 E-submission
E-submission TOTA
TOTA TOTS
TOTS
Articles
- Page Path
- HOME > J Musculoskelet Trauma > Volume 20(3); 2007 > Article
-
Review Article
- Ankle Syndesmotic Injury
- Keun-Bae Lee
-
Journal of the Korean Fracture Society 2007;20(3):282-290.
DOI: https://doi.org/10.12671/jkfs.2007.20.3.282
Published online: June 14, 2016
Department of Orthopedic Surgery, Chonnam National University Hospital, Gwangju, Korea.
- Address reprint requests to: Keun-Bae Lee, M.D. Department of Orthopedic Surgery, Chonnam National University Hospital, 8, Hak-dong, Dong-gu, Gwangju 501-757, Korea. Tel: 82-62-227-1640, Fax: 82-62-225-7794, kbleeos@chonnam.ac.kr
Copyright © The Korean Fracture Society. All rights reserved
- 2,296 Views
- 12 Download
- 4 Crossref
- 1. Alldredge RH. Diastasis of the distal tibiofibular joint and associated lesions. JAMA, 1940;115:2136. Article
- 2. Beumer A, van Hemert WL, Niesing R, et al. Radiographic measurement of the distal tibiofibular syndesmosis has limited use. Clin Orthop Relat Res, 2004;423:227-234.Article
- 3. Blasier RD, Bucholz R, Cole W, Johnson LL, Mäkelä EA. Bioresorbable implants: applications in orthopaedic surgery. Instr Course Lect, 1997;46:531-546.
- 4. Boden SD, Labropoulos PA, McCowin P, Lestini WF, Hurwitz SR. Mechanical considerations for the syndesmosis screw. A cadaver study. J Bone Joint Surg Am, 1989;71:1548-1555.Article
- 5. Burwell HN, Charnley AD. The treatment of displaced fractures at the ankle by rigid internal fixation and early joint movement. J Bone Joint Surg Br, 1965;47:634-660.ArticlePDF
- 6. Clanton TO, Paul P. Syndesmosis injuries in athletes. Foot Ankle Clin, 2002;7:529-549.Article
- 7. Close JR. Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am, 1956;38:761-781.Article
- 8. Cotton F. The ankle and foot. Dislocations and jointfractures. Philadelphia, PA: WB Saunders; 1910. p. 535-588.
- 9. Cox S, Mukherjee DP, Ogden AL, et al. Distal tibiofibular syndesmosis fixation: a cadaveric, simulated fracture stabilization study comparing bioabsorbable and metallic single screw fixation. J Foot Ankle Surg, 2005;44:144-151.Article
- 10. Ebraheim NA, Lu J, Yang H, Mekhail AO, Yeasting RA. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a cadaver study. Foot Ankle Int, 1997;18:693-698.ArticlePubMedPDF
- 11. Edwards GS, DeLee JC. Ankle diastasis without fracture. Foot Ankle, 1984;4:305-312.ArticlePubMedPDF
- 12. Hoiness P, Stromsoe K. Tricortical versus quadricortical syndesmosis fixation in ankle fractures: a prospective, randomized study comparing two methods of syndesmosis fixation. J Orthop Trauma, 2004;18:331-337.PubMed
- 13. Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH. Syndesmosis sprains of the ankle. Foot Ankle, 1990;10:325-330.ArticlePDF
- 14. Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma, 2005;19:604-609.Article
- 15. Kaukonen JP, Lamberg T, Korkala O, Pajarinen J. Fixation of syndesmotic ruptures in 38 patients with a malleolar fracture: a randomized study comparing a metallic and a bioabsorbable screw. J Orthop Trauma, 2005;19:392-395.
- 16. Kukreti S, Faraj A, Miles JN. Does position of syndesmotic screw affect functional and radiological outcome in ankle fractures? Injury, 2005;36:1121-1124.Article
- 17. Lauge-Hansen N. Fractures of the ankle. III. Genetic roentgenologic diagnosis of fractures of the ankle. Am J Roentgenol Radium Ther Nucl Med, 1954;71:456-471.
