 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 27(2); 2014 > Article
-
Review Article
- Current Concepts in Management of Pilon Fracture
- Jun-Young Lee, M.D., Sang-Joon Lee, M.D.
-
Journal of the Korean Fracture Society 2014;27(2):173-184.
DOI: https://doi.org/10.12671/jkfs.2014.27.2.173
Published online: April 18, 2014
Department of Orthopaedic Surgery, School of Medicine, Chosun University, Gwangju, Korea.
- Address reprint requests to: Jun-Young Lee, M.D. Department of Orthopaedic Surgery, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 501-717, Korea. Tel: 82-62-220-3147, Fax: 82-62-226-3379, leejy88@chosun.ac.kr
Copyright © 2014 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,468 Views
- 57 Download
- 1. Ovadia DN, Beals RK. Fractures of the tibial plafond. J Bone Joint Surg Am, 1986;68:543-551.ArticlePubMed
- 2. Rüedi T, Matter P, Allgöwer M. Intra-articular fractures of the distal tibial end. Helv Chir Acta, 1968;35:556-582.PubMed
- 3. Barei DP, Nork SE. Fractures of the tibial plafond. Foot Ankle Clin, 2008;13:571-591.ArticlePubMed
- 4. Bourne RB, Rorabeck CH, Macnab J. Intra-articular fractures of the distal tibia: the pilon fracture. J Trauma, 1983;23:591-596.PubMed
- 5. Egol KA, Wolinsky P, Koval KJ. Open reduction and internal fixation of tibial pilon fractures. Foot Ankle Clin, 2000;5:873-885.ArticlePubMed
- 6. Tornetta P 3rd, Gorup J. Axial computed tomography of pilon fractures. Clin Orthop Relat Res, 1996;(323):273-276.Article
- 7. Rüedi TP, Allgöwer M. The operative treatment of intra-articular fractures of the lower end of the tibia. Clin Orthop Relat Res, 1979;(138):105-110.PubMed
- 8. Tscherne H, Gotzen L. Fracutres with soft tissue injuries. Berlin, Heidelberg, NewYork, Tokyo: Springer-Verlag; 1984. p. 103-117.
- 9. Tull F, Borrelli J Jr. Soft-tissue injury associated with closed fractures: evaluation and management. J Am Acad Orthop Surg, 2003;11:431-438.ArticlePubMed
- 10. Wagner HE, Jakob RP. Plate osteosynthesis in bicondylar fractures of the tibial head. Unfallchirurg, 1986;89:304-311.PubMed
- 11. Wyrsch B, McFerran MA, McAndrew M, et al. Operative treatment of fractures of the tibial plafond. A randomized, prospective study. J Bone Joint Surg Am, 1996;78:1646-1657.ArticlePubMed
- 12. Coonrad RW. Fracture-dislocations of the ankle joint with impaction injury of the lateral weight-bearing surface of the tibia. J Bone Joint Surg Am, 1970;52:1337-1344.ArticlePubMed
- 13. Schatzker J, Tile M. The rationale of operative fracture care. 3rd ed. Berlin: Springer-Verlag; 2005. p. 523-550.
