 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 32(4); 2019 > Article
- Review Article Total Hip Arthroplasty after Acetabular Fracture: Acute Phase and Delayed Phase
- Hwan Hee Lee, Se Won Lee, Weon Yoo Kim
-
Journal of Musculoskeletal Trauma 2019;32(4):232-239.
DOI: https://doi.org/10.12671/jkfs.2019.32.4.232
Published online: October 31, 2019
1Department of Orthopedic Surgery, Daejeon St. Mary's Hospital, School of Medicine, The Catholic University of Korea, Daejeon, Korea. weonyookim@gmail.com
2Department of Orthopedic Surgery, Yeouido St. Mary's Hospital, School of Medicine, The Catholic University of Korea, Seoul, Korea.
2Department of Orthopedic Surgery, Yeouido St. Mary's Hospital, School of Medicine, The Catholic University of Korea, Seoul, Korea.
- 1,812 Views
- 2 Download
- 1 Crossref
- 0 Scopus
Abstract
The incidence of acetabular fractures in the elderly has increased because of the increasing elderly population. To determine the treatment plan for acetabular fractures, the patient's age, gait ability, presence or absence of osteoporosis and osteoarthritis, underlying disease, and fracture pattern should be considered. The application of total hip arthroplasty for acetabular fractures with the proper indications can be expected to have a good prognosis. In this paper, the application of total hip arthroplasty as a treatment method for acetabular fractures is divided into acute and delayed phases.
J Korean Fract Soc. 2019 Oct;32(4):232-239. Korean.
Published online Oct 28, 2019.
https://doi.org/10.12671/jkfs.2019.32.4.232
Published online Oct 28, 2019.
https://doi.org/10.12671/jkfs.2019.32.4.232
Copyright © 2019 The Korean Fracture Society. All rights reserved.
Review
Total Hip Arthroplasty after Acetabular Fracture: Acute Phase and Delayed Phase

Abstract
The incidence of acetabular fractures in the elderly has increased because of the increasing elderly population. To determine the treatment plan for acetabular fractures, the patient's age, gait ability, presence or absence of osteoporosis and osteoarthritis, underlying disease, and fracture pattern should be considered. The application of total hip arthroplasty for acetabular fractures with the proper indications can be expected to have a good prognosis. In this paper, the application of total hip arthroplasty as a treatment method for acetabular fractures is divided into acute and delayed phases.
Keywords
Arthroplasty, Hip, Acetabulum, Osteoarthritis
Figures
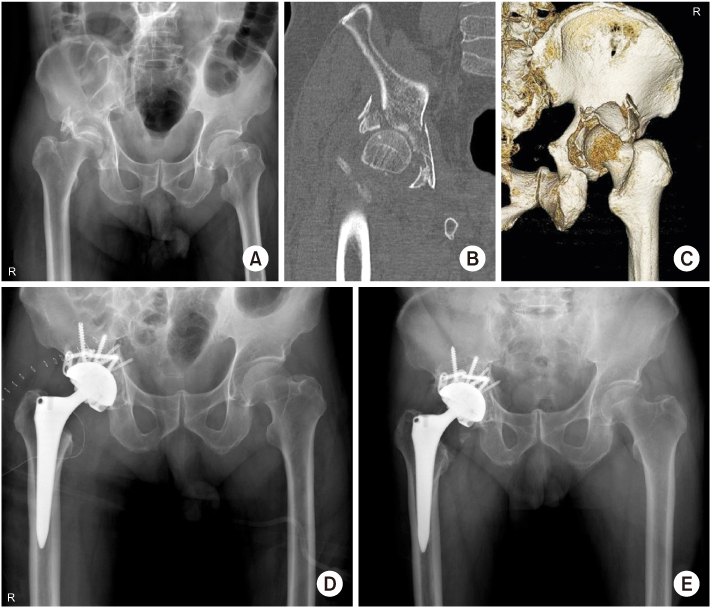
Fig. 1
(A) Preoperative anteroposterior radiograph of a 77-year-old male showed a posterior wall fracture with osteoporosis. (B, C) Computed tomography scan showed severe comminuted fracture of the posterior wall of the acetabulum and impaction of the femoral head. (D) Postoperative anteroposterior radiograph after internal fixation with total hip arthroplasty. (E) Four-year postoperative radiograph showed stable total hip component with bone union.