- 18. Leeds HC, Ehrlich MG. Instability of the distal tibiofibular syndesmosis after bimalleolar and trimalleolar ankle fractures. J Bone Joint Surg Am, 1984;66:490-503.Article
- 19. Lund-Kristensen J, Greiff J, Riegels-Nielsen P. Malleolar fractures treated with rigid internal fixation and immediate mobilization. Injury, 1981;13:191-195.Article
- 20. Marsh JL, Saltzman DL. Ankle fractures. In: Bucholz RW, Heckman JD, editors. Rockwood and Green's fractures in adults. 6th ed. Philadelphia, PA: Linppincott Williams and Wilkins; 2006. p. 2147-2247.
- 21. Marti RK, Raaymakers EL, Nolte PA. Malunited ankle fractures. The late results of reconstruction. J Bone Joint Surg Br, 1990;72:709-713.ArticlePDF
- 22. McBryde A, Chiasson B, Wilhelm A, Donovan F, Ray T, Bacilla P. Syndesmotic screw placement: a biomechanical analysis. Foot Ankle Int, 1997;18:262-266.ArticlePDF
- 23. McConnell T, Creevy W, Tornetta P. Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am, 2004;86:2171-2178.Article
- 24. Michelson JD, Magid D, Ney DR, Fishman EK. Examination of the pathologic anatomy of ankle fractures. J Trauma, 1992;32:65-70.ArticlePubMed
- 25. Needleman RL, Skrade DA, Stiehl JB. Effect of the syndesmotic screw on ankle motion. Foot Ankle, 1989;10:17-24.ArticlePubMedPDF
- 26. Nielson JH, Sallis JG, Potter HG, Helfet DL, Lorich DG. Correlation of interosseous membrane tears to the level of the fibular fracture. J Orthop Trauma, 2004;18:68-74.Article
- 27. Oae K, Takao M, Naito K, et al. Injury of the tibiofibular syndesmosis: value of MR imaging for diagnosis. Radiology, 2003;227:155-161.Article
- 28. Ogilvie-Harris DJ, Reed SC, Hedman TP. Disruption of the ankle syndesmosis: biomechanical study of the ligamentous restraints. Arthroscopy, 1994;10:558-560.Article
- 29. Pettrone FA, Gail M, Pee D, Fitzpatrick T, Van Herpe LB. Quantitative criteria for prediction of the results after displaced fracture of the ankle. J Bone Joint Surg Am, 1983;65:667-677.Article
- 30. Pneumaticos SG, Noble PC, Chatziioannou SN, Trevino SG. The effects of rotation on radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle Int, 2002;23:107-111.ArticlePDF
- 31. Rasmussen O, Tovborg-Jensen I, Boe S. Distal tibiofibular ligaments. Analysis of function. Acta Orthop Scand, 1982;53:681-686.Article
- 32. Snedden MH, Shea JP. Diastasis with low distal fibula fractures: an anatomic rationale. Clin Orthop Relat Res, 2001;382:197-205.
- 33. Takao M, Ochi M, Naito K, et al. Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy, 2001;17:836-843.ArticlePubMed
- 34. Tornetta P, Spoo JE, Reynolds FA, Lee C. Overtightening of the ankle syndesmosis: is it really possible? J Bone Joint Surg Am, 2001;83:489-492.ArticlePubMed
- 35. Wrazidlo W, Karl EL, Koch K. Arthrographic diagnosis of rupture of the anterior syndesmosis of the upper ankle joint. Rofo, 1988;148:492-497.PubMed
- 36. Yamaguchi K, Martin CH, Boden SD, Labropoulos PA. Operative treatment of syndesmotic disruptions without use of a syndesmotic screw: a prospective clinical study. Foot Ankle Int, 1994;15:407-414.ArticlePubMedPDF
- 37. Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg, 2007;15:330-339.ArticlePubMed
REFERENCES
Fig. 1
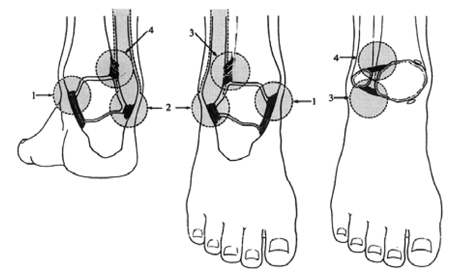
Ankle stabilizing structures are medial malleolus and deltoid ligament (1), lateral malleolus and lateral ligament complex (2), anterior syndesmosis and its bony attatchment (3) and posterior syndesmosis and its bony attatchment (4) (Adapted from Tile M. The rationale of operative fracture care, 2nd ed. New York, Springer: 523-561, 2007.).
