 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 24(4); 2011 > Article
-
Original Article
- Treatment of the Trimalleolar Fracture Using Posterolateral Approach: Minimum 2-year Follow Up Results
- Gwang Chul Lee, M.D., Jun-Young Lee, M.D., Sang-Ho Ha, M.D., Jae-Won You, M.D., Sang-Hong Lee, M.D., Hong-Moon Sohn, M.D., Ki-Young Nam, M.D., Kwang-Hyo Seo, M.D.
-
Journal of the Korean Fracture Society 2011;24(4):328-334.
DOI: https://doi.org/10.12671/jkfs.2011.24.4.328
Published online: October 30, 2011
Department of Orthopaedic Surgery, College of Medicine, Chosun University, Gwangju, Korea.
- Address reprint requests to: Jun-Young Lee, M.D. Department of Orthopaedic Surgery, Chosun University Hospital, 588, Seosuk-dong, Dong-gu, Gwangju 501-717, Korea. Tel: 82-62-220-3147, Fax: 82-62-226-3379, leejy88@chosun.ac.kr
• Received: January 4, 2011 • Revised: March 29, 2011 • Accepted: July 9, 2011
Copyright © 2011 The Korean Fracture Society
- 1,086 Views
- 3 Download
- 1 Crossref
Abstract
-
Purpose
- To analyze the long term follow up results of treatment with posterolateral approach and to investigate its usefulness in the patients of trimalleolar fracture with posterior fragment which is above 25% of articular involvement.
-
Materials and Methods
- There were 34 cases of trimalleolar fracture in our hospital from May 2004 to April 2008. We investigated 20 patients who underwent operation with the posterolateral approach and over-2 years follow up cases. The mean follow up period was 34 (24~58) months. Preoperative posterior malleolar fragment involved above 25% of articular surface in all cases and displaced more than 2 mm in 11 cases. We analyzed the radiologic type of posterior malleolar fragments and evaluated the function and pain through AOFAS score and complications.
-
Results
- All cases showed primary union at mean 13.1 weeks. The complications are that partial ankylosis result of soft tissue contracture is seen in 2 cases (10%) and post-traumatic arthritis is seen in 1 cases (5%) and 17 cases (85%) of all patients are showed excellent AOFAS score.
-
Conclusion
- The posterolateral approach is a valuable method because that it enables us to easily reduction and internal fixation of the posterior malleolus and lateral malleolus at one time and the results are satisfied for a long time follow up.
- 1. Burwell HN, Charnley AD. The treatment of displaced fractures at the ankle by rigid internal fixation and early joint movement. J Bone Joint Surg Br, 1965;47:634-660.ArticlePDF
- 2. Carr JB. Browner BD, Jupiter JB, Levine AM, Trafton PG. Malleolar fractures and softtissue injuries of the ankle. In: Browner: Skeletal Trauma: Basic Science, Management, and Reconstruction, 2003;3rd ed. St. Louis, MO, WB Saunders. 2307-2374.Article
- 3. Haraguchi N, Haruyama H, Toga H, Kato F. Pathoanatomy of posterior malleolar fractures of the ankle. J Bone Joint Surg Am, 2006;88:1085-1092.Article
- 4. Heim UF. Trimalleolar fractures: late results after fixation of the posterior fragment. Orthopedics, 1989;12:1053-1059.Article
- 5. Henderson MS. Trimalleolar fracture of the ankle. Surg Clin North Am, 1932;12:867-872.
- 6. Jarde O, Vives P, Havet E, Gouron R, Meunier W. Malleolar fractures. Predictive factors for secondary osteoarthritis. Retrospective study of 32 cases. Acta Orthop Belg, 2000;66:382-388.
- 7. Jaskulka RA, Ittner G, Schedl R. Fractures of the posterior tibial margin: their role in the prognosis of malleolar fractures. J Trauma, 1989;29:1565-1570.