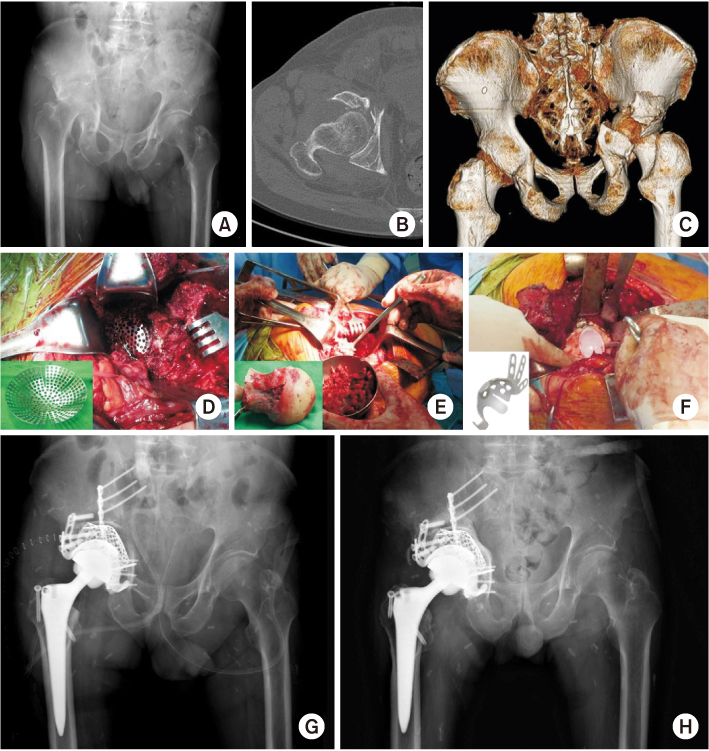
Fig. 2
(A) Preoperative anteroposterior radiograph of a 67-year-old male showed a transverse fracture with posterior wall fracture of the acetabulum and severe impaction. (B, C) Computed tomography showed a severe comminuted fracture of the posterior wall and protrusion of the femoral head. (D) The acetabular mesh plate was inserted into the acetabulum through the Kocher–Langenbeck approach. (E) Autogenous corticocancellous bone from the femoral head was grafted on a mesh plate to support the acetabular cup. (F) A liner was inserted after fixation of the cemented flanged acetabular cup. (G) Postoperative anteroposterior radiograph after internal fixation and total hip arthroplasty. (H) Three-year postoperative radiographs showed stable total hip arthroplasty.
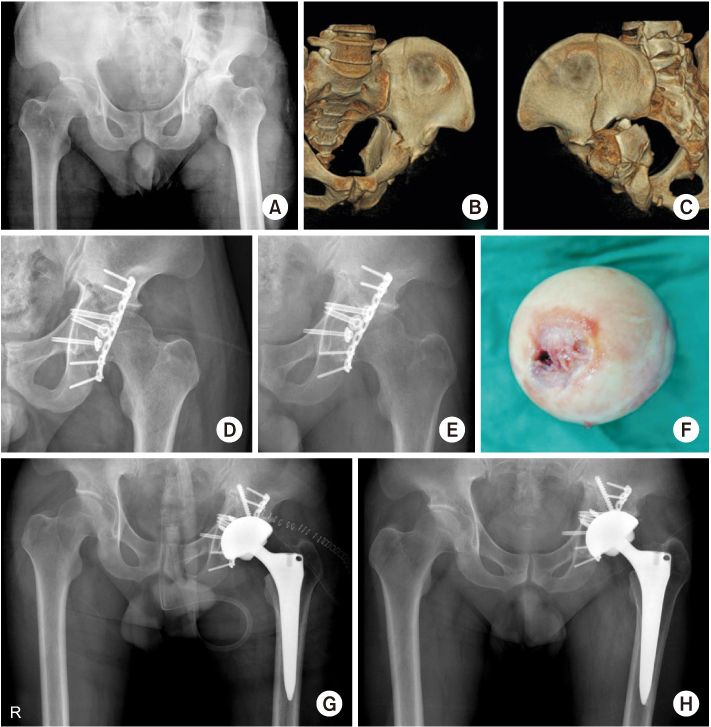
Fig. 3
(A) Preoperative anteroposterior radiograph of a 50-year-old male showed a transverse fracture with a posterior wall fracture of the acetabulum. (B, C) The three-dimensional reconstruction images showed the impaction of acetabulum and comminuted fragments. (D) Postoperative anteroposterior radiograph after internal fixation through the Kocher–Langenbeck approach. (E) Seven-month postoperative radiographs showed post-traumatic osteoarthritis on the left hip joint. (F) Intraoperatively, the resected femoral head showed denuded and destroyed articular cartilage. (G) Postoperative anteroposterior radiograph after total hip arthroplasty. (H) Five-year postoperative radiographs showed a stable total hip component with no complaint.