Fig. 2
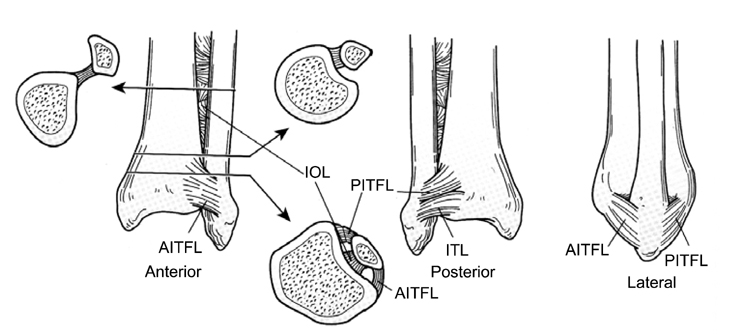
Anterior, posterior, and lateral views of select ligaments of the distal tibiofibular syndesmosis: the anterior-inferior tibiofibular ligament (AITFL); the posterior-inferior tibiofibular ligament (PITFL), of which the inferior transverse ligament (ITL) is part; and the interosseous ligament (IOL), which represents the thickened distal part of the interosseous membrane. The arrows indicate the respective location and point to the cross-sectional view (Adapted from Browner B, Jupiter J, Levine A, eds. Skeletal trauma: fractures, dislocations, and ligamentous injuries, 2nd ed. Philadelphia: WB Saunders, 1997.).
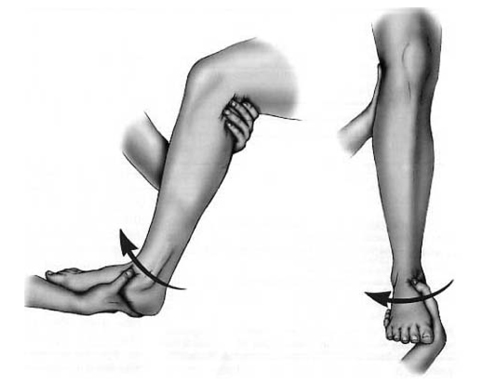
Fig. 3

Sqeeze test is performed by compressing fibula to tibia above midpoint of calf. Test is considered positive if proximal compression produces distal pain in interosseous ligaments or supporting structures (Adapted from Coughlin MJ, Mann RA, Saltzman CL. Surgery of the foot and ankle, 8th ed. Philadelphia: Mosby Elsevier, 2007.).
Fig. 4
External rotation test is performed by applying external rotation stress to involved foot and ankle while knee is held in 90 degrees of flexion and ankle is in neutral position. Positive test produces pain over anterior or posterior tibiofibular ligaments and over interosseous membrane (Adapted from Coughlin MJ, Mann RA, Saltzman CL. Surgery of the foot and ankle, 8th ed. Philadelphia: Mosby Elsevier, 2007.).
Fig. 5
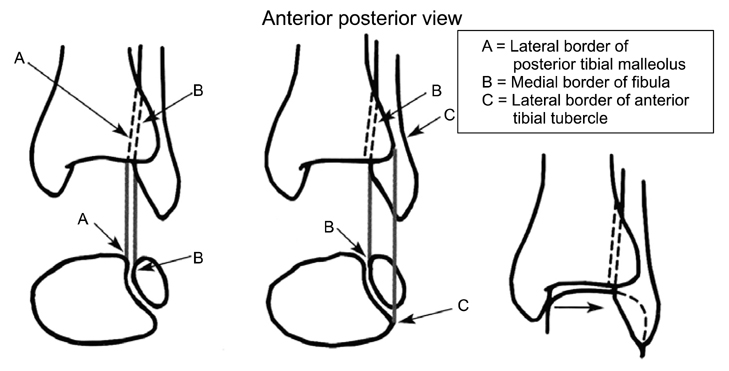
Normal syndesmotic relationships include a tibiofibular clear space (distance A-B) <6 mm in both the anteroposterior and mortise views, as well as a tibiofibular overlap (distance B-C) >6 mm or >42% of the width of the fibula on the anteroposterior view, or >1 mm on the mortise view. The overlap is measured 1 cm proximal to the plafond (Adapted from Coughlin MJ, Mann RA, Saltzman CL. Surgery of the foot and ankle, 8th ed. Philadelphia: Mosby Elsevier, 2007.).