- 14. Gould JS. Reconstruction of soft tissue injuries of the foot and ankle with microsurgical techniques. Orthopedics, 1987;10:151-157.ArticlePubMed
- 15. Assal M, Ray A, Stern R. The extensile approach for the operative treatment of high-energy pilon fractures: surgical technique and soft-tissue healing. J Orthop Trauma, 2007;21:198-206.ArticlePubMed
- 16. Mehta S, Gardner MJ, Barei DP, Benirschke SK, Nork SE. Reduction strategies through the anterolateral exposure for fixation of type B and C pilon fractures. J Orthop Trauma, 2011;25:116-122.ArticlePubMed
- 17. Konrath GA, Hopkins G 2nd. Posterolateral approach for tibial pilon fractures: a report of two cases. J Orthop Trauma, 1999;13:586-589.ArticlePubMed
- 18. Kao KF, Huang PJ, Chen YW, Cheng YM, Lin SY, Ko SH. Postero-medio-anterior approach of the ankle for the pilon fracture. Injury, 2000;31:71-74.Article
- 19. Leonard M, Magill P, Khayyat G. Minimally-invasive treatment of high velocity intra-articular fractures of the distal tibia. Int Orthop, 2009;33:1149-1153.ArticlePubMedPDF
- 20. Tong D, Ji F, Zhang H, et al. Two-stage procedure protocol for minimally invasive plate osteosynthesis technique in the treatment of the complex pilon fracture. Int Orthop, 2012;36:833-837.ArticlePubMedPDF
- 21. Marcus MS, Yoon RS, Langford J, et al. Is there a role for intramedullary nails in the treatment of simple pilon fractures? Rationale and preliminary results. Injury, 2013;44:1107-1111.ArticlePubMed
- 22. Wang C, Li Y, Huang L, Wang M. Comparison of two-staged ORIF and limited internal fixation with external fixator for closed tibial plafond fractures. Arch Orthop Trauma Surg, 2010;130:1289-1297.ArticlePubMedPDF
- 23. Sohn HM, Lee JY, Ha SH, Lee SH, Lee GC, Seo KH. The results of two stage surgical treatment of pilon fractures. J Korean Fract Soc, 2012;25:177-184.Article
- 24. Collinge C, Sanders R, DiPasquale T. Treatment of complex tibial periarticular fractures using percutaneous techniques. Clin Orthop Relat Res, 2000;(375):69-77.Article
- 25. Thordarson DB. Complications after treatment of tibial pilon fractures: prevention and management strategies. J Am Acad Orthop Surg, 2000;8:253-265.ArticlePubMed
- 26. Pollak AN, McCarthy ML, Bess RS, Agel J, Swiontkowski MF. Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am, 2003;85:1893-1900.ArticlePubMed
- 27. Mader JT, Shirtliff M, Calhoun JH. Staging and staging application in osteomyelitis. Clin Infect Dis, 1997;25:1303-1309.ArticlePubMed
- 28. Zalavras CG, Patzakis MJ, Thordarson DB, Shah S, Sherman R, Holtom P. Infected fractures of the distal tibial metaphysis and plafond: achievement of limb salvage with free muscle flaps, bone grafting, and ankle fusion. Clin Orthop Relat Res, 2004;(427):57-62.
- 29. Feldman DS, Shin SS, Madan S, Koval KJ. Correction of tibial malunion and nonunion with six-axis analysis deformity correction using the Taylor Spatial Frame. J Orthop Trauma, 2003;17:549-554.ArticlePubMed
- 30. Cierny G 3rd, Cook WG, Mader JT. Ankle arthrodesis in the presence of ongoing sepsis. Indications, methods, and results. Orthop Clin North Am, 1989;20:709-721.PubMed
- 31. Morrey BF, Wiedeman GP Jr. Complications and long-term results of ankle arthrodeses following trauma. J Bone Joint Surg Am, 1980;62:777-784.ArticlePubMed
- 32. Knecht SI, Estin M, Callaghan JJ, et al. The agility total ankle arthroplasty. Seven to sixteen-year follow-up. J Bone Joint Surg Am, 2004;86:1161-1171.PubMed
- 33. Clare MP, Sanders RW. Preoperative considerations in ankle replacement surgery. Foot Ankle Clin, 2002;7:709-720.ArticlePubMed
- 34. Saltzman CL, Mann RA, Ahrens JE, et al. Prospective controlled trial of STAR total ankle replacement versus ankle fusion: initial results. Foot Ankle Int, 2009;30:579-596.ArticlePubMedPDF
- 35. SooHoo NF, Zingmond DS, Ko CY. Comparison of reoperation rates following ankle arthrodesis and total ankle arthroplasty. J Bone Joint Surg Am, 2007;89:2143-2149.ArticlePubMed
REFERENCES
Fig. 1Mechanism of the axial load type injury. The ultimate fracture pattern depends on the direction and rate of application of the injury force, and on the position of the foot at the time of loading.