Tables
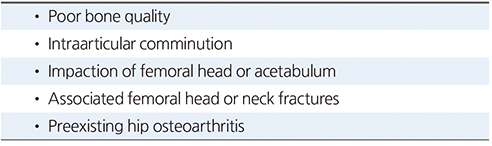
Table 1
Indications for Acute Total Hip Arthroplasty in Acetabular Fractures
Table 2
Indications for Delayed Total Hip Arthroplasty in Acetabular Fractures
Notes
Financial support:None.
Conflict of interests:None.
References
-
Laird A, Keating JF. Acetabular fractures: a 16-year prospective epidemiological study. J Bone Joint Surg Br 2005;87:969–973.
-
-
Werner CM, Copeland CE, Ruckstuhl T, Stromberg J, Turen CH, Bouaicha S. Acetabular fracture types vary with different acetabular version. Int Orthop 2012;36:2559–2563.
-
-
Lansinger O, Romanus B, Goldie IF. Fracture mechanism in central acetabular fractures. An experimental study. Arch Orthop Trauma Surg 1979;94:209–212.
-
-
Mears DC, Velyvis JH. Acute total hip arthroplasty for selected displaced acetabular fractures: two to twelve-year results. J Bone Joint Surg Am 2002;84:1–9.
-
-
Mears DC. Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128–141.
-
-
Matta JM, Merritt PO. Displaced acetabular fractures. Clin Orthop Relat Res 1988;(230):83–97.
-
-
Liebergall M, Mosheiff R, Low J, Goldvirt M, Matan Y, Segal D. Acetabular fractures. Clinical outcome of surgical treatment. Clin Orthop Relat Res 1999;(366):205–216.
-
-
Romness DW, Lewallen DG. Total hip arthroplasty after fracture of the acetabulum. Long-term results. J Bone Joint Surg Br 1990;72:761–764.
-
-
Berry DJ, Halasy M. Uncemented acetabular components for arthritis after acetabular fracture. Clin Orthop Relat Res 2002;(405):164–167.
-
-
Carroll EA, Huber FG, Goldman AT, et al. Treatment of acetabular fractures in an older population. J Orthop Trauma 2010;24:637–644.
-
-
Mouhsine E, Garofalo R, Borens O, et al. Acute total hip arthroplasty for acetabular fractures in the elderly: 11 patients followed for 2 years. Acta Orthop Scand 2002;73:615–618.
-
-
Uhl RL, Lozman J. Primary total hip arthroplasty for treatment of a geriatric acetabulum fracture. Orthopedics 2004;27:485–486.
-
-
Liporace FA, Yoon RS, Frank MA, Maurer JP, Gaines RJ. Single-stage total hip arthroplasty and fracture fixation for a both column acetabular fracture in type I osteogenesis imperfecta. Injury 2011;42:1184–1187.
-
-
Mears DC, Velyvis JH. Primary total hip arthroplasty after acetabular fracture. Instr Course Lect 2001;50:335–354.
-
-
Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am 1964;46:1615–1646.
-
-
Culemann U, Holstein JH, Köhler D, et al. Different stabilisation techniques for typical acetabular fractures in the elderly--a biomechanical assessment. Injury 2010;41:405–410.
-
-
Hessmann MH, Nijs S, Rommens PM. [Acetabular fractures in the elderly. Results of a sophisticated treatment concept]. Unfallchirurg 2002;105:893–900.German.