Fig. 6
(A) The initial mortise radiograph shows unstable supination-external rotation stage IV ankle fracture with the widening of medial clear space and increased tibiofibular clear space.
(B) The photograph of a medial side of the ankle demonstrates ecchymosis and swelling.
(C) Arthroscopic view of medial gutter of the ankle shows tear of the deltoid ligament as seen from the anteromedial portal. Arthroscopic debridement and shrinkage with radiofrequency were performed.
(D) Arthroscopic view of the ankle syndesmosis shows diastasis which increased distal tibiofibular joint with arthroscopic shaver.
(E) Arthroscopic view shows syndesmotic reduction as seen from the anterolateral portal.
(F) Postoperative anteroposterior radiograph shows open reduction and internal fixation of fibula as well as syndesmotic stabilization with two 3.5 mm screws engaging four cortices.
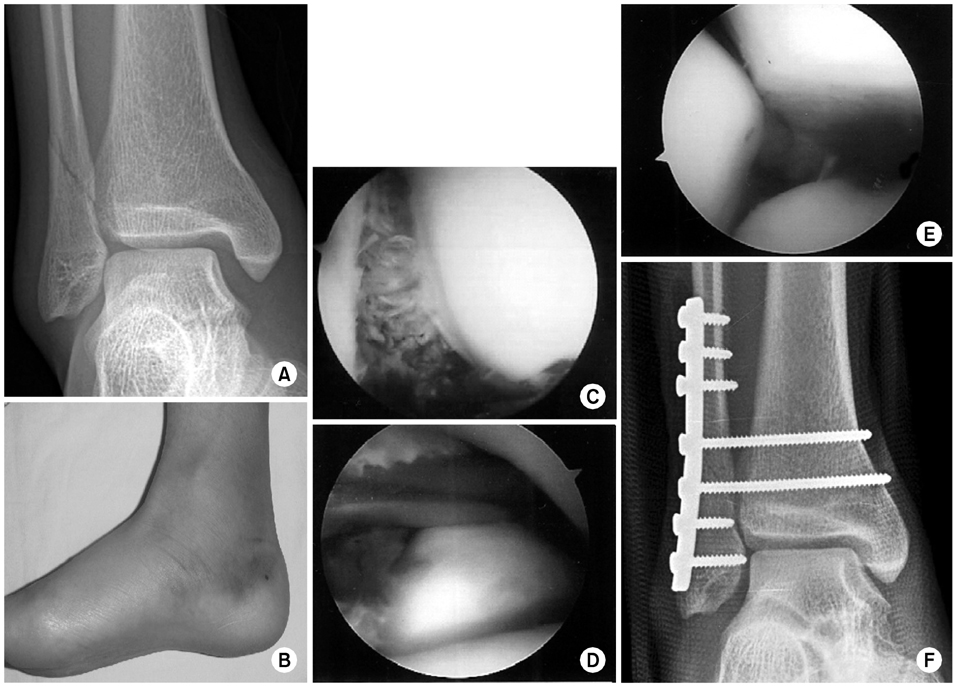
A 23-year-old man slipped and sustained a fracture of the ankle.
Fig. 7
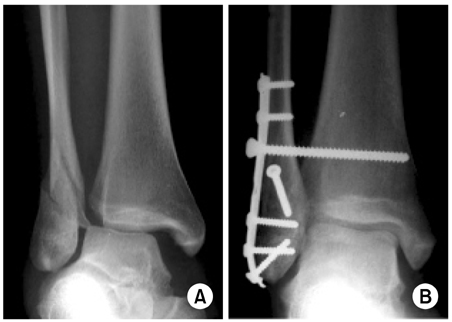
(A) Anteroposterior radiograph shows pronation-abduction stage III ankle fracture.
(B) Lateral radiograph shows posterior malleolar fracture.
(C) Postoperative anteroposterior radiograph shows accurate anatomical reduction and fixation of fracture. Syndesmotic transfixation screws were unnecessary because intraoperative evidence of syndesmotic disastasis is absent after fixation.

A 54-year-old woman sustained an inversion injury of ankle.
Fig. 8
(B) Syndesmosis fixation with a single 4.5 mm screw was performed (Adapted from Zalavras C, Thordarson D: Ankle syndesmotic injury. J Am Acad Orthop Surg, 15:330-339, 2007.).