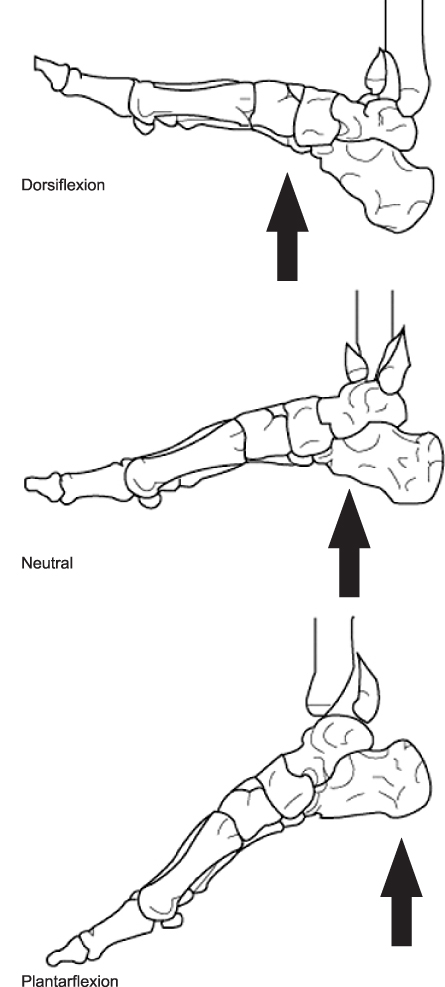
Fig. 2
(A) The patient has a pilon fracture with severe soft tissue swelling and blisters. (B, C) A temporary external fixator was applied in order to maintain the length and alignment of the lower leg and reduce the fracture.
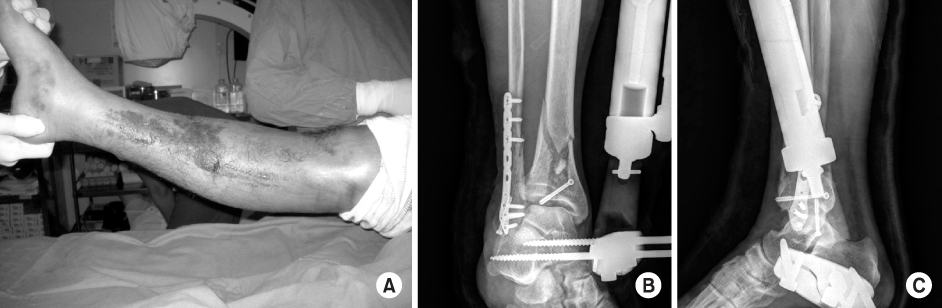
Fig. 3
(A) The surgical incision of the anteromedial approach to metaphysis and the ankle joint has been marked out on the patient's left ankle. (B) Deep surgical exposure of the ankle joint using an anteromedial approach. (C, D) Immediate postoperative radiographs show a satisfactory articular reduction and restoration of distal tibial alignment by semi-tubular plate (Synthes®).
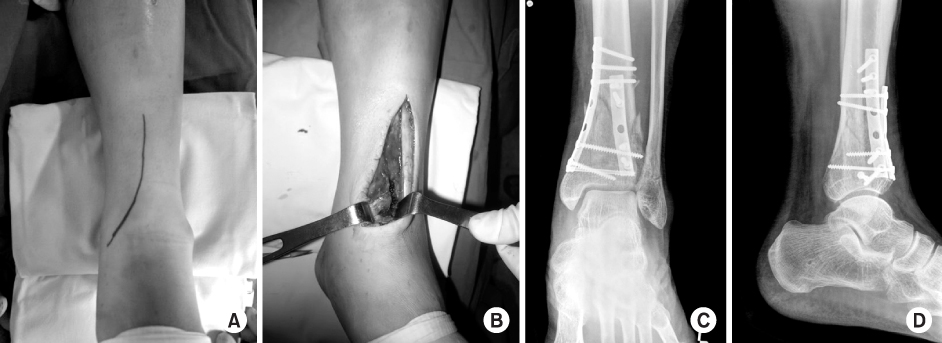
Fig. 4
(A, B) Injury anteroposterior and lateral radiographs of a displaced left tibial pilon fracture. (C) Large Volkmann fragment and Chaput fragment were observed. (D, E) Restoration of tibial length and joint spanning by temporary tibia external fixator. (F) Chaput fragment remained attached to the lateral malleolus; however, it was not reduced after reduction and plating of the associated fibular fracture. (G-J) Definitive open reduction and internal fixation was performed using an anterolateral surgical exposure and additional medial plating using the minimally invasive percutaneous osteosynthesis technique after resolution of soft tissue swelling.