-
-
Jeffcoat DM, Carroll EA, Huber FG, et al. Operative treatment of acetabular fractures in an older population through a limited ilioinguinal approach. J Orthop Trauma 2012;26:284–289.
-
-
Ferguson TA, Patel R, Bhandari M, Matta JM. Fractures of the acetabulum in patients aged 60 years and older: an epidemiological and radiological study. J Bone Joint Surg Br 2010;92:250–257.
-
-
Guerado E, Cano JR, Cruz E. Surgical technique: intraacetabular osteosynthesis with arthroplasty for acetabular fracture in the octogenarian. Injury 2012;43:509–512.
-
-
Pagenkopf E, Grose A, Partal G, Helfet DL. Acetabular fractures in the elderly: treatment recommendations. HSS J 2006;2:161–171.
-
-
Matta JM, Anderson LM, Epstein HC, Hendricks P. Fractures of the acetabulum. A retrospective analysis. Clin Orthop Relat Res 1986;(205):230–240.
-
-
Spencer RF. Acetabular fractures in older patients. J Bone Joint Surg Br 1989;71:774–776.
-
-
Sen RK, Veerappa LA. Long-term outcome of conservatively managed displaced acetabular fractures. J Trauma 2009;67:155–159.
-
-
Magu NK, Rohilla R, Arora S. Conservatively treated acetabular fractures: a retrospective analysis. Indian J Orthop 2012;46:36–45.
-
-
Harper CM, Lyles YM. Physiology and complications of bed rest. J Am Geriatr Soc 1988;36:1047–1054.
-
-
Henry PD, Kreder HJ, Jenkinson RJ. The osteoporotic acetabular fracture. Orthop Clin North Am 2013;44:201–215.
-
-
Vanderschot P. Treatment options of pelvic and acetabular fractures in patients with osteoporotic bone. Injury 2007;38:497–508.
-
-
Antell NB, Switzer JA, Schmidt AH. Management of acetabular fractures in the elderly. J Am Acad Orthop Surg 2017;25:577–585.
-
-
Boettcher WG. Total hip arthroplasties in the elderly. Morbidity, mortality, and cost effectiveness. Clin Orthop Relat Res 1992;(274):30–34.
-
-
Starr AJ, Jones AL, Reinert CM, Borer DS. Preliminary results and complications following limited open reduction and percutaneous screw fixation of displaced fractures of the acetabulum. Injury 2001;32 Suppl 1:SA45–SA50.
-
-
Herscovici D Jr, Lindvall E, Bolhofner B, Scaduto JM. The combined hip procedure: open reduction internal fixation combined with total hip arthroplasty for the management of acetabular fractures in the elderly. J Orthop Trauma 2010;24:291–296.
-
-
Boraiah S, Ragsdale M, Achor T, Zelicof S, Asprinio DE. Open reduction internal fixation and primary total hip arthroplasty of selected acetabular fractures. J Orthop Trauma 2009;23:243–248.
-
-
Borg T, Hernefalk B, Hailer NP. Acute total hip arthroplasty combined with internal fixation for displaced acetabular fractures in the elderly: a short-term comparison with internal fixation alone after a minimum of two years. Bone Joint J 2019;101-B:478–483.
-
-
Jauregui JJ, Clayton A, Kapadia BH, Cherian JJ, Issa K, Mont MA. Total hip arthroplasty for acute acetabular fractures: a review of the literature. Expert Rev Med Devices 2015;12:287–295.
-
-
Pohlemann T, Culemann U. Summary of controversial debates during the 5th “Homburg Pelvic Course” 13-15 September 2006. Injury 2007;38:424–430.
-
-
Ranawat A, Zelken J, Helfet D, Buly R. Total hip arthroplasty for posttraumatic arthritis after acetabular fracture. J Arthroplasty 2009;24:759–767.
-
-
Sermon A, Broos P, Vanderschot P. Total hip replacement for acetabular fractures. Results in 121 patients operated between 1983 and 2003. Injury 2008;39:914–921.
-
-
Gavaskar AS, Gopalan H, Karthik B, Srinivasan P, Tummala NC. Delayed total hip arthroplasty for failed acetabular fractures: the influence of initial fracture management on outcome after arthroplasty. J Arthroplasty 2017;32:872–876.
-
 PubReader
PubReader Cite
Cite