(A) Anteroposterior radiograph demonstrates Weber type B supination-external rotation ankle fracture associated with disruption of the syndesmosis.
Fig. 9
(B) Syndesmosis fixation with two 4.5 mm screws was performed (Adapted from Zalavras C, Thordarson D: Ankle syndesmotic injury. J Am Acad Orthop Surg, 15:330-339, 2007.).
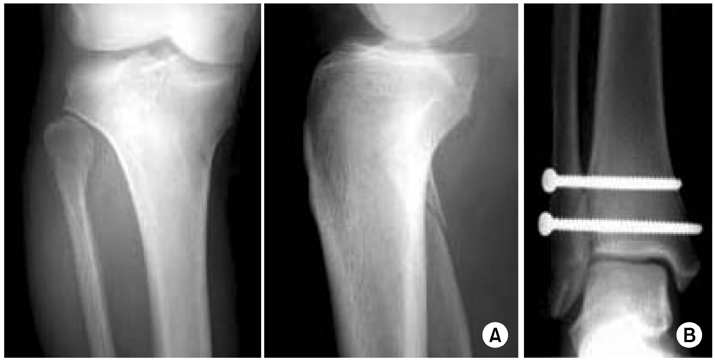
(A) Anteroposterior and lateral radiograph show the proximal fibula fracture (Maissonneuve) that was not stabilized.
Fig. 10
(A) Anteroposterior radiograph shows unstable pronation-external rotation stage IV ankle fracture with widening of medial clear space and increased tibiofibular clear space.
(B) Lateral radiograph demonstrates posterior malleolar fracture.
(C) Postoperative anteroposterior radiograph shows open reduction and internal fixation of fibula as well as syndesmotic stabilization with two 3.5 mm screws.
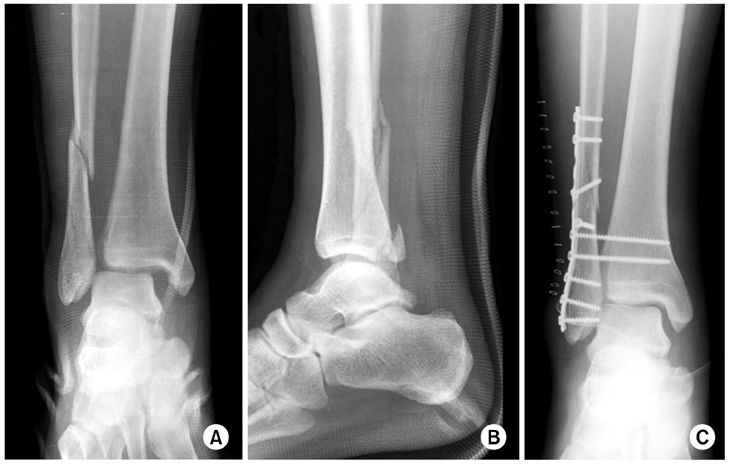
A 48-year-old man slipped and sustained a fracture of the ankle.
Fig. 11
(A) Incorrect angle for insertion of syndesmotic transfixation screw.
(B) In the transverse plane, the screw should follow a 30 degrees oblique direction from posterolateral to anteromedial.
(C) The fibula should be held reduced during screw placement. The screw may be inserted through a fibular plate or outside of the plate (From Heim U, Pfeiffer KM: Small fragment set manual: Technique recommended by the ASIF group, 2nd ed. Berlin, Springer-Verlag, 1975.).
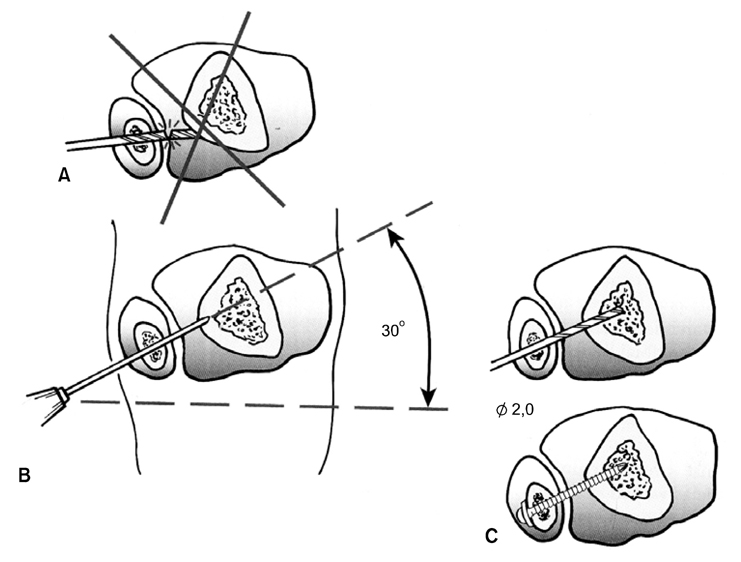
Proper placement of a syndesmotic screw.