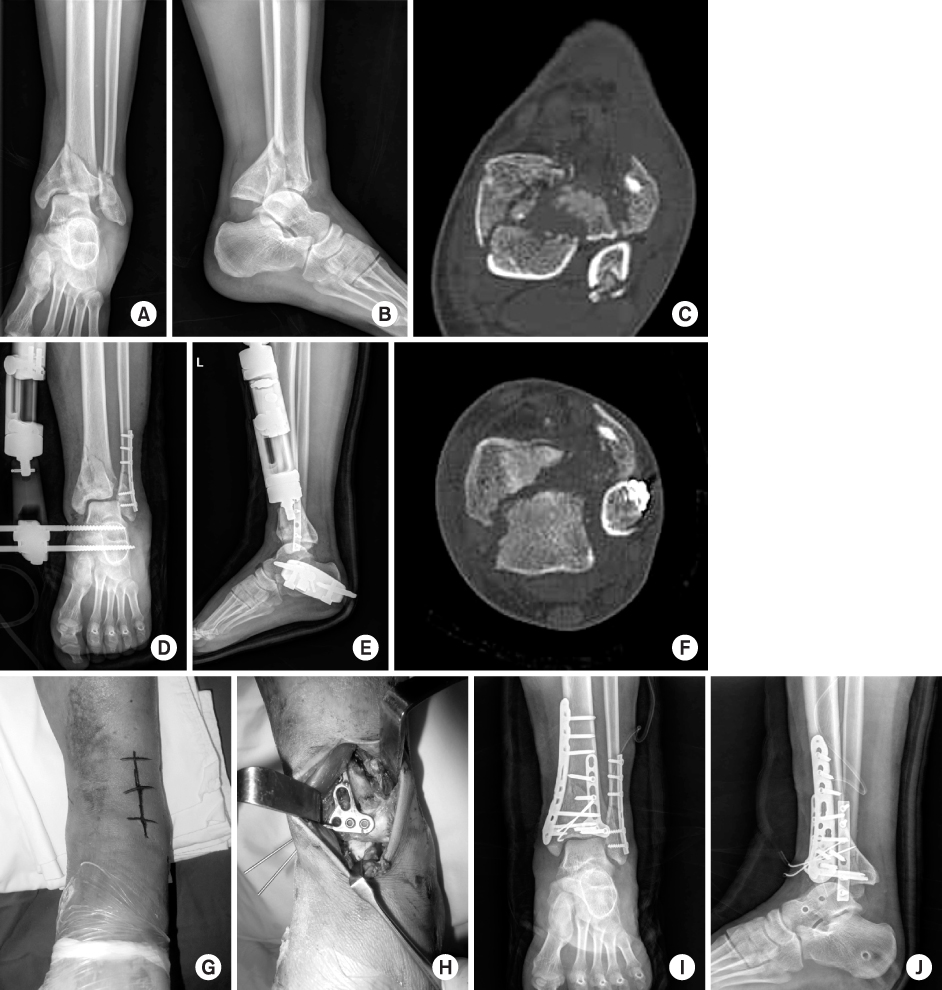
Fig. 5
(A) Surgical incision of the posterolateral approach and posterolateral fibular plating was performed. (B) Volkmann fragment was observed after retraction of the peroneal tendon and buttress plating was possible. (C, D) Postoperative radiographs show a satisfactory articular reduction and restoration of distal tibial alignment.