- 8. Jeong HJ, Kim KC, Chung SW. Treatment of the posterior malleolar fracture. J Korean Soc Fract, 1998;11:924-931.Article
- 9. Jergesen F. Open reduction of fractures and dislocations of the ankle. Am J Surg, 1959;98:136-151.Article
- 10. Kim SJ, Choi IY, Ahn TK. A clinical study of the trimalleolar fracutes of the ankle. J Korean Soc Fract, 1989;2:145-154.Article
- 11. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int, 1994;15:349-353.ArticlePDF
- 12. Klossner O. Late results of operative and non-operative treatment of severe ankle fractures. A clinical study. Acta Chir Scand Suppl, 1962;Suppl 293. 1-93.
- 13. Langenhuijsen JF, Heetveld MJ, Ultee JM, Steller EP, Butzelaar RM. Results of ankle fractures with involvement of the posterior tibial margin. J Trauma, 2002;53:55-60.Article
- 14. Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg, 1950;60:957-985.Article
- 15. Lauge N. Fractures of the ankle; analytic historic survey as the basis of new experimental, roentgenologic and clinical investigations. Arch Surg, 1948;56:259-317.
- 16. Lee JY, Ha SH, Noh KH, Lee SJ. Treatment of the posterior malleolar fragment of trimalleolar fracture using posterolateral approach: preliminary report. J Korean Orthop Assoc, 2009;44:422-428.
- 17. Malka JS, Taillard W. Results of nonoperative and operative treatment of fractures of the ankle. Clin Orthop Relat Res, 1969;67:159-168.
- 18. Marsh JL, Saltzman CL. Rockwood and Green's fractures in adults, 2002;5th ed. Philadelphia, Lippincott Williams and Wilkins. 2001-2090.
- 19. McDaniel WJ, Wilson FC. Trimalleolar fractures of the ankle. An end result study. Clin Orthop Relat Res, 1977;122:37-45.
- 20. Miller AJ. Posterior malleolar fractures. J Bone Joint Surg Br, 1974;56B:508-512.
- 21. Phillips WA, Schwartz HS, Keller CS, et al. A prospective, randomized study of the management of severe ankle fractures. J Bone Joint Surg Am, 1985;67:67-78.
- 22. Roberts RS. Surgical treatment of displaced ankle fractures. Clin Orthop Relat Res, 1983;172:164-170.
- 23. Sachs W, Kanat IO, McLaughlin E, Burns DE. A surgical approach to a displaced ankle fracture. J Foot Surg, 1984;23:302-307.
- 24. Schaffer JJ, Manoli A 2nd. The antiglide plate for distal fibular fixation. A biomechanical comparison with fixation with a lateral plate. J Bone Joint Surg Am, 1987;69:596-604.
- 25. Sir Cooper A. A treatise on dislocations and on fractures of the joints: fractures of the neck of the thigh-bone. 1823. Clin Orthop Relat Res, 2007;458:6-7.
- 26. Talbot M, Steenblock TR, Cole PA. Posterolateral approach for open reduction and internal fixation of trimalleolar ankle fractures. Can J Surg, 2005;48:487-490.
REFERENCES
Fig. 1
Posterolateral approach.
(A) Longitudinal skin incision is placed just medial to the posterior border of the fibula.
(B) Retracting the peroneal tendons medially and fibular fracture is fixed with antiglide plate.
(C) Posterior fragment is exposured between peroneal tendons and the flexor hallucis longus tendon, and is fixed with 4.0 cannulated screw after reduction.
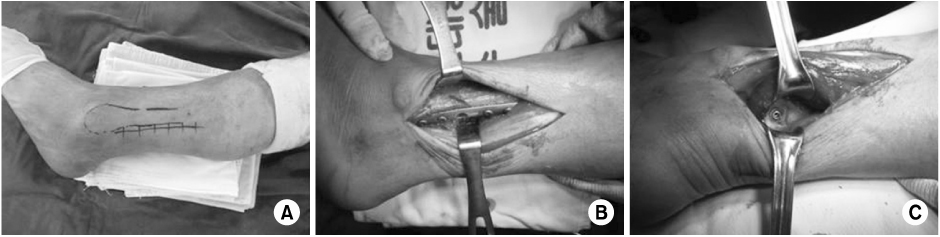
Fig. 2
(A, B) Anteroposterior and lateral radiographs showing a displaced trimalleolar fracture.
