distal clavicle with detachment of the coracoclavicular ligaments in adults. J Trauma, 1963;3:99-110.Article
- 14. Neer CS 2nd. Fractures of the distal third of the clavicle. Clin Orthop Relat Res, 1968;58:43-50.
- 15. Nordqvist A, Petersson C, Redlund-Johnell I. The natural course of lateral clavicle fracture. 15 (11-21) year follow-up of 110 cases. Acta Orthop Scand, 1993;64:87-91.Article
- 16. Rijal L, Sagar G, Joshi A, Joshi KN. Modified tension band for displaced type 2 lateral end clavicle fractures. Int Orthop, 2012;36:1417-1422.ArticlePDF
- 17. Tambe AD, Motkur P, Qamar A, Drew S, Turner SM. Fractures of the distal third of the clavicle treated by hook plating. Int Orthop, 2006;30:7-10.ArticlePDF
- 18. Thomas PR, Richard EB, Christopher GM. AO principles of fracture management, 2007;2nd ed. New York, Thieme. 249-255.
- 19. Tiren D, van Bemmel AJ, Swank DJ, van der Linden FM. Hook plate fixation of acute displaced lateral clavicle fractures: mid-term results and a brief literature overview. J Orthop Surg Res, 2012;7:2. Article
- 20. Webber MC, Haines JF. The treatment of lateral clavicle fractures. Injury, 2000;31:175-179.Article
REFERENCES
Fig. 1
(A) After two K-wire inserted to the coracoid process, drill hole was made between them.
(B) Coracoclavicular screw is fixed with a tension band wiring.
(C) Superior view: We use interosseous augmentation sutures through drill holes in the distal clavicle tip and coracuclavicular screw head. The use of wire sutures separately in a figure-eight pattern.
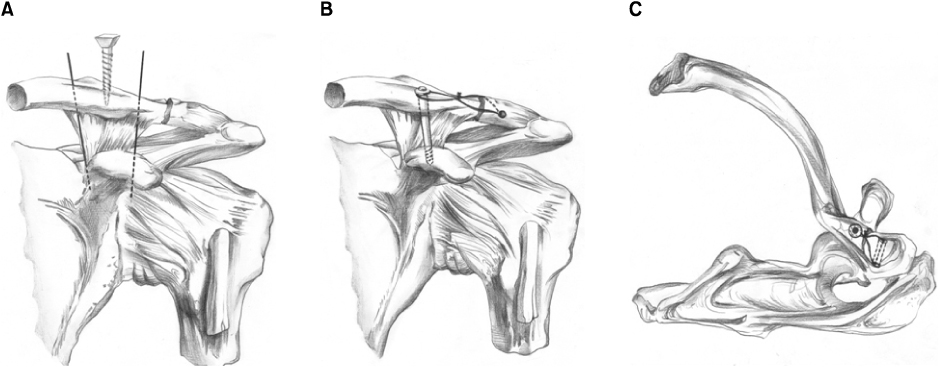
Fig. 2
(A) Initial radiograph showed a left type II fracture of the distal clavicle and significant displacement of the fracture.
(B) This radiograph showed that the fracture was reduced anatomically immediately after surgery.
(C) Radiograph 2 months after surgery showing that the fracture line was not clear and the alignment was well maintained.
(D) Radiograph showed that the fracture was united 6 months after surgery and after the implant had been removed.
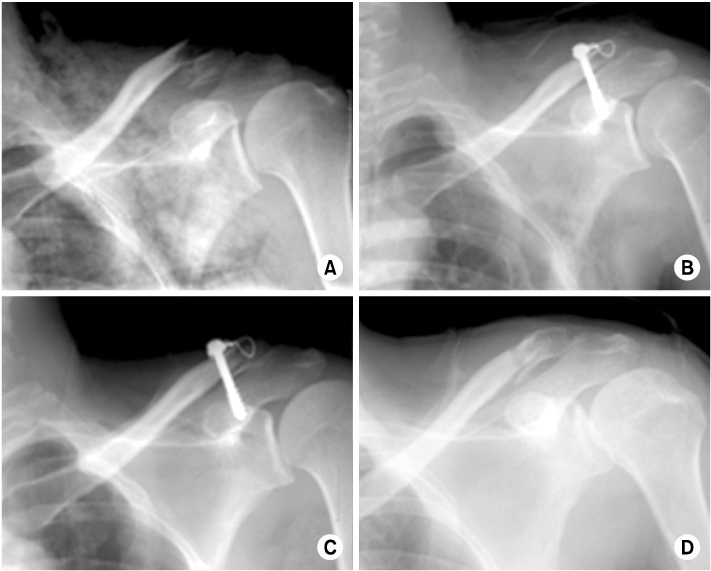
Fig. 3
(A) Initial radiograph showed a right type II fracture of the distal clavicle and significant displacement of the fracture.
(B) This radiograph showed that the fracture was reduced anatomically immediately after surgery.
(C) Radiograph 6 weeks after surgery showing the breakage of screw, which caused minimal displacement at the fracture site.