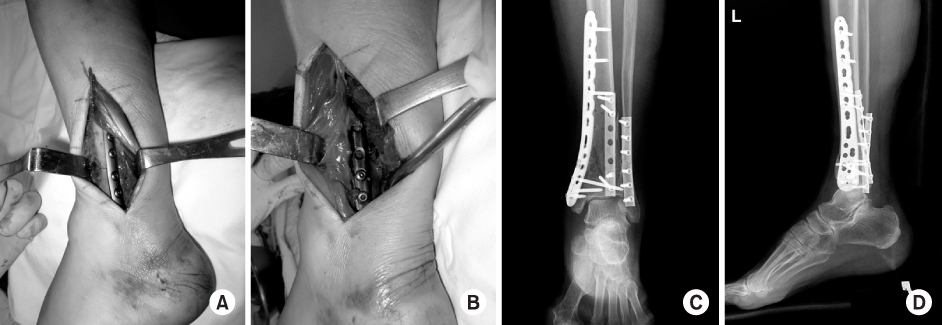
Fig. 6C3 pilon fracture with a medial open wound sustained by a male of 46 years (smoking history) as a result of a traffic accident. (A, B) Preoperative anteroposterior and lateral radiography. (C) Type II open wound at the medial aspect of the anterior tibia. (D, E) A temporary external fixator was applied in order to maintain the length and alignment of the lower leg and reduce the fracture. (F, G) Immediate postoperative radiographs show a satisfactory articular reduction and restoration of distal tibial alignment by locking the compression plate (Synthes®) in the second stage operation. (H-K) Bone union and satisfactory function of the ankle six months after the operation.

Fig. 7
(A) Initial photo of a pilon fracture with an open wound measuring 4 cm in size. (B) Photo of wound dehiscence three weeks after the initial injury. (C, D) It was treated with reverse sural artery flap.


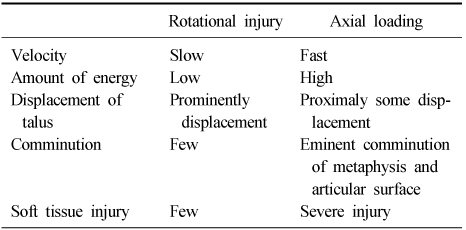
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 Cite
CiteCurrent Concepts in Management of Pilon Fracture
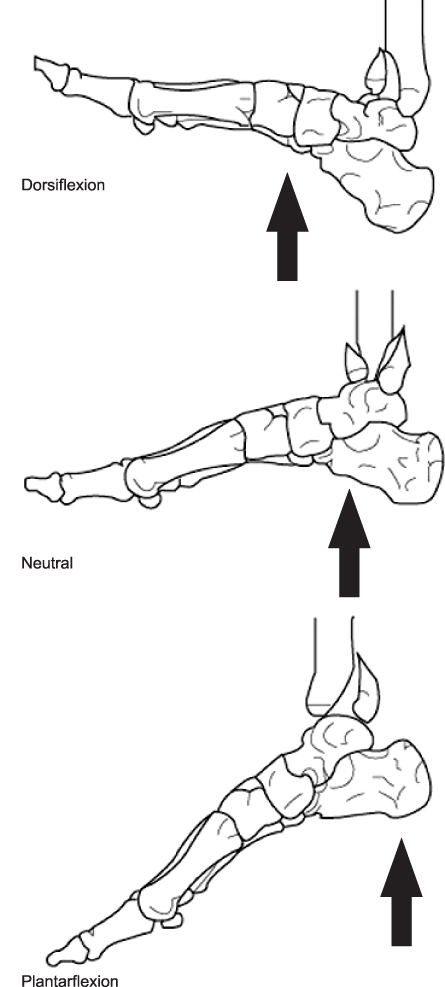
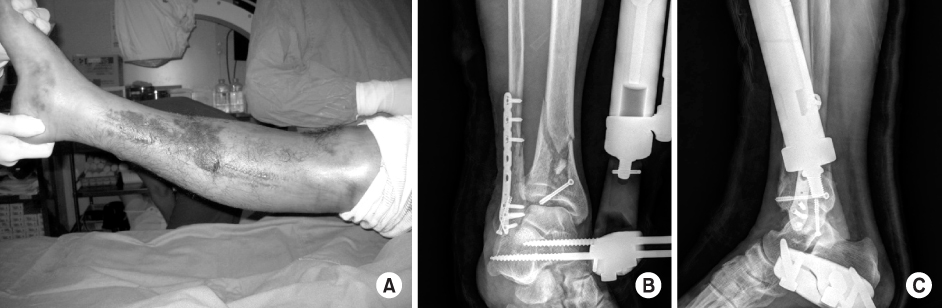
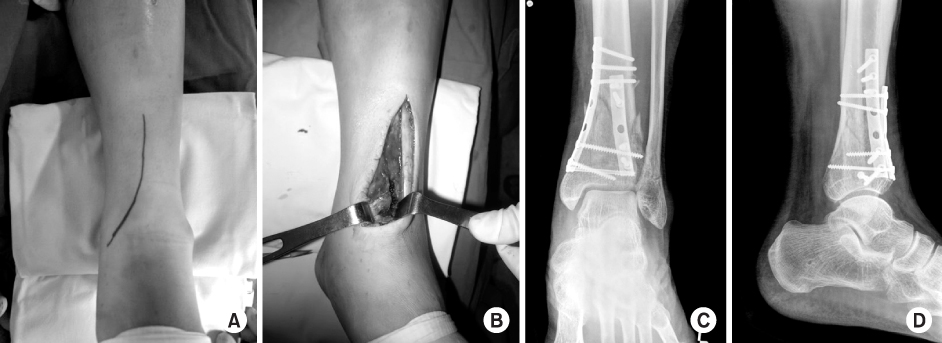
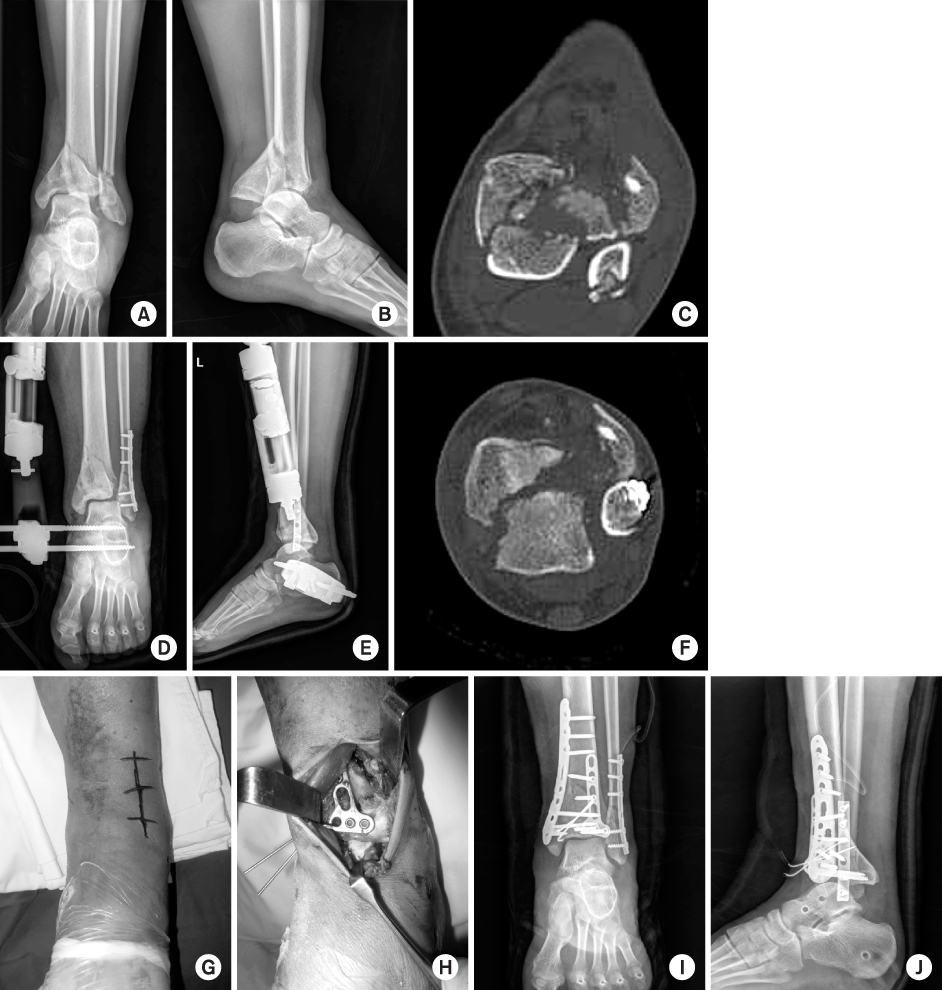
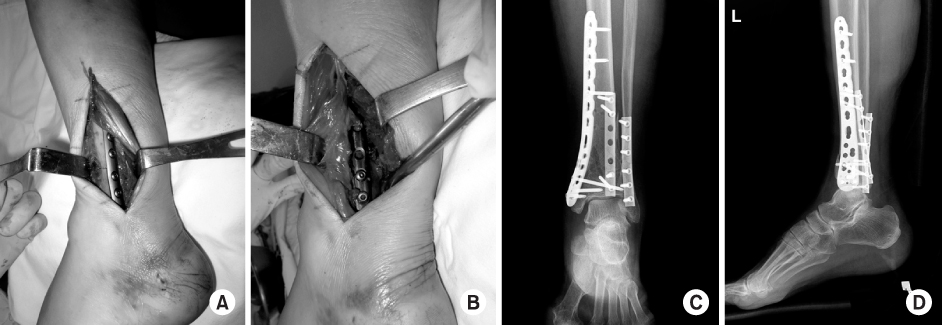



Fig. 1
Mechanism of the axial load type injury. The ultimate fracture pattern depends on the direction and rate of application of the injury force, and on the position of the foot at the time of loading.