(C, D) Preoperative CT of the sagittal and axial view. It has posterolateral fragment.
(E~G) There is postoperative radiograph.


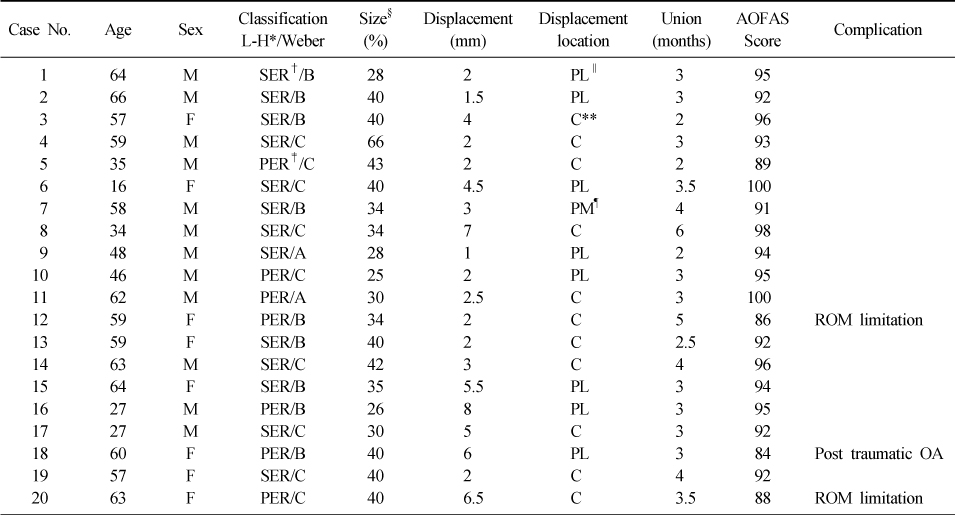
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Outcomes of Immediate Operative Treatment of Ankle Trimalleolar Open Fractures
Jun-Young Lee, Yong-Jin Cho, Sin-Wook Kang, Yung-Min Cho, Hyun-Bai Choi
Journal of Korean Foot and Ankle Society.2020; 24(1): 25. CrossRef
 Cite
CiteTreatment of the Trimalleolar Fracture Using Posterolateral Approach: Minimum 2-year Follow Up Results



Fig. 1
Posterolateral approach.
(A) Longitudinal skin incision is placed just medial to the posterior border of the fibula.
(B) Retracting the peroneal tendons medially and fibular fracture is fixed with antiglide plate.
(C) Posterior fragment is exposured between peroneal tendons and the flexor hallucis longus tendon, and is fixed with 4.0 cannulated screw after reduction.
Fig. 2
(A, B) Anteroposterior and lateral radiographs showing a displaced trimalleolar fracture.
(C, D) Preoperative CT of the sagittal and axial view. It has posterolateral fragment.
(E~G) There is postoperative radiograph.
Fig. 3
(A, B) Preoperative radiograph showing a displaced trimalleoar fracture.
(C, D) 6 months later postoperative radiograph showing a Post-traumatic OA (grade 4).
(E, F) Plate and screw is removed.
Fig. 1
Fig. 2
Fig. 3
Treatment of the Trimalleolar Fracture Using Posterolateral Approach: Minimum 2-year Follow Up Results
Data about the patients
*Lauge-Hansen, †Supination-external rotation, ‡Pronation-external rotation, §Joint involvement ratio of the posterior malleolar fragment, ∥Posterolateral, ¶Posteromedial, **Central.
Table 1
Data about the patients
*Lauge-Hansen, †Supination-external rotation, ‡Pronation-external rotation, §Joint involvement ratio of the posterior malleolar fragment, ∥Posterolateral, ¶Posteromedial, **Central.