(D) Radiograph showed that the fracture was united 11 weeks after surgery and after the implant had been removed in spite of the broken screw.
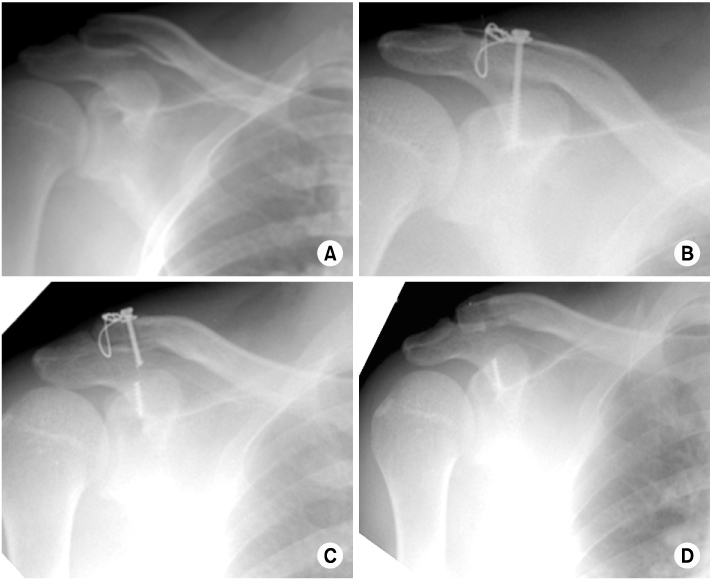
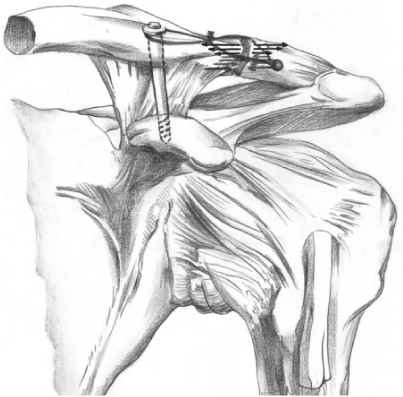
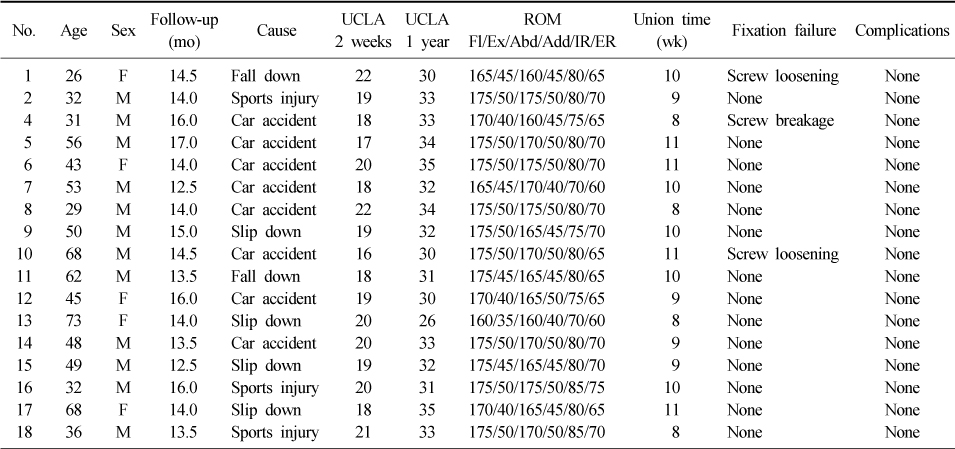
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteCoracoclavicular Screw Fixation and Tension Band Wiring in Treatment of Distal Clavicle Fracture
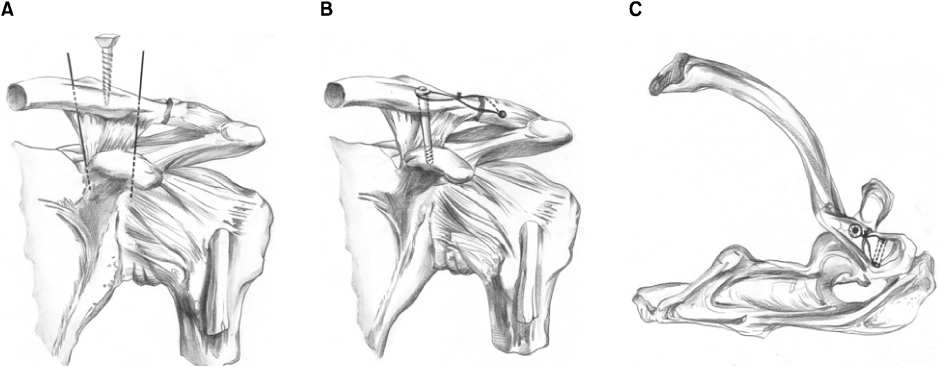
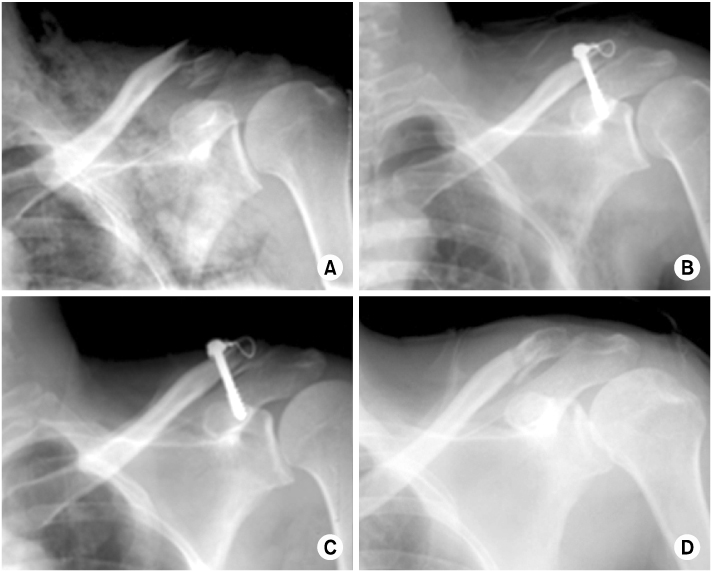
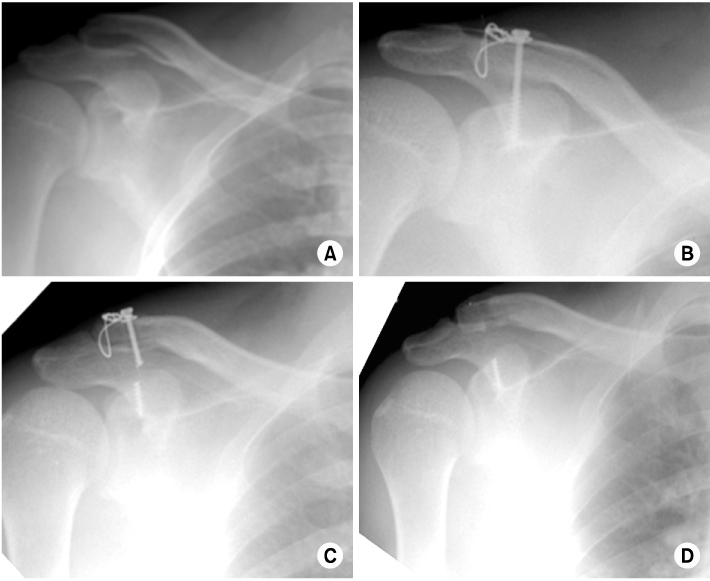
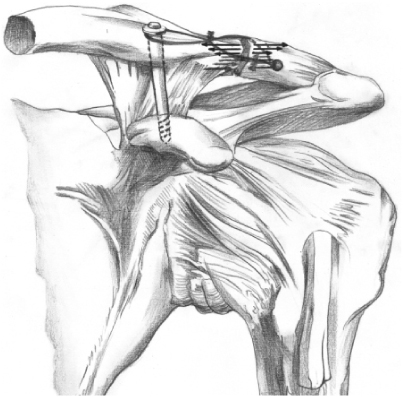
Fig. 1
(A) After two K-wire inserted to the coracoid process, drill hole was made between them.
(B) Coracoclavicular screw is fixed with a tension band wiring.
(C) Superior view: We use interosseous augmentation sutures through drill holes in the distal clavicle tip and coracuclavicular screw head. The use of wire sutures separately in a figure-eight pattern.
Fig. 2
(A) Initial radiograph showed a left type II fracture of the distal clavicle and significant displacement of the fracture.
(B) This radiograph showed that the fracture was reduced anatomically immediately after surgery.
(C) Radiograph 2 months after surgery showing that the fracture line was not clear and the alignment was well maintained.
(D) Radiograph showed that the fracture was united 6 months after surgery and after the implant had been removed.
Fig. 3
(A) Initial radiograph showed a right type II fracture of the distal clavicle and significant displacement of the fracture.
(B) This radiograph showed that the fracture was reduced anatomically immediately after surgery.
(C) Radiograph 6 weeks after surgery showing the breakage of screw, which caused minimal displacement at the fracture site.
(D) Radiograph showed that the fracture was united 11 weeks after surgery and after the implant had been removed in spite of the broken screw.
Fig. 4
Tension band was tied in a figure-eight manner, keeping the knot superiorly. The figure-eight wire loop acts as a tension band. Tension band converts tensile force into compression force at the opposite cortex.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Coracoclavicular Screw Fixation and Tension Band Wiring in Treatment of Distal Clavicle Fracture
Patient Demographic Data
UCLA: University of California at Los Angeles, ROM: Range of motion, Fl: Flexion, Ex: Extension, Abd: Abduction, Add: Adduction, IR: Internal rotation, ER: External rotation, F: Female, M: Male.
Table 1
Patient Demographic Data
UCLA: University of California at Los Angeles, ROM: Range of motion, Fl: Flexion, Ex: Extension, Abd: Abduction, Add: Adduction, IR: Internal rotation, ER: External rotation, F: Female, M: Male.