Fig. 2
(A) The patient has a pilon fracture with severe soft tissue swelling and blisters. (B, C) A temporary external fixator was applied in order to maintain the length and alignment of the lower leg and reduce the fracture.
Fig. 3
(A) The surgical incision of the anteromedial approach to metaphysis and the ankle joint has been marked out on the patient's left ankle. (B) Deep surgical exposure of the ankle joint using an anteromedial approach. (C, D) Immediate postoperative radiographs show a satisfactory articular reduction and restoration of distal tibial alignment by semi-tubular plate (Synthes®).
Fig. 4
(A, B) Injury anteroposterior and lateral radiographs of a displaced left tibial pilon fracture. (C) Large Volkmann fragment and Chaput fragment were observed. (D, E) Restoration of tibial length and joint spanning by temporary tibia external fixator. (F) Chaput fragment remained attached to the lateral malleolus; however, it was not reduced after reduction and plating of the associated fibular fracture. (G-J) Definitive open reduction and internal fixation was performed using an anterolateral surgical exposure and additional medial plating using the minimally invasive percutaneous osteosynthesis technique after resolution of soft tissue swelling.
Fig. 5
(A) Surgical incision of the posterolateral approach and posterolateral fibular plating was performed. (B) Volkmann fragment was observed after retraction of the peroneal tendon and buttress plating was possible. (C, D) Postoperative radiographs show a satisfactory articular reduction and restoration of distal tibial alignment.
Fig. 6
C3 pilon fracture with a medial open wound sustained by a male of 46 years (smoking history) as a result of a traffic accident. (A, B) Preoperative anteroposterior and lateral radiography. (C) Type II open wound at the medial aspect of the anterior tibia. (D, E) A temporary external fixator was applied in order to maintain the length and alignment of the lower leg and reduce the fracture. (F, G) Immediate postoperative radiographs show a satisfactory articular reduction and restoration of distal tibial alignment by locking the compression plate (Synthes®) in the second stage operation. (H-K) Bone union and satisfactory function of the ankle six months after the operation.
Fig. 7
(A) Initial photo of a pilon fracture with an open wound measuring 4 cm in size. (B) Photo of wound dehiscence three weeks after the initial injury. (C, D) It was treated with reverse sural artery flap.
Fig. 8
(A, B) Posttraumatic arthritis was developed by a pilon fracture. (C, D) Postoperative radiographs treated with total ankle arthroplasty.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Current Concepts in Management of Pilon Fracture
Comparison of Features between Rotational Injury and Axial Loading Injury
Table 1
Comparison of Features between Rotational Injury and Axial Loading Injury