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Radiologic consideration of acute ankle sprains: diagnostic imaging
Dong-Il Chun, Seung Lim Baek, Sung Hun Won
Arthroscopy and Orthopedic Sports Medicine.2024; 11(2): 39. CrossRef - Removal of broken syndesmotic screw with minimal bone defects in Korea: a case report
Min Gyu Kyung, Chulhee Park
Journal of Trauma and Injury.2023; 36(3): 265. CrossRef - Treatment of Ankle Fracture and Dislocation
Chan Kang
Journal of the Korean Fracture Society.2022; 35(1): 38. CrossRef - Isolated Syndesmotic Injury
Yong Tae Kim, Hyong Nyun Kim, Yong Wook Park
Journal of Korean Foot and Ankle Society.2016; 20(3): 100. CrossRef
 Cite
CiteAnkle Syndesmotic Injury
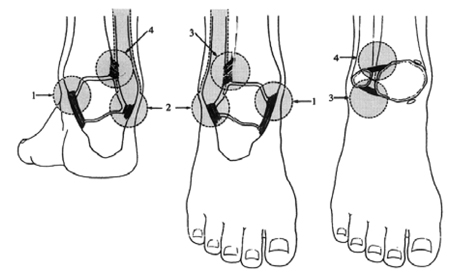
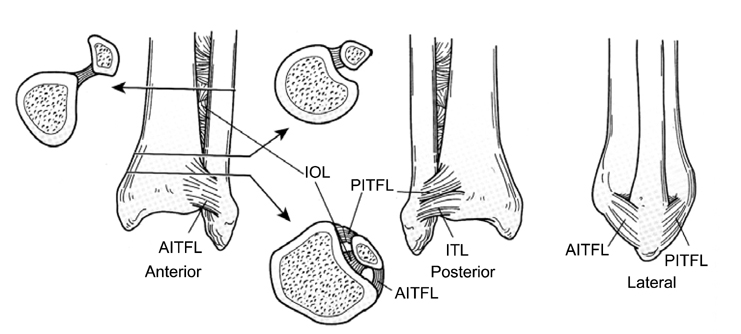

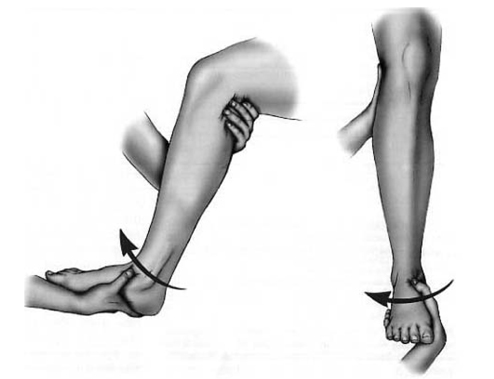
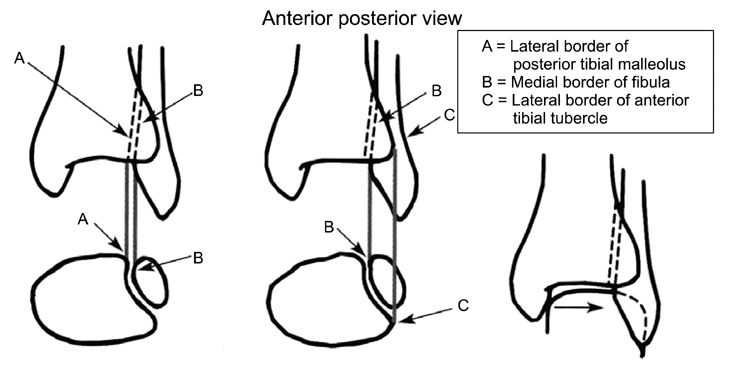


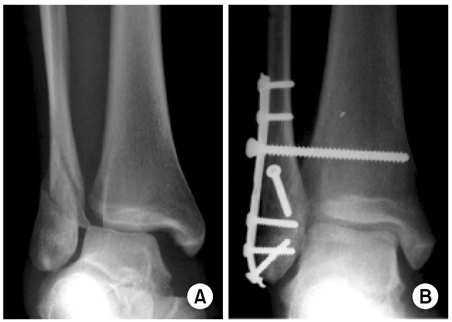

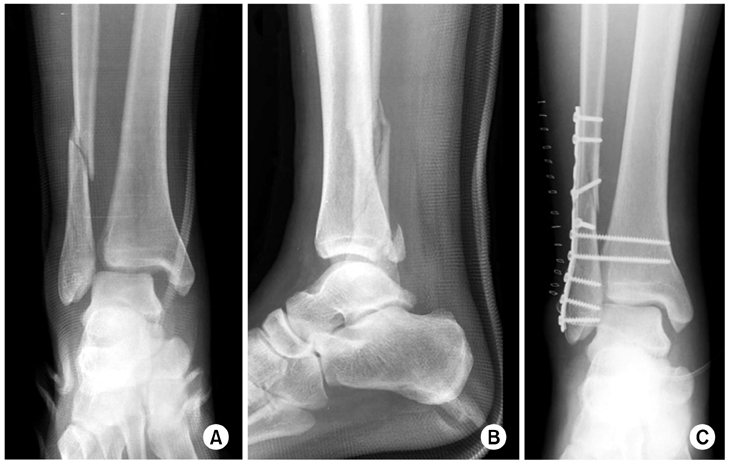
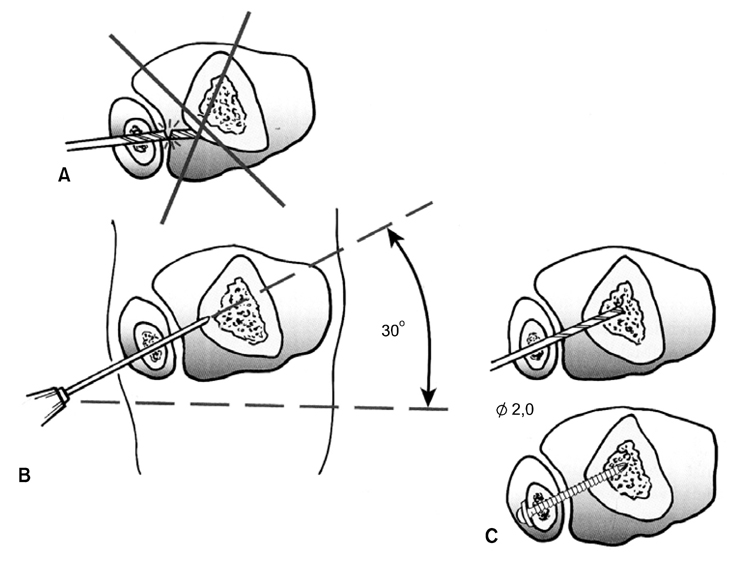
Fig. 1
Ankle stabilizing structures are medial malleolus and deltoid ligament (1), lateral malleolus and lateral ligament complex (2), anterior syndesmosis and its bony attatchment (3) and posterior syndesmosis and its bony attatchment (4) (Adapted from Tile M. The rationale of operative fracture care, 2nd ed. New York, Springer: 523-561, 2007.).
Fig. 2
Anterior, posterior, and lateral views of select ligaments of the distal tibiofibular syndesmosis: the anterior-inferior tibiofibular ligament (AITFL); the posterior-inferior tibiofibular ligament (PITFL), of which the inferior transverse ligament (ITL) is part; and the interosseous ligament (IOL), which represents the thickened distal part of the interosseous membrane. The arrows indicate the respective location and point to the cross-sectional view (Adapted from Browner B, Jupiter J, Levine A, eds. Skeletal trauma: fractures, dislocations, and ligamentous injuries, 2nd ed. Philadelphia: WB Saunders, 1997.).
Fig. 3
Sqeeze test is performed by compressing fibula to tibia above midpoint of calf. Test is considered positive if proximal compression produces distal pain in interosseous ligaments or supporting structures (Adapted from Coughlin MJ, Mann RA, Saltzman CL. Surgery of the foot and ankle, 8th ed. Philadelphia: Mosby Elsevier, 2007.).
Fig. 4
External rotation test is performed by applying external rotation stress to involved foot and ankle while knee is held in 90 degrees of flexion and ankle is in neutral position. Positive test produces pain over anterior or posterior tibiofibular ligaments and over interosseous membrane (Adapted from Coughlin MJ, Mann RA, Saltzman CL. Surgery of the foot and ankle, 8th ed. Philadelphia: Mosby Elsevier, 2007.).
Fig. 5
Normal syndesmotic relationships include a tibiofibular clear space (distance A-B) <6 mm in both the anteroposterior and mortise views, as well as a tibiofibular overlap (distance B-C) >6 mm or >42% of the width of the fibula on the anteroposterior view, or >1 mm on the mortise view. The overlap is measured 1 cm proximal to the plafond (Adapted from Coughlin MJ, Mann RA, Saltzman CL. Surgery of the foot and ankle, 8th ed. Philadelphia: Mosby Elsevier, 2007.).
Fig. 6
A 23-year-old man slipped and sustained a fracture of the ankle.
(A) The initial mortise radiograph shows unstable supination-external rotation stage IV ankle fracture with the widening of medial clear space and increased tibiofibular clear space.
(B) The photograph of a medial side of the ankle demonstrates ecchymosis and swelling.
(C) Arthroscopic view of medial gutter of the ankle shows tear of the deltoid ligament as seen from the anteromedial portal. Arthroscopic debridement and shrinkage with radiofrequency were performed.
(D) Arthroscopic view of the ankle syndesmosis shows diastasis which increased distal tibiofibular joint with arthroscopic shaver.
(E) Arthroscopic view shows syndesmotic reduction as seen from the anterolateral portal.
(F) Postoperative anteroposterior radiograph shows open reduction and internal fixation of fibula as well as syndesmotic stabilization with two 3.5 mm screws engaging four cortices.
Fig. 7
A 54-year-old woman sustained an inversion injury of ankle.
(A) Anteroposterior radiograph shows pronation-abduction stage III ankle fracture.
(B) Lateral radiograph shows posterior malleolar fracture.
(C) Postoperative anteroposterior radiograph shows accurate anatomical reduction and fixation of fracture. Syndesmotic transfixation screws were unnecessary because intraoperative evidence of syndesmotic disastasis is absent after fixation.
Fig. 8
(A) Anteroposterior radiograph demonstrates Weber type B supination-external rotation ankle fracture associated with disruption of the syndesmosis.
(B) Syndesmosis fixation with a single 4.5 mm screw was performed (Adapted from Zalavras C, Thordarson D: Ankle syndesmotic injury. J Am Acad Orthop Surg, 15:330-339, 2007.).
Fig. 9
(A) Anteroposterior and lateral radiograph show the proximal fibula fracture (Maissonneuve) that was not stabilized.
(B) Syndesmosis fixation with two 4.5 mm screws was performed (Adapted from Zalavras C, Thordarson D: Ankle syndesmotic injury. J Am Acad Orthop Surg, 15:330-339, 2007.).
Fig. 10
A 48-year-old man slipped and sustained a fracture of the ankle.
(A) Anteroposterior radiograph shows unstable pronation-external rotation stage IV ankle fracture with widening of medial clear space and increased tibiofibular clear space.
(B) Lateral radiograph demonstrates posterior malleolar fracture.
(C) Postoperative anteroposterior radiograph shows open reduction and internal fixation of fibula as well as syndesmotic stabilization with two 3.5 mm screws.
Fig. 11
Proper placement of a syndesmotic screw.
(A) Incorrect angle for insertion of syndesmotic transfixation screw.
(B) In the transverse plane, the screw should follow a 30 degrees oblique direction from posterolateral to anteromedial.
(C) The fibula should be held reduced during screw placement. The screw may be inserted through a fibular plate or outside of the plate (From Heim U, Pfeiffer KM: Small fragment set manual: Technique recommended by the ASIF group, 2nd ed. Berlin, Springer-Verlag, 1975.).
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7
Fig. 8
Fig. 9
Fig. 10
Fig. 11
Ankle Syndesmotic Injury

